


1Department of Psychology, University of Zaragoza and Aragon Health Sciences Institute, Zaragoza, Spain, 2Department of Consultation Liaison Psychiatry, Paris Descartes University, Sorbonne Paris Cité, Faculty of Medicine, 3Dermatologist and Psychoanalyst, Paris, France, Departments of Dermatology, 4Université Libre de Bruxelles, Erasme Hospital, Brussels, Belgium, 5University of Halle, Halle, Germany, 7Roskilde Hospital; Health Science Faculty, University of Copenhagen, Copenhagen, Denmark, 9Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands, 10Moscow State Medical University, Moscow, Russia, 6Oslo Centre for Biostatistics and Epidemiology, University of Oslo, Oslo, Norway, 8Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, and 11Department of Psychosomatic Medicine, Justus Liebig University, Giessen, Germany
The classification of self-inflicted skin lesions proposed by the European Society for Dermatology and Psychiatry
(ESDaP) group generated questions with regard to specific treatments that could be recommended for such cases. The therapeutic guidelines in the current paper integrate new psychotherapies and psychotropic drugs without forgetting the most important relational characteristics required for dealing with people with these disorders. The management of self-inflicted skin lesions necessitates empathy and a doctor–patient relationship based on trust and confidence. Cognitive behavioural therapy and/or psychodynamic and psychoanalytic psychotherapy (alone, or combined with the careful use of psychotropic drugs) seem to achieve the best results in the most difficult cases. Relatively new therapeutic techniques, such as habit reversal and mentalization-based psychotherapy, may be beneficial in the treatment of skin picking syndromes.
Key words: self-inflicted injury; skin picking disorder; psychological treatment; doctor–patient relationship; clinical practice guidelines.
Accepted Aug 22, 2016; Epub ahead of print Aug 26, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Lucía Tomas-Aragones, Department of Psychology, University of Zaragoza, Calle Pedro Cerbuna 12, ES-50009 Zaragoza, Spain. E-mail: ltomas@unizar.es
Self-harming behaviour has many aspects. In 2013, the European Society for Dermatology and Psychiatry (ESDaP) group (1) proposed a terminology and classification of self-inflicted skin lesions (SISL), which included several aspects of self-harm behaviour to the skin. Recent studies have indicated the acceptance of the classification with regard to therapeutic approaches to the treatment of patients with skin conditions (2). The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published in May 2013 (3), includes “skin picking” as a new category within the spectrum of obsessive-compulsive and related disorders. SISL have been described as a non-suicidal, conscious and direct damage to the skin (4–7).
In the previous classification paper from the ESDaP group, there was an explanation as to why SISL should not encompass all skin lesions attributed to pathological behaviour (1). In psychiatric practice, classification traditionally requires that when a symptom or a set of symptoms is better explained by a well-identified mental disorder, the diagnosis should be related to that psychiatric disorder. Self-mutilations may therefore occur in a spectrum of primarily psychiatric diagnoses. For example, in autistic spectrum disorders (8), schizophrenia (9) or mental retardation (10), as well as in Tourette and chronic tic disorders (11), Lesch-Nyhan (12, 13) or Prader-Willi (14, 15) genetically determined syndromes, with their neurological, behavioural and/or metabolic abnormalities. Consequently, self-mutilations seen in these psychiatric or neurological disorders should not be included in the restricted category of SISL, although a dermatological consultation and treatment may be required in all these conditions and some of the behavioural or pharmacological therapeutic approaches recommended in SISL could also be effective. The same principle should be applied to skin damage due to phlebotomy suicide attempts, skin or even deeper body self-injury seen in patients with various body delusions or hallucinations. The potential dermatological therapeutic approach of these patients is outside the scope of this article.
In its previous paper, the ESDaP group displayed the rationale of the proposed classification based on the answers to an initial question: “Is the behaviour responsible for the somatic damage denied or kept secret by the patient?” If the answer to this question is affirmative, the next question should be: “Are there any external incentives?”, thereby differentiating between malingering and factitious disorders. If the answer to the question is negative, the next question should be: “Is the behaviour responsible for the somatic damage compulsive or impulsive?”, thereby differentiating be-tween 2 different categories of skin picking disorders. This step-by-step classification tree helps to describe different categories within the set of SISL, as the purpose of both the previous paper and the current one is to help dermatologists identify and treat these syndromes. Most dermatological research published SISL are mainly dedicated to only one category, this being the compulsive spectrum of skin picking syndromes: “trichotillomania” or compulsive hair pulling, acne excoriée, etc. Moreover, as the new DSM-5 classification individualizes and includes “skin picking” within the spectrum of obsessive-compulsive disorders (OCD), the other category of skin picking, i.e. the impulsive one, does not belong to this diagnostic class and is supposed to constitute a clinical expression of different psychiatric diagnoses, such as borderline personality disorder.
There is evidence that SISL are more prevalent than previously believed: a 2010 study suggested that approximately 1.4% of adults in the USA are sufferers (16); a recent Canadian study concluded that the life-time prevalence of skin picking in young people was approximately 18% (17) and in 2013, in a German sample of 266 school children, 19.6% admitted occasional skin picking, with 1.9% regularly indulging in this behaviour and presenting clear stress regulation difficulties (18).
Dermatologists are therefore regularly called upon to treat patients who exhibit symptoms of SISL. The aim of this paper is to provide skin specialists not familiar with the psychiatric classification system (and/or behavioural disorders) with some stratified therapeutic principles on the taxonomy of the aforementioned lesions (1). The role of dermatologists is predominant in the management of patients with combined dermatological and mental disorders. Nevertheless, our purpose is not to encourage dermatologists to prescribe a wide range of psychotropic drugs or to engage in structured psychotherapeutic interventions without any specific training, but to provide them with some landmarks for better managing this kind of patients, in collaboration with mental health specialists. The therapeutic recommendations of the ESDaP group are derived both from evidence-based data, where available, and from the clinical experience of this multidisciplinary group of specialists.
