


1Department of Dermatology, Venereology and Allergology, 2Department of Histology and Embryology, Wroclaw Medical University, and 3Department of Physiotherapy, University School of Physical Education, Wroclaw, Poland
The aim of this study was to investigate the role of lym-phangiogenesis in the clinical progression and outcome of mycosis fungoides. Immunohistochemistry and Western blot techniques were used to assess the expression of podoplanin and vascular endothelial growth factor C in mycosis fungoides. Expression of vascular endothelial growth factor C measured by immunohistochemistry was significantly higher in mycosis fungoides samples in comparison with control cases (chronic benign dermatoses) (p = 0.0012). Increased expression of podoplanin was found in advanced vs. early mycosis fungoides (p < 0.0001), and was positively correlated with cutaneous and nodal involvement (p < 0.001, p < 0.0001; respectively). Higher podoplanin expression was also significantly
associated with shorter survival (p < 0.001). Strong posi-tive correlation was observed between expression of podoplanin analysed by immunohistochemistry and Western blot (r = 0.75, p < 0.0001). A similar association was shown regarding expression of vascular endothelial growth factor C (r = 0.68, p = 0.0007). In conclusion, these results suggest that increased expression of podoplanin is associated with poor clinical course, as well as shorter survival, of patients with mycosis fungoides.
Key words: mycosis fungoides; primary cutaneous T-cell lymphoma; lymphangiogenesis; podoplanin; VEGF-C.
Accepted Aug 17, 2016; Epub ahead of print Aug 22, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, University of Medicine, Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Mycosis fungoides (MF) is the most common form of primary cutaneous T-cell lymphoma, accounting for approximately 50% of cases (1). It arises in peripheral T lymphocytes and is characterized by a relatively benign remitting/relapsing course. Initially, MF develops solely in the skin, evolving through consecutive stages, from patches through plaques to tumours, often ulcerated. The disease can also occur in the erythrodermic form, in which inflammation of the skin covers more than 80% of the body surface area. In some cases, the disease manifests aggressive behaviour, disseminating to the lymph nodes and internal organs. The distinctive nature of MF is reflected in the current staging system, in which special attention has been paid to the character and extent of the skin lesions (2). Despite numerous studies over the last decades, the aetiology of MF is not fully understood, but, similarly to solid tumours and other haematological malignancies, recent studies suggest the involvement of lymphangiogenesis in the development and progression of the disease.
Lymphangiogenesis is a multistep process of formation of new lymphatic vessels from the existing vascular network through extension and branching in response to local stimulation (3). It plays a significant role in physiological processes, mainly during embryogenesis, the ovarian cycle and gestation. However, it is also fundamental for metastasis of malignancies (4). The importance of this process in the dissemination of malignant neoplasms has been suggested due to the discovery of specific markers of lymphatic vessels. Among them, a highly O-glycosylated mucin-like transmembrane glycoprotein, podoplanin (PDPN), is commonly used in lymphatic vasculature assessment. PDPN is involved in the processes of adhesion and migration of endothelial cells, and its expression is observed on lymphatic endothelium. Moreover, physiologically its expression has been found in osteocytes, peritoneal mesothelial, glandular myoepithelial, and ependymal cells, as well as in stromal reticular and follicular dendritic cells of lymphoid organs. Expression in oncological lesions was shown in breast, oesophageal and testicular cancer, as well as in germ cell tumours (5–8).
Numerous lines of evidence indicate an important role of the family of vascular endothelial growth factors (VEGF) in lymphangiogenesis. The VEGF family consists of 6 proteins: VEGF-A, -B, -C, -D, -E, and placental growth factor (PGF), of which, the most potent stimulator of lymphangiogenesis is VEGF-C (9). VEGF-C promotes proliferation, migration and survival of lymphatic endothelial cells through a specific transmembrane receptor VEGFR-3/FLT4 (10, 11). Many recent studies have revealed a strong association between VEGF-C expression and clinicopathological data, i.e. grade of histological malignancy, progression, dissemination as well as prognosis of the disease (12–15). In breast, prostate and colon cancer increased expression of VEGF-C correlated with high lymphatic vessel density (LVD) and poor survival (16–21). In haematological malignancies, increased lymphangio-genesis was found to be correlated with aggressiveness and poor clinical outcome of lymphoma (22, 23).
In studies on lymphangiogenesis in lymphoproliferative disorders relatively little attention was paid to primary cutaneous T-cell lymphomas (CTCL). Therefore, using immunohistochemical (IHC) and molecular methods (Western blot; WB), we evaluated the expression of VEGF-C and PDPN, important markers of lymph-angiogenesis, in relation to clinicopathological data and their potential impact on patients’ outcomes in MF.
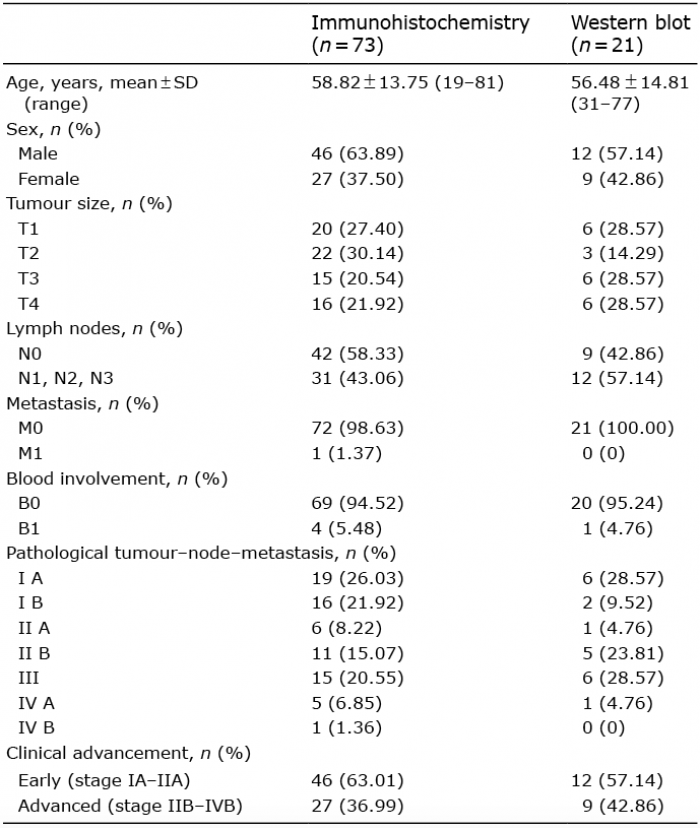
The material for the IHC comprised 73 paraffin-embedded samples obtained from patients with MF diagnosed and treated in the Department of Dermatology, Venereology and Allergology (Wroclaw Medical University) in the period 1994–2015. The diagnosis was established and re-evaluated based on clinical, histopathological and IHC examinations, according to the World Health Organization (WHO) classification (2008) (1). The staging was assessed according to TNMB (Tumour, Nodes, Metastases, Blood) system (ISCL/EORTC revision) presented in our previous study (24). To examine potential differences between benign and malignant skin conditions chronic benign dermatitis paraffin samples (16 lichen planus, 3 disseminated eczema cases) were used as a control. Moreover, skin biopsies were collected from 21 patients with MF and 4 with benign dermatoses and stored at –80°C in order to perform WB analysis. The material for WB was obtained simultaneously from the same lesions as those for IHC study. The study was approved by the ethics committee of Wroclaw Medical University (approval number KB 574/2011). All patients’ clinicopathological data are shown in Table I.
Table I. Clinicopathological data
All reactions were performed on 4-µm-thick paraffin sections. In order to examine the expression of PDPN, a protocol using Dako Autostainer Link48 (Dako, Glostrup, Denmark) was introduced. Deparaffinization, rehydration and unmasking the antigens was conducted by boiling in EnVision FLEX Target Retrieval Solution (pH 9, 20 min, 97°C; Dako) using Pre-Treatment Link platform (Dako). Activity of endogenous peroxidase was blocked by 5 min incubation in EnVision FLEX Peroxidase-Blocking Reagent (Dako). Sections were incubated with the primary monoclonal mouse anti-human PDPN antibody (clone D2-40, RTU, catalogue number: IR072; Dako) for 20 min at room temperature (RT). Following this EnVision FLEX /HRP – secondary antibodies were applied (20 min at RT; Dako). Diaminobenzidine (DAB, Dako) was utilized as the peroxidase substrate and the sections were incubated for 10 min at RT. In order to examine the expression of VEGF-C manual protocol was performed. The sections were deparaffinized in xylene, rehydrated and boiled in a citrate buffer, pH 6. Subsequently, endogenous peroxidase was blocked using 3% H2O2 (5 min, RT). The sections were incubated with primary mouse antibody anti-VEGF-C (1:100, catalogue number: 101-M90; ReliaTech GmbH, Wolfenbüttel, Germany) for 18 h at 4°C. The next reaction stages were conducted according to the manufacturer’s instructions for the LSAB+ System-HRP visualization system (Dako). All slides were counterstained with EnVision FLEX Hematoxylin (Dako). Subsequently, the preparations were mounted in Mounting Medium (Dako).
All sections were evaluated using a BX-41 light microscope (Olympus, Tokyo, Japan) by 2 pathologists who were blinded to the patients’ clinical data. In doubtful cases, a re-evaluation with a double-headed microscope was performed until a consensus was achieved. PDPN expression was observed in a cytoplasm of lymphatic vessels endothelial cells. Initially, whole slide was determined as follows: the sections were first scanned at low power (×40 and ×100 magnification) to identify the hot-spots (areas of potentially highest lymphatic vessel density) as it is used in the microvessel density (LVD) count. Subsequently, these areas were examined under ×200 magnification using a Chalkley Point Array graticule (Pyser Sgi., Edenbridge, UK). The Chalkley count was regarded as the number of grid points that hit stained vessels. A mean score was determined for 3 hot-spots. Expression of VEGF-C was conducted using the semiquantitative immunoreactive score (IRS) of Remmele and Stegner, which is based on the intensity of the colour reaction and the percentage of positive neoplastic cells in the whole slide (25). The scale takes into account the percentage of cells with positive reaction (0 points: absence of cells with positive reaction, 1 point: 1–10% cells, 2 points: 11–50%, 3 points: 51–80%, 4 points: over 80% cells with positive reaction) as well as intensity of the reaction (0 points: no reaction, 1 points: low, 2 points: moderate, and 3 points: strong intensity of colour reaction). The product of both these parameters comprises the final score, ranging from 0 to 12 points.
Frozen samples were thawed in CellLytic MT Cell Lysis Solution (SigmaAldrich, Munich, Germany) with the addition of protease inhibitors, Benzonase – 50 U/ul (Merck; Millipore, Bedford, MA, USA) and 0.2 mM phenylmethanesulfonyl fluoride (PMSF; SigmaAldrich). Protein concentrations of whole-cell lysates were determined by bicinchoninic acid (BCA) assay (Pierce, Rockford, IL, USA). Equal amounts of total protein (30 μg) were mixed with sample buffer and dithiothreitol (DTT) and resolved by sodium dodecyl sulphate – polyacrylamide gel electrophoresis (SDS-PAGE). After completion of the electro-phoresis, the samples were transferred to polyvinylidene difluoride (PVDF) membranes (Immobilon; Millipore) and incubated in a 4% bovine serum albumin (BSA) solution in Tris-buffered saline (TBS) with the addition of 0.1% Tween-20. Subsequently, the membranes were incubated with rabbit anti-human VEGF-C antibody – 1:500 (AP2042c; Abgent, San Diego, CA, USA) and rabbit anti-human PDPN antibody – 1:750 (11629-1-AP; Proteintech Europe, Manchester, UK) for a night at 4°C. At the end the membranes were treated with the peroxidase-conjugated donkey anti-rabbit secondary antibody – 1:3,000 (711-035-152; Jacksons Immunoresearch, Suffolk, UK) for 1 h, rinsed, and incubated with the Luminata Classico Western HRP Substrate (Merck) overnight. Protein quantifications were based on the total protein normalization with the use of the TGX Stain Free FastCast Acrylamide Kit (Bio-Rad, Hercules, CA, USA). Protein separation was visualized on the gels after electrophoresis and analysed by using Image Lab 5.0 Software (Bio-Rad) and ChemiDock MP System (Bio-Rad).
Shapiro-Wilk test was used to evaluate the normality assumption of examined groups. To compare the differences between the expression of examined markers in the all patients’ pairs of groups and clinicopathological data the unpaired t-test and Mann–Whitney test were used. To compare the differences between more than 2 groups the Kruskal–Wallis and Dunn’s multiple comparison test was performed. In addition, the Spearman’s correlation test was used to analyse the existing correlations. The Kaplan–Meier method was used to construct survival curves. To evaluate the analysis of survival Mantel–Cox test was performed. A Cox proportional hazards model with forward stepwise selection was used to calculate univariate and multivariate hazard ratio for the study variables. All statistical analyses were performed using Prism 5.0 (GraphPad, La Jolla, CA, USA) and Statistica 10 (StatSoft Inc. Tulsa, OK, USA). The results were considered as statistically significant when p < 0.05.
Immunohistochemical expression of PDPN and VEGF-C was observed in 71 out of 73 cases of MF and in 18 out of 19 control cases. Expression of PDPN was observed in the cytoplasm of endothelial cells of lymphatic vessels (Fig. 1A, B), whereas VEGF-C expression was found in the cytoplasm of atypical T cells (Fig. 1C, D). The IHC expression of PDPN was higher in MF than in the control group; however, it did not reach statistical significance (p = 0.07; Mann-Whitney test, Fig. 2A). On the other hand, when comparing the chronic benign dermatoses and advanced MF group significantly higher expression was present in the latter (p < 0.0001; Mann-Whitney test; Fig. 2B). The expression of VEGF-C was significantly higher in MF samples compared with the control group (p = 0.0012, Mann–Whitney test; Fig. 2C). VEGFC was increased in both early and advanced cases compared with the control group (both p < 0.01, Mann-Whitney test; Fig. 2D).
Fig. 1. Immunohistochemical expression of (A, B) podoplanin in cytoplasm of endothelial cells of lymphatic vessels, and (C, D) expression of vascular endothelial growth factor C, with (C) moderate and (D) strong cytoplasmic localization in neoplastic cells in patients with mycosis fungoides. Original magnification × 200.
Fig. 2. Comparison of immunohistochemical expression of podoplanin (PDPN) with regard: to (A) disease presence and (B) clinical advancement. Comparison of immunohistochemical expression of vascular endothelial growth factor-C (VEGF-C) with regard to (C) disease presence and (D) clinical advancement. MF: mycosis fungoides; IHC: immunohistochemistry, early MF – stage IA–IIA; advanced MF – stage IIB–IVB. **p < 0.01, ****p < 0.0001, Mann–Whitney test.
Regarding advancement of the disease, increased PDPN expression was found in advanced vs. early MF (p < 0.0001; Mann–Whitney test; Fig. 2B). PDPN expression increased with more infiltrated cutaneous lesions (tumours, stage T3) and with more extensive skin involvement (erythroderma, stage T4, compared with less infiltrated skin changes with the limited involvement of the body surface (patches and plaques, stages T1, T2) (p = 0.0004, p = 0.0014, respectively, Mann-Whitney test; Fig. 3A, B). Moreover, higher PDPN expression was associated with nodal involvement, N1-3 vs. N0 (p < 0.0001; Mann–Whitney test; Fig. 3C). Evident trend of increased PDPN expression was found in higher stages of MF clinical advancement (Mann–Whitney test; Fig. 3D). In contrast, no association between VEGF-C expression and disease advancement, extracutaneous involvement as well as staging in MF was disclosed.
Fig. 3. Comparison of immunohistochemical expression of podoplanin (PDPN) with regard to: (A, B) skin involvement, (C) nodal involvement, and (D) staging. MF: mycosis fungoides; IHC: immunohistochemistry. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001; Mann–Whitney test.
To confirm the results obtained by IHC, expression of PDPN and VEGF-C in frozen samples of MF and control cases (21 and 4 samples, respectively) was assessed using the WB technique (Fig. 4). WB expression of PDPN and VEGFC proteins was observed in all MF and control cases. Slightly higher expression of both studied markers was found in the MF group, albeit not reaching statistical significance (Fig. 5). In addition, no associations were found between expression of both examined proteins and clinicopathological data of MF (data not shown). Nevertheless, strong positive correlation between PDPN expression analysed by IHC and WB was observed (r = 0.75, p < 0.0001, Spearman’s rank correlation test; Fig 6A). Similar association regarding VEGF-C expression was shown (r = 0.68, p = 0.0007, Spearman’s rank correlation test; Fig. 6B). Analysing mutual correlations between the IHC expression of studied markers, a strong positive correlation between PDPN and VEGF-C was found (r = 0.70, p < 0.0001; Spearman’s rank correlation test; Fig. 6C). Correlation between PDPN and VEGF-C analysed by WB did not reach statistical significance (r = 0.38, p = 0.083, Spearman’s rank correlation test; Fig. 6D).
Fig. 4. Sample results of Western blot analysis of vascular endothelial growth factor C (VEGF-C) and podoplanin (PDPN) expression in mycosis fungoides (MF) and control cases.
Fig. 5. Comparison of vascular endothelial growth factor C (VEGF-C) and podoplanin (PDPN) expression in Western blot (WB) analysis with regard to disease presence. MF: mycosis fungoides.
Fig. 6. Spearman’s rank correlation plots presenting associations between expressions of podoplanin (PDPN) and vascular endothelial growth factor C (VEGF-C) analysed by immunohistochemistry (IHC) and Western blot (WB) technique: (A) PDPN WB vs. PDPN IHC (r = 0.75, p < 0.0001), (B) VEGF-C WB vs. VEGF-C IHC (r = 0.68, p = 0.0007), (C) VEGF-C IHC vs. PDPN IHC (r=0.70, p < 0.0001) and (D) VEGF-C WB vs. PDPN WB (r = 0.38, p = 0.083) in patients with mycosis fungoides.
Univariate analysis using the Mantel-Cox test revealed that, in 73 patients tested, higher PDPN expression was significantly associated with shorter overall survival (OS; Fig. 7A). Regarding VEGF-C, increased expression of this marker was also associated with shorter survival, albeit not reaching statistical significance (Fig. 7B). Univariate and multivariate Cox regression model analysis is shown in Table II.
Fig. 7. Analysis of survival in the mycosis fungoides group according to (A) immunohistochemical expression of podoplanin (PDPN) and (B) vascular endothelial growth factor C (VEGF-C). **p < 0.001, Mantel-Cox test.
Table II. Univariate and multivariate Cox regression model analysis of survival in mycosis fungoides
So far, only a few studies have analysed the process of lymphangiogenesis in CTCL. The current study demonstrated that higher PDPN expression is significantly correlated with disease progression and shorter survival in MF. First, we noticed the increased PDPN expression in MF compared with the control group, albeit not reaching statistical significance. However, the significantly higher PDPN expression was found in advanced MF while comparing with chronic benign dermatitis. Numerous data indicate the close association between lymphangiogenesis and chronic inflammation. In the skin, the increased expression of VEGF-C and enhanced LVD measured utilizing antibodies against PDPN was observed in cutaneous lichen planus, psoriasis and atopic eczema (26, 27). MF lesions, especially in the early stages, are characterized by mixed infiltration consisting of malignant lymphocytes mingled with reactive cells. Our data suggest, however, more pronounced process of lymphangiogenesis in the course of malignancy than in inflammation.
Secondly, we found an association between disease progression and PDPN expression. Advanced cases of MF were characterized by increased marker expression compared with early cases. Expression of PDPN also correlated with skin and nodal involvement. Increased lymphatic vascularization has been found in more infiltrated as well as in more extensive cutaneous lesions (tumours vs. patches and plaques, erythroderma vs. patches and plaques). Our results are consistent with accumulated lines of evidence that strongly suggest the role of tumour-induced lymphangiogenesis in progression and metastasis of various cancers, i.e. prostate adenocarcinoma, oesophageal squamous cell carcinoma, gastric, breast and lung cancer (28–32). Considering haematological malignancies, positive correlation between increased number of PDPN-positive vessels and disease progression was reported in Sézary syndrome, the most common, aggressive CTCL (33). Increased LVD was also associated with aggressive histology in non-Hodgkin’s lymphomas (NHL) (23).
Our study has also revealed increased expression of the key lymphangiogenesis factor, VEGF-C, in MF compared with the control group. VEGF-C overexpression was also observed in Sézary syndrome in the IHC study of Karpova et al. (33). In further analysis, we observed comparable levels of VEGF-C expression in early as well as in advanced stages, suggesting that VEGF-C could play a role on the subsequent steps of disease initiation and progression. Analogously, comparable expression level of another VEGF family member, VEGF-A, was observed in early and advanced disease in the skin biopsy tissue obtained from patients with MF (34). According to the authors, VEGF-A overexpression observed in all disease stages should be considered as an inner phenomenon associated with MF development. This hypothesis could be also applicable to the role of VEGF-C in MF.
A number of studies has documented VEGF-C expression in tumour cells, inflammatory cells and tumour-associated fibroblasts in primary human tumours and their stroma. IHC analysis allowed us to locate the VEGF-C in the cytoplasm of the tumour cells. VEGF-C expression has been also observed in malignant T cells in the course of tumour progression in a xenograft mouse model of MF, and in the cells of suprabasal layers of the epidermis in another IHC study on the MF skin samples (33). Interestingly, in vitro study failed to detect VEGF-C in CTCL cells, while co-culture with malignant lymphocytes induced increased VEGF-C expression in fibroblasts, which implies the modulating effect of the tumour microenvironment on VEGF-C expression level in different cell types (35).
In the current study we observed a positive correlation between PDPN and VEGF-C expression. Our results are consistent with the report of Karpova et al., who found the same association in Sézary syndrome and erythrodermic MF (33). A positive correlation between VEGF-C, and PDPN expression was also reported in other malignancies, i.e. gastric and bladder cancer (17, 36).
Taking into account observed PDPN and VEGF-C expression in MF, the potential impact of lymphangiogenesis on the patients’ outcome was analysed. Increased expression of PDPN significantly correlated with shorter survival. Moreover, association between increased expression of VEGF-C and poor outcome was found, although it did not reach statistical significance. How-ever, this phenomenon may be due to the relatively small number of patients included in the study. Accumulated lines of evidence indicate the association between tumour lymphangiogenesis and poor survival in solid tumours, i.e. increased VEGF-C expression correlated with poor outcome in breast cancer, and enhanced LVD was associated with shorter survival in colon and gastric cancer (29, 37–39). Considering haematological malignancies, in a heterogeneous group of NHL, mainly diffuse large B-cell lymphoma (DLBCL) and follicular B-cell lymphoma as well as Hodgkin’s lymphomas, the LVD correlated with poor outcome (22). Another study revealed that increased expression of VEGF-C in blood and tumour tissue correlated with mortality and high International Prognostic Index score in patients with DLBCL (40). In Hodgkin’s lymphomas, Rueda et al. (41) found that higher tissue expression of VEGF-C was a negative prognostic factor and correlated with shorter progression-free survival.
