


1Department of Dermatology, Hokkaido University Graduate School of Medicine, North 15 West 7, Kita-ku, Sapporo 060-8638, 2Department of Dermatology, KKR Sapporo Medical Center, and 3Hiragishi Eye Clinic, Sapporo, Hokkaido, Japan. *E-mail: nomura@huhp.hokudai.ac.jp
Accepted Aug 17, 2016; Epub ahead of print Aug 22, 2016
Ophthalmic beta-adrenergic blockers, such as timolol, were first used in the treatment of glaucoma in the 1970s. Since then a range of systemic side-effects have been reported (1). However, the clinical characteristics of alopecia induced by timolol eye-drops are poorly understood. We describe here a challenging case of telogen effluvium due to topical administration of timolol eye-drops.
A 58-year-old Japanese man presented with a 1-month history of sudden hair loss. His medical history included glaucoma diagnosed 1 year previously. The patient was not on any oral medication. He did not report any weight loss or change in diet. A review of his systems did not reveal any other significant findings. Physical examination revealed asymptomatic diffuse alopecia on his scalp. Marked loss of the eyebrows and eyelashes was also noted, although the axillary and pubic hair were not affected. No nail pitting was observed. A hair-pull test resulted in several clubbed hairs. Trichoscopy showed no findings of alopecia areata, such as tapering hair, yellow spots or black dots. Thyroid dysfunction, collagen diseases, Treponema pallidum infection and zinc or iron deficiency were excluded by laboratory tests. Histopathological examination of the lesional skin from the scalp revealed numerous telogen hairs. These findings collectively suggested a diagnosis of telogen effluvium. At this point, however, we were unable to specify the cause. The patient then underwent gradual exacerbation of the disease, with almost all of his scalp hairs, eyebrows and eyelashes falling out within the next month.
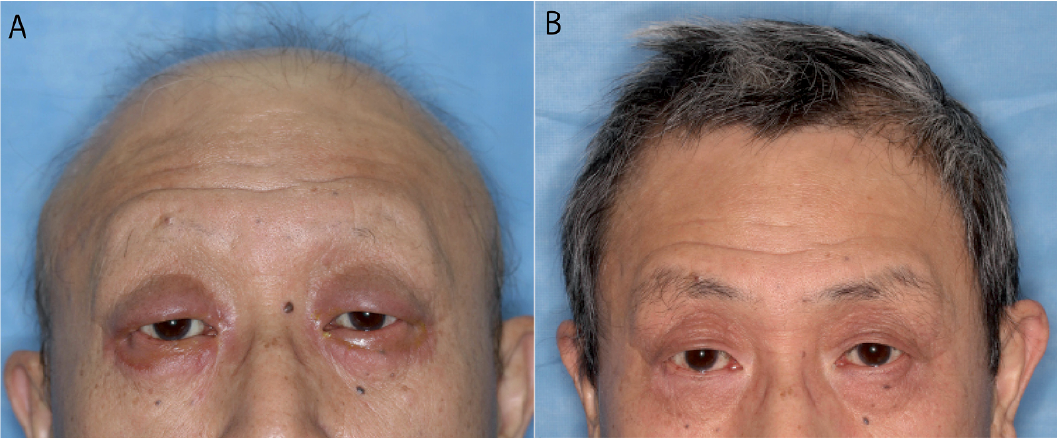
One month later, he developed itchy, well-demarcated swelling of the eyelids (Fig. 1A). Contact dermatitis induced by his prescription eye-drops was clinically suspected. He applied ophthalmic solutions of timolol, brimonidine, dorzolamide and bimatoprost daily to his eyes for bilateral open-angled glaucoma with advanced visual loss. A patch test for each of the eye-drops revealed the patient to be positive only for timolol, which strongly suggested that timolol was the cause of the contact dermatitis on his eyelids. A detailed medical interview revealed that he had been using the timolol eye-drops for 6 months before alopecia began. At this time, a review of the literature found that timolol eye-drops can cause drug-induced alopecia, especially telogen effluvium. We asked his ophthalmologist to discontinue the prescription for the timolol eye-drops. The contact dermatitis on his eyelids disappeared within one month of discontinuation of the timolol. Of particular note, partial regrowth of thin white hairs was also observed as an initial sign of improvement. Cessation of the timolol eye-drops, a key drug in the treatment of glaucoma, exacerbated his high intraocular pressure; however, selective laser trabeculoplasty was performed instead of timolol resumption and this lowered the pressure. Fourteen months after discontinuation of the timolol eye-drop, his scalp hairs, eyelashes and eyebrows had recovered to almost their original volumes and colour (Fig. 1B), which further confirmed the diagnosis of drug-induced telogen effluvium from timolol eye-drops.