Readers should bear in mind that certain categories of SISL, such as factitious disorders, are not suitable for systematic studies on the efficacy of different therapeutic approaches, due to the fact that they are relatively rare disorders, as well as for ethical reasons. Nevertheless, these clinical manifestations pose difficult problems and should be managed by well-informed dermatologists.
For the correct management of SISL, dermatologists should be aware of the importance of the psychological suffering that generally underlies this behaviour. Diag-nosis and treatment of the skin lesions are often the first steps for the dermatologist, but simply treating the lesion does not deal with the psychological suffering, often requiring a multidisciplinary approach involving mental health professionals. A multidisciplinary approach implies a combination or a succession of different therapies: dermatological treatment, psychotropic drugs, cognitive-behavioural therapy (CBT) and other psychotherapies, such as psychodynamic psycho-therapy or even psychoanalysis.
The basis for the management of all types of SISL is the patient–doctor relationship; its establishment may depend on experience with SISL patients, knowledge of psychodermatology and participation in a so-called Balint-group (19). Good listening skills, the ability to demonstrate empathy, and to engage in non-judgemental communication are other important qualities for the therapist. Treating SISL patients can be very difficult as they are often unaware of the psychological causes behind their symptoms or not cognisant of the link between their psychological suffering and their pathological behaviour. This lack of awareness is a significant obstacle to the establishment of a therapeutic alliance.
Feelings of frustration and discouragement are common among dermatologists treating SISL patients; subjects often show little or no improvement, and they may even present more or worsening symptoms.
Despite these difficulties, improvements in patients’ conditions can be a source of gratification for both dermatologists and psychotherapists. The worst therapeutic approach is to refuse to treat these patients, immediately referring them to a mental health professional, even before having established any kind of doctor–patient relationship. Patients need to understand their situation and have to be motivated before they start working with the mental health team. A therapeutic approach to the management of SISL can be made easier if the specialist has background knowledge as to why a human being is capable of self-harm.
Nock (7) developed an integrated theoretical model of the development and maintenance of self-harm, including risk factors and biographical aspects. The following hypotheses on the underlying mechanisms were proposed:
The dermatologist can suggest that the problem is not only physical (the skin), but that there might be other causes. Patients will often accept the possibility that the symptoms are aggravated by stressful situations in daily life. A basic physiological discussion on stress-reactions on the skin and the activation of skin nerves would be one of the first steps in a psychoeducational approach to motivating the patient to consider broader-based treatments. A clear statement about the complexity (not the difficulty) of the patients’ case is also recommended. A non-confrontational discussion on how and when the lesions appeared, and the suggestion that the patient may aggravate the injuries through their own actions, can be a way of determining the person’s awareness of their self-harm behaviour.
Some patients may comment on (or the physician will suspect) suicidal ideation. In these cases, co-operation with a mental health specialist is recommended. If access to a mental health professional is not possible or the patient refuses a referral, the dermatologist must determine if the patient’s feelings are limited to suicidal ideation or if there is a specific intention to commit suicide. If there is an intent, psychiatric treatment must be offered; in extreme situations, the physician should feel justified in forcing the subject to undergo a psychiatric examination, even without consent (depending on the legal structure in the country in question). For such a purpose, collaboration with the general practitioner can be essential.
Even when the dermatologist has carried out and correctly applied these management techniques, there will still be some individuals who will refuse any kind of psychiatric treatment. Based on members’ experience, the ESDaP group estimate that this may occur in as many as 15–30% of SISL patients. The maintenance of the therapeutic relationship could, in the medium-to-long term, convince these patients to change their opinion.
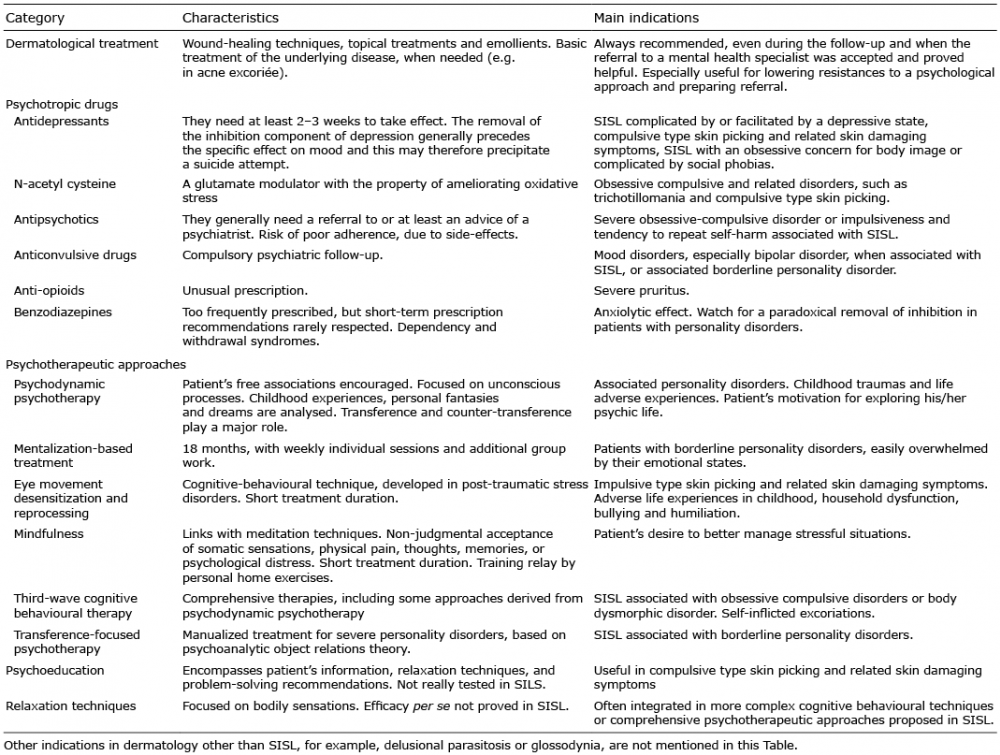
There are a number of therapeutic approaches that can be applied to SISL. For the dermatologist, the first step is the dermatological treatment of the skin lesions; a further priority is the establishment of a good doctor–patient relationship. The indications of the pharmacological and non-pharmacological approaches described hereafter depend on the type of the disorder. Several of these approaches can be combined, especially in the more difficult patients or in a second-line treatment. Most importantly, a multidisciplinary approach is often appropriate.
Table I. Overview of therapeutic approaches in self-inflicted skin lesions (SISL)
Antidepressants (Table II). The antidepressants commonly used in dermatology are: tricyclic antidepressants (TCAs) (amitriptyline, clomipramine, doxepin); tetracyclic antidepressants – (TeCAs) (mirtazapine); selective serotonin reuptake inhibitors (SSRIs) (fluoxetine, paroxetine, fluvoxamine, citalopram, escitalopram, sertraline); selective serotonin and norepinephrine reuptake inhibitors (SSNRIs) (venlafaxine, duloxetine); serotonin modulators (trazodone); and dopamine-norepinephrine reuptake inhibitors (DNRI) (bupropion). Antidepressants need at least 2–3 weeks to take effect. The physician must be aware of the fact that an anxiolytic effect and the removal of the inhibition component of depression generally precede the specific effect on mood and this may therefore, in rare cases, precipitate a suicide attempt. Dermatologists and other health professionals should bear in mind that by not treating a severely depressed patient the risk of suicide is much higher than prescribing an antidepressant with disinhibitory properties. Such a cost-benefit assessment might help dermatologists confront a patient presenting with both SISL and depressive symptoms.
Table II. Antidepressants
TCAs are long-established and efficacious antidepressants, but they are less used nowadays due to their adverse effects. The most commonly used TCA in dermatology is doxepin, which has a potent H1 and H2 histamine-blocking activity and represents the first-line “off-label” treatment for psychogenic excoriations and SISL linked to pruritus. Lower dosages of doxepin have anti-pruritic and sedative effects, but the antidepressant effect is limited.
Mirtazapine is a TeCA, which antagonizes adrenergic α2-auto- and α2-heteroreceptors as well as 5-HT2 and 5-HT3 receptors and can have significant effects on pruritus. Mirtazapine has a high affinity to central and peripheral histamine H1 receptors (21, 22). However, an adverse effect is weight gain.
SSRIs and SSNRIs are currently the most prescribed antidepressants due to tolerability and a favourable side-effect profile. A serotonin syndrome can develop when serotoninergic drugs, such as SSRIs and SSNRIs, are used concomitantly with monoamine oxidase inhibitors, triptans (e.g. sumatriptan for migraine treatment), antidopaminergic agents (e.g. metoclopramide for nausea) or antipsychotics (e.g. risperidone).
TCAs and SSRIs have other properties and are used in: panic disorder, OCD, PTSD, social phobia and generalized anxiety disorder. The fact that they are anti-compulsive means that they are a first-line treatment for all compulsive-type SISL as well as when an obsessive concern for body image contributes to skin picking behaviour.
N-acetyl cysteine. N-acetyl cysteine (NAC) is a glutamate modulator that has the property of ameliorating oxidative stress and has demonstrated promising effects in the treatment of OCD (23). Recent results in obsessive-compulsive related disorders, such as trichotillomania or compulsive type skin picking disorders, have to be replicated (24, 25).
Antipsychotics. The antipsychotics most commonly used in dermatology are typical antipsychotics (first generation) such as haloperidol or pimozide, and atypical antipsychotics (second and third generation) such as risperidone, olanzapine, and aripiprazole. First-generation antipsychotics have several side-effects (extrapyramidal side-effects, orthostatic hypotension, blurred vision, constipation, urinary hesitancy, galactorrhea and amenorrhea). This has limited their use and explains the low treatment adherence (or interruption of the treatment) on the part of the patients. This must be taken into account with patients who are reluctant to recognize the psychological component of their problem. Second- and third-generation antipsychotics are better tolerated (less extrapyramidal effects), even though many of them have metabolic side-effects, including weight gain, hyperglycaemia, diabetes mellitus and lipid abnormalities.
Antipsychotics are prescribed in dermatology for treating delusory parasitosis, severe OCD associated with SISL or the impulsiveness and tendency to repeat self-harm that is also associated with SISL. In these cases, the involvement of a psychiatrist is highly recommended.
Anticonvulsive drugs. Anticonvulsive drugs (lithium salts, carbamazepine, oxcarbamazepine, valproic acid, lamotrigine, etc.) are commonly used in psychiatry for treating mood disorders (especially bipolar disorder), as an augmentation strategy for depression resistant to antidepressants and for severe affective regulation problems and the behaviour instability usually present in borderline personality disorders. Side-effects include weight gain, acne conglobata, hidradenitis suppurativa and psoriasis (with lithium therapy); erythema multiforme and Stevens-Johnson syndrome (with carbamazepine and lamotrigine). They can, nevertheless, be useful in some conditions associated with SISL, but require considered prescription and follow-up by trained mental health professionals.
Anti-opioids. Naltrexone has positive effects in syndromes associated with severe pruritus (see European guidelines for pruritus treatment (26)).
Benzodiazepines. Benzodiazepines are the most commonly prescribed anxiolytic drugs. Short-term prescriptions are recommended but rarely respected. Side-effects (sedation, alcohol intolerance, lack of concentration, driving disturbances, agitation, sexual dysfunction), the frequency of withdrawal symptoms (depression, seizures, autonomic nervous system disturbances), rebound symptoms (anxiety, sleep disturbances, restlessness) and the risk of dependence or abuse should be taken into account, especially for patients with personality disorders. A paradoxical removal of inhibition can be observed and should be watched for, especially in patients with personality disorders, facilitating self-harm behaviour.
Psychodynamic psychotherapy. The concept of psychodynamic therapy has its origins in psychoanalytic theory. Psychodynamic therapy is also known as “insight-oriented therapy” and focuses on unconscious processes as they are manifested in a person’s behaviour. Analysis of early childhood experiences, as well as personal fantasies and dreams, can help improving self-awareness and understanding the influence of the past on present behaviour.
Psychodynamic therapy uses free association in a non-judgmental environment and takes advantage of transference and counter transference phenomena. “Transference” refers to the patient and is the repetition, in adulthood, of modes of relating to others (including doctors and psychotherapists), which were formed in infancy during early bonding (27). “Countertransference” concerns the doctor’s emotional, conscious and unconscious reaction to the subject, in accordance with his or her own family, personal and professional experience.
Whilst psychodynamic therapy is one of the psycho-therapeutic techniques that can be used as such, more specific and sometimes even manualized psychodynamic techniques have been applied and tested with patients with SISL or other underlying psychiatric disorders (28).
At this stage it should be mentioned that the legitimacy of integrating a psychodynamic approach in an evidence-based practice of medicine is a long-debated issue. Nonetheless, the evidence for the efficacy of such approach is increasing (29).
Mentalization-based treatment (MBT) (30) was developed for patients with borderline personality disorders. It is based on the idea that the consideration of mental states, in oneself and others, should lead to a better understanding and management of one’s self-harm behaviour. The goal of psychodynamic psychotherapy is for the subject to be able to deal with the mentalization of thoughts and emotions, especially in emotionally tense situations. Therapy takes place over 18 months, with weekly individual sessions and additional group work. In randomized-controlled studies (31) with an 8-year follow-up, efficacy was demonstrated by a lower number of suicide attempts (32).
Eye movement desensitization and reprocessing (EMDR) is a psychotherapeutic method developed for the treatment of trauma victims (33). In a recent article, Shapiro (34) reviewed all the randomized studies on EMDR therapy in treating psychological and somatic disorders and concluded that the technique can be successful in dealing with physically aggressive behaviour (pushing, grabbing, shoving, slapping, hitting). These are behaviours that are related to adverse life experiences in childhood, household dysfunction, bullying and humiliation. It has also been suggested that EMDR is useful for treating women who have experienced sexual violence (35).
Mindfulness is inspired by Buddhism and based on the non-judgmental acceptance of somatic sensations, physical pain, thoughts, memories, or psychological distress. There are 4 mechanisms: attention regulation, body awareness, emotional regulation, and change in one’s self-perspective (36). Mindfulness has been described as effective with somatization disorders, addictive behaviour, bodily distress syndrome (37) and PTSD (38).
Third-wave cognitive behavioural therapy. The “first wave” comprised the scientific behavioural therapies developed from the 1950s to the 1980s; the “second wave” is considered to be the CBTs that were popular between 1980 and 1990; nowadays, the “third wave” is denominated as a group of cognitive-emotional behavioural therapies that include: acceptance and commitment therapy (Hayes); schema therapy (Young), dialectical behaviour therapy (Linehan); cognitive behavioural analysis system of psychotherapy; functional analytic psychotherapy; and integrative behavioural couple therapy (39). Schema therapy has been used with OCD (40) and small-group intensive CBT was found to improve OCD symptoms and cingulate neurochemistry (41). Furthermore, it has been argued that it is more effective than anxiety management in treating body dysmorphic disorders (BDD) (42).
Self-inflicted excoriations have been improved with CBT (43).
Transference focused psychotherapy. Transference-focused psychotherapy (TFP) is a manualized, evidence-based treatment for borderline and other severe personality disorders that is based on psychoanalytic object relations theory. The treatment contracting/setting the frame, managing countertransference, and the interpretative process are 3 critical components of TFP (44). It is used to treat borderline personality disorders (45), which is often the personality disorder underlying SISL.
Psychoeducation has not really been studied in patients with SILS, although it is important for understanding skin reactions. The stress-symptom axis, tension-relief relaxation, problem-solving in helpless situations and neurogenic inflammation may offer additional explanations for the unknown origin of some skin symptoms. In PTSD, habit reversal techniques (see further on), skills training and avoidance of triggering situations could achieve positive results.
In general, relaxation techniques involve refocusing attention, concentrating on tranquillity and increasing awareness of the body. Relaxation was one of the first non-pharmacological treatments recommended by dermatologists (46). However, the use of relaxation as a stand-alone therapy seems to have a little effect on stress, anxiety and depression (47). Relaxation techniques include: autogenic relaxation (Shultz); progressive muscle relaxation (Jacobson); visualization; and deep breathing. They can be combined or present overlapping features with other similar therapeutic approaches, such as hypnosis, massage, meditation, Tai chi, yoga, biofeedback, music and art-therapy. Relaxation techniques are a main component of CBT and in habit reversal.
The SISL classification proposed by the ESDaP Group defines 4 main categories (1):
This sequence of clinical categories will be followed to offer recommended or specific therapeutic approaches in SISL.
The compulsive spectrum of SISL indicates obsessive-compulsive behaviours as the cause of the skin symptoms. Examples of such behaviour would be face picking (acne excoriée), nose picking, trichotillomania and onychotillomania.
There may be skin lesions (e.g. acne excoriée) before onset of the obsessive-compulsive behaviour although patients can start skin picking with no previous skin lesions (e.g. onychotillomania). The most frequent underlying comorbidities are: anxiety disorders (including the whole spectrum of OCD); depression; dissociation disorders; obsessive-compulsive personality disorder; borderline personality disorder; and body dysmorphic disorder (BDD), which is related to face skin picking in acne excoriée. BDD is also a possible comorbid disorder in other compulsive skin picking syndromes, such as trichotillomania (48).
The patient probably has an obsessive behaviour disorder that is easily diagnosed by the doctor on asking about behaviour at home or in stressful situations. Patients usually have feelings of shame and guilt. They are therefore reluctant to spontaneously disclose or admit this behaviour. Subjects may not trust the doctor, so the first step is to develop an open and confident relationship (see “General Principles”); non-judgmental communication is essential. Patients will have often tried to resist the behaviour, so comments like “You should stop doing it” are not helpful. Family members should be advised not to prohibit the behaviour, unless an agreement between the patient and his/her relative is reached which helps the patient to be aware of the behaviour; if the repetitive behaviour occurs when the patient is in a state of altered consciousness (dissociative state), external support can be useful.
Doctor–patient communication should be aimed at shared decision-making regarding options for avoiding the obsessive behaviour and focusing on the emotions of guilt and shame. A basic therapy option is the behavioural analysis of the situations where the obsessive behaviour arises or the identification of specific emotions or thoughts that lead to the skin lesions. Naming and defining the obsessive-compulsive mechanism can provide relief for the patient (this is not the case with factitious disorders). Suicidal ideation and attempted suicide are not frequent with this type of SISL.
In general, studies indicate that cognitive behavioural therapy for skin picking is the most effective treatment. Stein et al. (55) advanced the “A-B-C model” of habit reversal for hair pulling and skin picking (“A” – affect regulation; “B” – behavioural addiction; “C” – cognitive control).
The “habit-reversal therapy” for trichotillomania consists of 4 main components: (i) self-monitoring (the patient keeps a record of hair-pulling behaviour), (ii) awareness training (increasing patient’s awareness of both hair-pulling behaviour and high-risk situations that frequently trigger hair-pulling behaviours), (iii) stimulus control (techniques dedicated either to decrease opportunities to pull hair or to interfere with or prevent pulling, as for example wearing gloves in high-risk situations), and (iv) stimulus-response intervention (developing activities to substitute, such as deep muscle relaxation or taking a walk, when the desire for hair pulling occurs) or competing response intervention (engaging in a physically incompatible behaviour to the pulling for a short fixed period of time or until the urge goes away) (55–57).
Habit reversal techniques aimed at stopping the OCD seem to have positive outcomes: in 2006, Teng et al. (58) undertook a pilot investigation on habit reversal treatment in chronic skin picking and Twohig et al. (59) studied acceptance and commitment therapy as a treatment for the same problem. However, few scientific papers with small numbers of patients have been published, thus evidence is limited.
Cognitive interaction using a diary (as with food allergy sufferers) is another option for establishing more conscious self-treatment. The positive cognition increases when the patient and the dermatologist jointly set the goal of desisting from the skin picking or hair pulling behaviour; for example a 2- or 3-day period could be agreed, if the patient complies then they may give themselves some kind of reward.
If the dermatologist feels it is impossible to introduce these kinds of therapy options, a mental health specialist should be contacted. The organization of a team that includes a general practitioner, a mental health professional, specialist nurses, etc. is recommended.
A systematic meta-analysis published in 2007, based on 7 randomized studies comparing pharmacological (clomipramine or SSRIs) and behavioural treatments (habit reversal therapy) for trichotillomania demonstrated that the effect size of habit reversal therapy was superior to pharmacotherapy. Furthermore, it demonstrated that only clomipramine (not SSRIs), was superior to placebo (57). A more recent meta-analysis published in 2014 by McGuire et al. (60) confirms the superiority of behaviour therapy to pharmacological treatments; especially for behaviour therapy trials that used mood-enhanced therapeutic techniques. Clomipramine exhibited larger effect sizes relative to SSRIs, but the difference was not statistically significant.
If there are life-long problems, specific problems with emotional communication, or if underlying anxieties appear, patients with acne excoriée, trichotillomania or another disorder belonging to the compulsive spectrum of SISL might benefit from psychodynamic psychotherapy. This of course will depend on the time-frame and the availability of such therapists.
If patients are able to accept the diagnosis of OCD the prognosis is generally favourable. Non-acceptance may indicate more severe personality problems and the specific therapeutic aspects of SISL should be considered. The relationship with the dermatologist is probably the most important prognostic factor. The presence of an impulsive component in compulsive type skin picking disorders is generally considered as an index of severity (61) and pushes some psychiatrists to support the categorization of skin picking disorders as an impulsive control disorder, rather than an obsessive compulsive related disorder (62). The phenomenology of trichotillomania and pathological skin picking, especially the fact that these behaviours are not always triggered by obsessional thoughts and can begin without the person’s awareness, contrarily to classical OCD, led some authors to reject the DSM-5’s new category of obsessive-compulsive and related disorders (OCRDs) and along with its content on both scientific and logical grounds (63).
As mentioned by the ESDaP group, impulsive skin picking and related skin damaging syndromes are acts of uncontrolled aggression to the skin. These behaviours frequently offer rapid, but short-lived, relief from a variety of intolerable conditions, providing vital support for the patient, aiding their psychological survival, albeit in a pathological state” (1). This spectrum of disorders is most common in adolescence.
Impulsive skin picking usually involves more personality disorders than the obsessive-compulsive type; borderline personality disorders, narcissistic personality syndromes and antisocial personality disorders are frequent. Substance abuse, risk-taking behaviour (binge drinking, illegal drug use, promiscuity, unprotected sex, etc.) and eating disorders could also be present. A history of sexual, physical and/or emotional abuse (especially in childhood and puberty) with post-traumatic stress may have impaired the emotional regulation capacity of these subjects. Less severe impulsive SISLs can correlate with mood disorders.
Impulsive-type SISL lesions can also be referred to as “non-suicidal self-injury”: the deliberate, direct destruction of body tissue without conscious suicidal intent. The most common forms are biting, cutting, scratching, hitting and burning. These kinds of self-injuries are not specific to psychiatric populations, although they are more frequent in this group. In 2007, an observational study on a population of adolescents (6) found that up to 46.5% had committed some form of non-suicidal self-injury during the past year and 28% were moderate or severe cases. This high prevalence of non-suicidal self-injury observed in a community sample, and not in clinical population, indicates that this phenomenon can be overlooked unless open-ended questions are tactfully asked to inquire about the behaviour. Therefore, it is important to have established a relationship of trust before approaching these issues. In general, there is a tendency among young people to trivialize this behaviour, which can range from minor to severe self-injury. Minor self-injury is often not recognized or may be denied as pathological behaviour as it would correspond to a normative expression of teen culture. However, moderate and severe forms are generally associated with personality disorders and other self-harm behaviours, such as drug abuse, eating disorders, risk taking behaviour, bone breaking, falling, jumping, etc., as well as suicidal ideation and suicidal attempts. Some authors (64–66) have tried to attribute multiple functions to non-suicidal self-injury, such as to relieve negative emotions, to relieve negative thoughts, to self-punish, to set boundaries with others, to feel something (even if it is pain), to provide a sense of security or control, to get attention, etc. Of course, puberty is accompanied by body transformations and sexual arousal, which can be difficult to handle and contain for some, and may lead to self-inflicted behaviours as a mean of tension relief. Males seem more likely to self-harm as a means to communicate or influence others; females are more likely to engage in self-harm for relief of intra-punitive issues, such as self-hatred, depression or loneliness. Aside from gender differences, it appears that positive and negative reinforcement and acceptance incite repetition, trivialization and amplification of non-suicidal self-injury behaviour.
After unambiguous diagnosis and definition of the type of impulsive behaviour, the first step is to discuss the different options for ending the harmful behaviour. Unlike obsessive-compulsive behaviour, the impulsive state is not repeated chronically. It is also unusual for the patient to harbour feelings of shame or guilt.
Patients are generally willing to talk about their impulsive behaviour. Relief of tension is a typical motivator and the physician should raise this issue, as it is possible that the patient will not be aware of it. Some patients are not psychologically disturbed, but indulge in impulsive self-harm in imitation of their peer-group without understanding the potential long-lasting effects of scars and wounds. Intolerance and frustration could be the cause of the impulsive behaviour.
Impulsive behaviour is also characteristic of patients with severe destructive personality problems: borderline personality disorders, narcissistic personality disorders and PTSD in which the impulsive self-harm is only one symptom of the condition.
Impulsive-type SISLs can be considered as a risk factor for suicide, especially in male adolescents (67). Suicidal ideation and suicide attempts are much more frequent with this type of self-harm, and the physician should always take this into account when dealing with the patient (see general principals on suicidal ideation management). Sometimes the impulsive-type of skin lesion, even if it is not a severe dermatological symptom, can be the final signal from the patient before suicide is attempted; a self-harm risk assessment is therefore recommended.
A cognitive behavioural approach could begin with a discussion on impulsive situations, with the aim of determining emotional triggers for the actions. This could lead to a strategy for dealing with the “point of no return” some minutes or seconds before the self-harm begins (squeezing a small ball in the hand; pinching the skin; pulling an elastic band to the skin at the arm/hand; putting emotions in a “safe place”, the “treasure box philosophy”; turning attention to external stimuli; communicating with others etc.).
Linehan’s dialectic behavioural therapy (69) and transference-focused psychotherapy (44) for borderline personality disorders are recommended. A mindfulness-based approach (70) is another option for psychotherapy.
In adolescents, family therapy should be considered, especially if eating disorders are also present.
The first-line goal should be to lower the frequency of the impulsive behaviour. Without therapy, the prognosis is poor, suicidal ideation and suicide attempts are common and the self-harm will probably continue (in approximately 46.5% of patients, according to Lloyd-Richardson et al. (6). If patients have access to, and are able to accept mental health treatment, the prognosis is positive, but this obviously depends on the severity of the underlying personality problems.
Factitious disorders in dermatology are defined as the induction of skin lesions by the patient: this induction is kept secret until an appropriate relationship with a caregiver is established. The subject may be aware that he or she is driven to create the lesions, or in some instances the activity may take place in a dissociative state outside the patient’s awareness. Dermatitis artefacta, factitious dermatitis or dermatitis factitious are often synonymously referred to as factitious disorders. We already recommended the avoidance of these terms and their replacement by the term “factitious disorders in dermatology”, since dermatitis suggests underlying inflammation (1). Lesions are usually seen in areas that are available to the handedness of the patient; the most frequently affected sites are the face, arms and legs. Factitious disorders can also occur in children and adolescents, but this syndrome has to be differentiated from Polle’s syndrome or Munchausen syndrome by proxy, where a subject, most often the mother, may artificially cause a skin disease in her own child.
The main motivation is assumed to be a method for coping with a severe psychological background and a preference for the sick role with no immediate tangible benefits. Factitious disorders in dermatology are at least twice as frequent in women as in men.
Cutaneous lesions can be accompanied by other factitious disorders; for example, a chronic fever due to the manipulation of the thermometer. These associations may complicate and delay the diagnosis, which is always difficult to establish.
Patients presenting factitious symptoms sometimes describe demonstrative and dramatic problems and give false information on their medical history (“pseudologia fantastica”); they may speak of many hospital stays and show numerous scars from surgical procedures (“doctor and hospital shopping”). This is characteristic of Munchausen’s syndrome, a clinical subtype of factitious disorders, more frequent in men than in women. In Munchausen’s syndrome, self-harm is often delegated to the care providers.
Borderline personality disorder, substance abuse, somatoform pain disorder, conversion disorders, sexual disorders, dysthymia and suicide attempts are frequently associated with factitious disorders (71, 72). Substance abuse, eating disorders and personality disorders are more frequently associated with factitious disorders involving direct self-harm (scratching, cutting, burning) than in those involving indirect self-harm (use of medication, chemicals or infectious substances); in these cases, anxiety disorders, adaptation disorders and somatoform disorders are more frequent. Mood disorders seem to be common in both types of factitious disorders (73). Depression can precede the onset of a factitious disorder.
Patients with borderline personality disorder have often experienced abandonment, family separation or hospitalization in their childhood, resulting in intense affective dependency, which explains the sensitivity of these patents to separation, mourning and emotional disappointment. These situations very often re-open old wounds of abandonment. Concomitant or family physical disease (especially if it affects a close family member) is a common association (74).
Some participants in the ESDaP Group suggest the possibility of a paranoid personality when a factitious disease occurs in a man.
Communication between the patient and the healthcare providers. Patients with a factitious disease often model their relationship with the doctor on relationships they have had with parental figures or relatives. They may see any close relationship as bearing a threat of betrayal, abandonment and even aggression. This can explain the ambivalent attitude of many factitious disorder patients towards their physicians. Although a good initial relationship may develop, sufferers will demand more and more attention, care, and medication. This is often followed by disappointment, ignorance and even an accusatory attitude; expectation and rejection, love and hate, may therefore coexist. The effects produced by a factitious skin disorder on others will reproduce this ambivalence. Damaged skin represents both a call for help, an appeal for care and love, and a means of distancing from others, defying and aggressively manipulating those who are perceived as unreliable or even dangerous.
It has been suggested that patients with a factitious skin lesion seek painful sensations to create an “envelope” of suffering to restore their bodily and psychological boundaries, which they perceive as damaged. By damaging their skin and by lying about the cause of their “skin disease”, patients with factitious skin lesions not only reset their own limits, but also acquire an identity: a “surface identity” or “patient identity” that is a camouflage for their internal emptiness. Through illness, the subject may establish a relationship, if only with a healthcare provider. The healthcare provider will provide the patient with the skin and body care that was acutely inadequate or completely lacking in childhood.
Patient–dermatologist communication. It can be difficult for the dermatologist to accept that a patient is responsible for their own lesions; acknowledgement means jeopardizing the doctor–patient relationship as the physician may feel that they have been manipulated. However, avoiding this possibility risks the reinforcement of the patient’s position, allowing them to believe in the reality of their condition and this, in turn, can strengthen the patient’s masochism and cause them to increase the production of lesions.
If the dermatologist is capable of contemplating the possibility of psychological suffering and understanding that self-produced lesions are the expression of that suffering, it is easier to diagnose a factitious disorder. This enables early diagnosis and avoids the deterioration of the doctor–patient relationship. In a hospital setting, supervision by an external mental health professional (for example, a psychoanalytical supervisor) can improve screening for factitious disorders (73).
If a dermatologist does not feel sufficiently confident to manage the psychological aspects of a skin condition that they suspect is self-produced, they should (at least in the initial stages) refer the patient to a dermatologist that is more experienced in this pathology, or to a psychiatrist–psychotherapist or psychologist. This should be done as soon as possible because a late referral to a mental health specialist may cause the therapist to be viewed as the person who forces the patient to admit to self-harm. Patients with factitious skin lesions rarely refuse a first meeting with a psychiatrist–psychotherapist or psychologist, as long as they do not feel rejected by their dermatologist.
Screening and objectively identifying a depressive condition is a means for the dermatologist to broach the subject of the psychological and emotional state of the patient with a factitious skin lesion and it may be used as the basis of a request for help to a mental health specialist.
Attempts should be made to adhere to appointment schedules and to create a safe and accepting environment during the consultation (74). It is preferable to avoid any reference to the physical mechanisms causing the lesions, and to focus on “stress” as the probable mediator; this may be easier for the patient to accept and could be a rationale for the introduction of psychotherapy or a psychiatric consultation. Referring to a mental health specialist could be interpreted as a subtle means to force the patient to confess responsibility for the lesions.
Communication between a dermatologist and healthcare teams. When a person with a factitious skin lesion is hospitalized, the healthcare team must work together to determine a common approach and to maintain the links between the various healthcare providers; they should also offer support to fellow workers and deal with any feelings of irritation, aggression or rejection towards the patient that can be caused by a sense of manipulation and ambivalence. If these feelings are not addressed, they can lead to the prescription of unnecessary medication or even surgical procedures that could be dangerous for the patient. This could ultimately result in the development of a sadomasochistic relationship between the factitious skin lesion patient and the healthcare provider.
Communication between the dermatologists, patient’s relatives and his/her general practitioner. Precautions must be taken when informing relatives (and even the patient’s general practitioner), of the condition. The dermatologist should emphasize the seriousness of the psychological suffering that is expressed through the SISL. Relationships with relatives can be uncomfortable: the family are often angry and accusatory and believe that the physician is incompetent (75). The relatives may have noticed the suffering of the patient and can play a role as a mediator in resolving family conflicts. It is important that the relatives are not told that it is the patient that is responsible for their own lesions (unless this is first suggested by the relatives themselves). Dermatologists should be aware that some general practitioners are reluctant to consider the possibility of a SISL and may tell the patient that the diagnosis of self-harm is the idea of the dermatologist, thereby jeopardizing the therapeutic approach.
Factitious cutaneous disorders are probably the most complex of all self-inflicted skin lesions. Treatment objectives are more easily achieved when the dermatologist is non-judgmental about the patient’s condition and has acquired specific skills for treating it. There are very few publications that encourage the physician to confront patients suspected of self-harm behaviour: most authors argue that conflict is counter-productive and even dangerous (76–78). Aggravation of the lesions, breaking contact with the healthcare team, becoming delirious and even suicide have been reported in cases where patients have been directly questioned on their responsibility for the lesions.
Dermatological treatment is of particular importance with factitious skin lesions because the underlying causes are not usually hidden or denied. Occlusive dressings (especially standard plaster casts), which allow the skin lesions to heal completely (confirming self-infliction) may be applied and local treatments such as antiseptic solutions, antibiotic ointments and healing ointments may be prescribed. After antimicrobial susceptibility testing, antibiotics may be used to treat secondary infections of the skin, subcutaneous tissues and, occasionally, bacteraemia or septicaemia.
Surgical procedures that are often requested by patients with Munchausen’s syndrome should be avoided. Reparative plastic surgery should only be considered in collaboration with a psychiatrist-psychotherapist, only after the skin has healed and on the condition that a marked improvement has been observed in the patient’s psychological state.
Antidepressants can be useful with associated depressive syndromes and for encouraging the patient to accept a psychological approach. Tranquillizers and antipsychotics can treat underlying impulsiveness or emotion regulation disorders, especially in cases of severe comorbid personality disorders, but they should only be used after careful consideration: there is a risk of abuse and of damaging the trust that has been built up between the doctor and patient.
Several, previously described, approaches for managing borderline personality disorders underlying SISL can be applied. The therapist must have experience in treating this type of condition and be able to adapt to the very special personality of patients with factitious disorders; progress is slow and sufferers have great difficulties in verbalizing their feelings and conflicts.
In contrast to the defeatist position found in some publications (79, 80), the ESDaP Group believes that a psychological and psychodynamic approach can be successful with these patients, as long as the psychotherapist is convinced of the possibility of success and is prepared to persevere (81). The psychotherapist’s awareness of counter-transference feelings and support or individual supervision in the follow-up period can result in more positive outcomes.
In adolescents, factitious disorders often represent “a cry for help”. In general, the early onset of a factitious disorder has a better prognosis than late onset. This is also true with mild forms of factitious skin lesions and in cases in which the lesions are produced in a dissociated state. As always, the quality of the psychotherapeutic relationship is a significant factor.
Malingering is the production or feigning of a well-known symptom or lesion by the patient. The patient is aware that the lesion is self-inflicted, but will deny responsibility with the aim of gaining a social or financial advantage. In dermatology, patients may intentionally aggravate the symptoms of pre-existing skin conditions, but they may also cause de novo skin lesions. The term “malingering” is often used to describe the aggravation of a pre-existing lesion, whilst “simulation” refers to feigning a subjective symptom or the creation of a new lesion. There will be no prior history of self-harm and the patient will rarely admit to the behaviour. The doctor–patient relationship is therefore complicated and the first step is to validate diagnosis (careful observation of the patient’s behaviour, dressings that make self-harm more difficult, etc.).
Comorbidities cover the full spectrum of personality disorders, especially antisocial personality disorders and Munchausen’s syndrome. An illustrative example would be a real-life case that was brought before one of the authors of this paper: a middle-aged woman with an allergy to bee stings suffered sexual abuse at her job, she deliberately instigated contact with the insects (her husband was an apiculturist) and the presentation of the consequent symptoms of anaphylaxis and Quincke’s oedema meant she was able to avoid work. It took a number of years before this was recognized and the patient was able to discuss the problem.
Communication should be aimed at offering comfort and suggesting explanations for the condition. The objective is that the patient becomes able to disclose and talk about the underlying problem. Collaboration with the general practitioner and other health professionals is recommended.
No specific therapy options have been described for malingering. Each case is different and an individual approach with close supervision is advisable.
If the patient cannot be convinced to undergo therapy, the prognosis is not favourable.
Dermatologists often lack therapeutic strategies for dealing with patients who present SISL. This article aims to help dermatologists without psychotherapeutic training to deal with such patients. Ideally, treatment should be initiated during the dermatology consultation, and delaying this treatment may lead to repetitive behaviour, making it more and more difficult to treat. The therapeutic recommendations put forward in this paper are based on the review of the literature and on the experience of a group of dermatologists, in collaboration with mental health specialists. These recommendations are not exhaustive, but they are known to be effective. For example, until now, very little has been written about the family members of self-harm patients and the potential benefits of family therapy. More research, based on the classification, using prospective and comparative studies is needed to refine the strategies for each condition. However, as the doctor–patient relationship is the cornerstone for improvement, comparison is somewhat complex. If new studies can be developed that employ diagnostics with reference to the classification, a more accurate prognosis for each type of SISL may be forthcoming, something that is clearly lacking in the literature. These studies would also help to confirm that the classification is functioning in the day-to-day work of the dermatologist.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize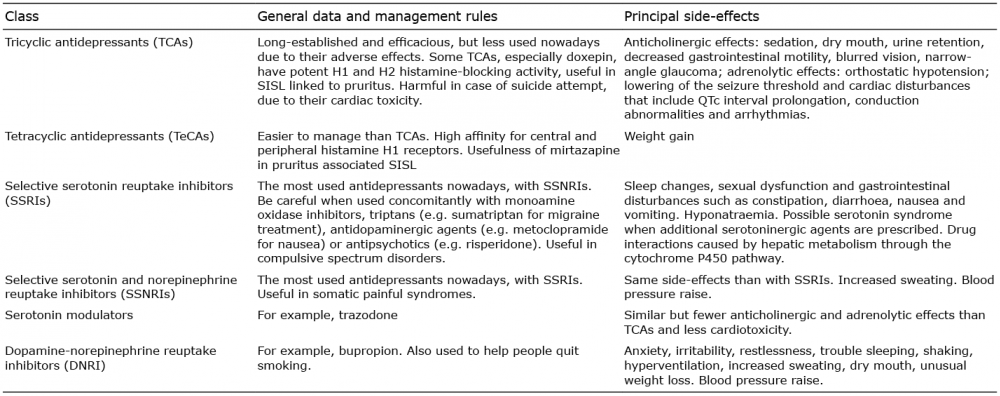 Click to show fullsize
Click to show fullsize