In our study, the expression of VEGF-C and PDPN observed in the IHC study was confirmed utilizing WB technique. A strong correlation was found between the results of the IHC and WB analyses regarding both studied factors. However, in-depth analysis of the WB results did not show significant associations. Given the small sample size these findings are not surprising for us, but are a limitation of the study.
In summary, this study provides new data indicating the role of lymphangiogenesis in the progression, skin and nodal involvement of MF, as well providing evidence for potential future use of increased expression of PDPN as a predictor of shorter survival in patients with MF.
This work was financially supported by the National Science Center (decision no. DEC-2011/01/B/NZ4/01052).
The authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize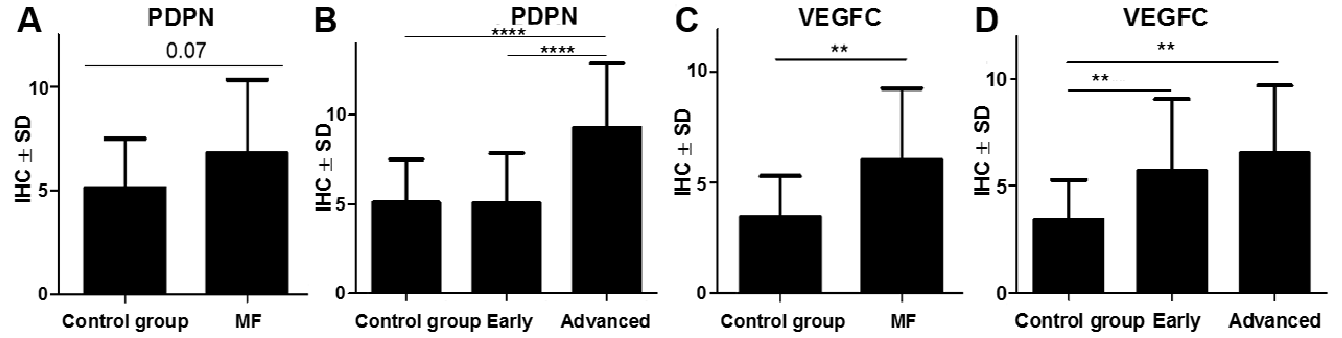 Click to show fullsize
Click to show fullsize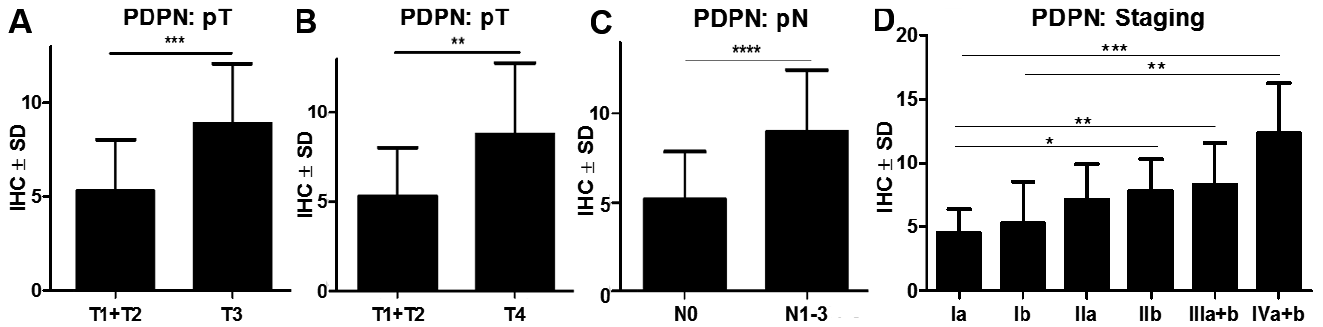 Click to show fullsize
Click to show fullsize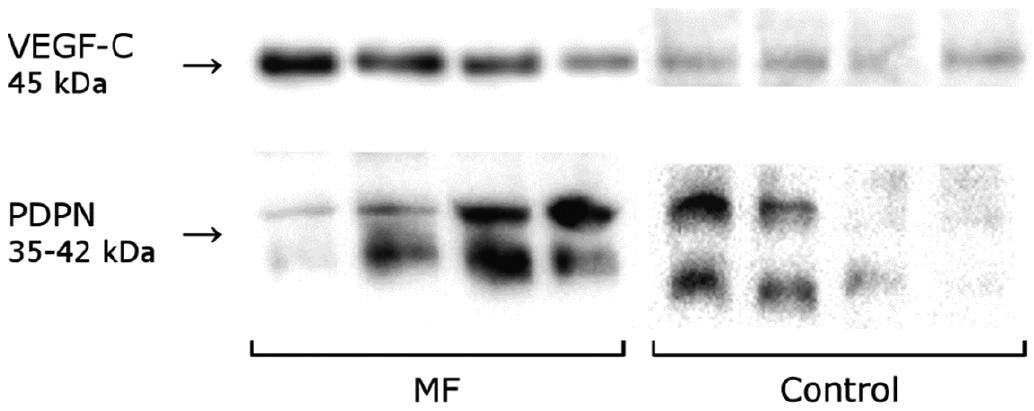 Click to show fullsize
Click to show fullsize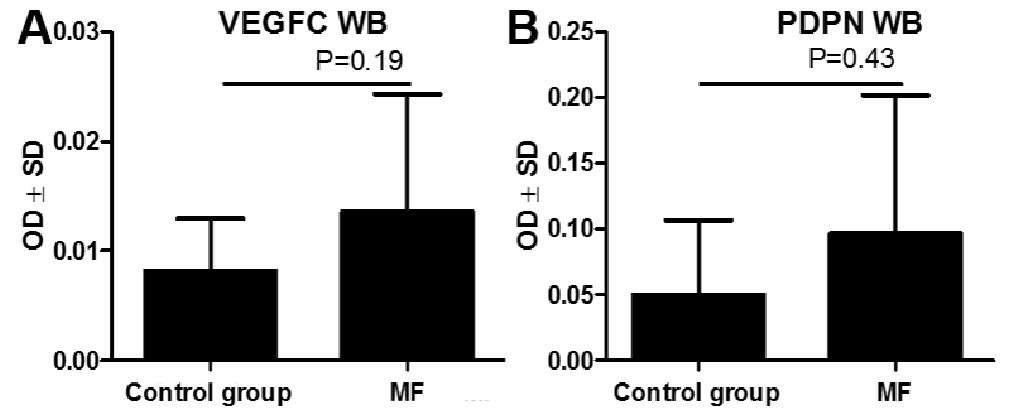 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize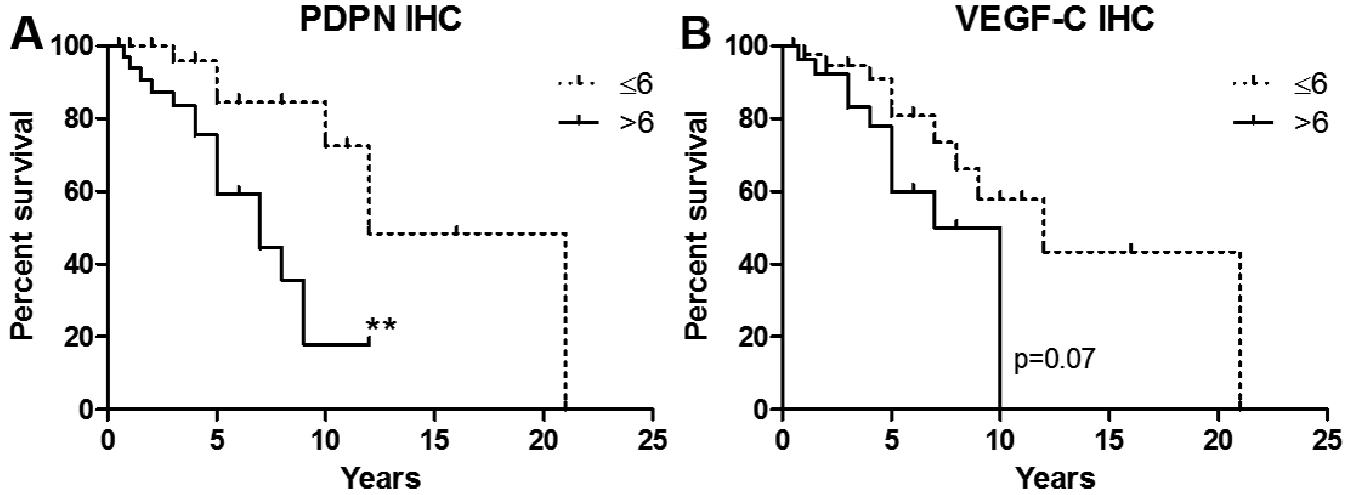 Click to show fullsize
Click to show fullsize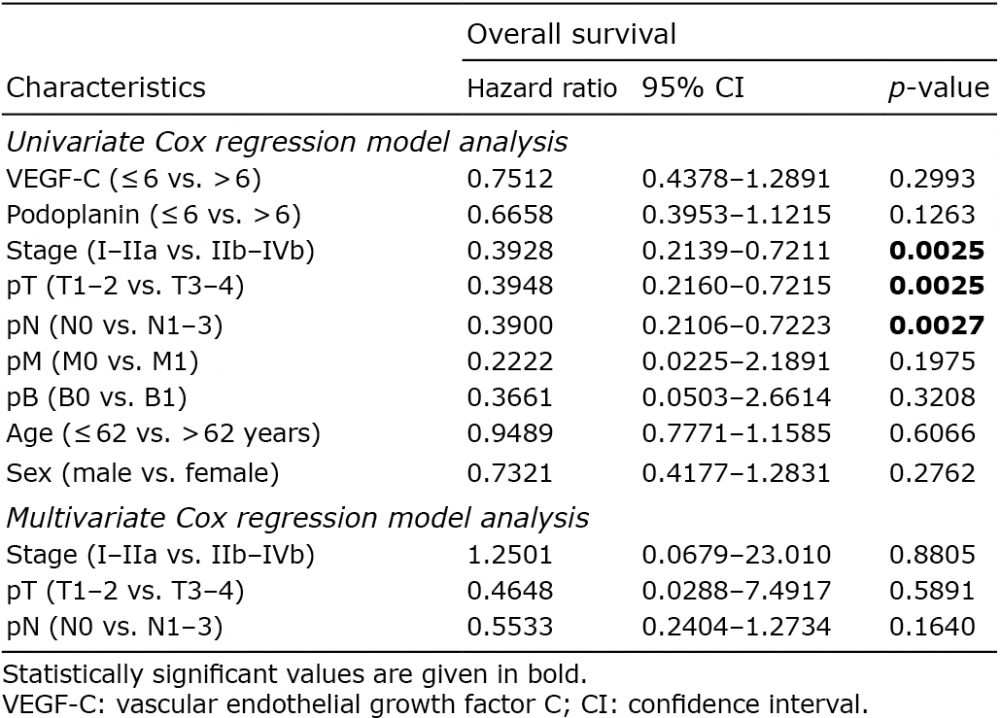 Click to show fullsize
Click to show fullsize