Fig. 1. Alopecia caused by timolol eye-drops. (A) Diffuse alopecia before discontinuation of the timolol eye-drops. Note that severe contact dermatitis is also evident on the eyelids. (B) The scalp hairs, eyebrows and eyelashes are almost fully recovered at 14 months after discontinuation of the timolol eye-drops. Permission to publish these photos are given.
Drug-induced alopecia is mainly classified into anagen effluvium and telogen effluvium; the former is usually caused by chemotherapeutic agents, and the latter is caused by various drugs, such as mood stabilizers, antidepressants, anticoagulants, antimicrobials, antivirals and beta-adrenergic blockers (1–3). Telogen effluvium results in diffuse, non-scarring hair loss without signs of inflammation, due to an increased proportion of hairs shifting from the growth phase (anagen) to the shedding phase (telogen) (2). Since ophthalmic beta-adrenergic blockers enter the bloodstream through the lacrimal system and the conjunctival vessels, the blood levels of beta-adrenergic blockers can increase to a significant extent, which might induce systemic reactions even in ophthalmic usage (4). Indeed, 2 drops of 0.5% timolol eye-drops can cause blood concentrations equivalent to those of 10 mg oral timolol (4). Thus, systemic adverse reactions, such as cardiovascular, neurological, pulmonary, gastrointestinal and dermatological effects, including alopecia, have been described as side-effects of timolol (5). Although the US Food and Drug Administration states that alopecia is a possible side-effect of timolol eye-drops, only one report of timolol-induced telogen effluvium has been published in the English literature. In 1990, Fraunfelder et al. (6) briefly summarized cases of timolol-induced alopecia registered in the National Registry of Drug-Induced Ocular Side Effects with few clinical details of each case. Thus, this study should expand our understanding of telogen effluvium caused by timolol eye-drops. Observations from the very limited number of patients with timolol-induced telogen effluvium indicate that an abnormal number of hairs, especially scalp hairs, eyebrows and eyelashes, may start to shed 1–24 months after administration of the eye-drops (6), although further studies are warranted to verify this. The diagnosis should be carefully made by determining whether the chronology of causative drug exposure is compatible with the onset of alopecia and by ruling out other factors triggering telogen effluvium, such as iron, zinc and protein deficiencies, thyroid dysfunction, general anaesthesia and postpartum, all of which were excluded in our patient (1, 2).
The only treatment for drug-induced telogen effluvium is discontinuation of the causative drugs. It takes 3–6 months to observe initial regrowth of thin white hairs and 12–18 months for a cosmetically significant increase in hair volume (1). In this case, complete recovery from the alopecia required 14 months, which is consistent with the natural course of telogen effluvium. Although contact dermatitis on the eyelids gave us an opportunity to make a diagnosis of timolol-induced telogen effluvium in the present case, its association with alopecia is considered to be coincidental, because the hair loss had begun 2 months before the contact dermatitis.
Glaucoma is the leading cause of blindness worldwide. As the number of patients with glaucoma was estimated to be 64.3 million in 2013 and is projected to increase to 76.0 million by 2020, the prescription of ophthalmic beta-adrenergic blockers is expected to expand significantly (7). Physicians should be aware of systemic side-effects caused by ophthalmic solutions containing beta-adrenergic blockers. Seemingly harmless eye-drops containing beta-adrenergic blockers should be included in differential diagnoses when encountering alopecia with an unspecified cause.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize