


1Department of Dermatology and Itch Center, 2Department of Rheumatology, Temple University School of Medicine, 3322 North Broad Street, Medical Office Building, Suite 212, Philadelphia, PA 19140, USA, and 3Biostatistics Unit, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore. *E-mail: yosipog@gmail.com
Accepted Aug 22, 2016; Epub ahead of print Aug 26, 2016
Sjögren’s syndrome (SS) is an autoimmune disorder characterized by inflammatory destruction of the salivary and lacrimal glands (1). SS can occur in the setting of comorbid rheumatologic disorders, which is considered secondary SS (s-SS), while primary SS (p-SS) occurs in the absence of such disorders (1). The prevalence of p-SS widely varies depending on the diagnostic criteria utilized and has been reported to range from 0.22 to 2.7% (1). Previous studies have reported that pruritus and xerosis are among the most common cutaneous manifestations in p-SS (2, 3). We aim to assess the characteristics of pruritus and its effect on quality of life (QoL) in patients with p-SS as no study to date has examined this.
All patients with established diagnosis of p-SS using the American College of Rheumatology Classification Criteria (4), were recruited from the Department of Rheumatology outpatient clinics, who were seen from February 2014 to March 2016. Of 21 patients with p-SS screened, 19 agreed to participate. All consented patients underwent both rheumatologic and dermatologic evaluations.
Participants suffering from chronic itch were asked to complete the Questionnaire for the Assessment of Pruritus, designed to capture the various dimensions and clinical characteristics of pruritus, as well as the ItchyQoL (5, 6). The design of the questionnaire has been detailed previously (6). The ItchyQoL evaluates how itch affects the subject’s QoL by analyzing 3 domains: symptoms, functional limitations, and emotions relating to itch. Xerosis was objectively assessed utilizing the overall dry skin score (ODS), a standardized tool (7).
From the chart, laboratory parameters, such as anti-nuclear antibody (ANA), rheumatoid factor (RF), anti-SSA, anti-SSB, complete blood count, and comprehensive metabolic panel, were obtained from patient medical records. Medications and comorbid conditions were also documented.
All analyses were performed using software (SPSS 16.0, IBM Corp, Armonk, NY). Descriptive statistics for quantitative variables were presented as mean ± SD and as percentages for qualitative variables. Spearman correlation coefficients were presented to assess relationships between quantitative and ordinal qualitative outcomes. Correlations between lab values and chronic pruritus were determined using the Mann Whitney U test. Statistical significance was set at p < 0.05.
The patients mean age was 55 years (range 30–74) with 18 (94%) females and one (6%) male (Table SI).
Ten subjects (53%) reported suffering from chronic itch with a mean duration of 74.4 months (range 12–240). The mean ± SD itch intensity reported using the visual analogue scale (VAS) was 7.7 ± 1.7. The most common locations were: shins (90%), back (80%) and forearms (70%). Six out of 10 subjects considered scratching to be pleasurable with a mean score of 2.6 ± 3.2 on the Likert scale.
Itch intensity was worst during the evening and least severe in the morning. Itch was rated as most intense during the summer rather than the winter. The most common aggravating factors were dry skin (70%) and hot water (50%). The onset of itch ranged from 11 years prior to diagnosis of p-SS to 3 years after the diagnosis. Eight subjects with chronic itch reported sleep disturbance due to itch.
Xerosis was present in 9 (90%) of the pruritic subjects as opposed to 4 (44%) in those without itch. When the severity of xerosis (grade 0 to 4) was compared between patients with itch (mean 1.1) versus no itch (mean 0.6), no statistical significance was seen (p = 0.1).
The mean ± SD QoL score of p-SS patients with pruritus was 57.3 ± 18, which had a significant correlation coefficient of 0.71 (p = 0.02) associated with severity of itch. The emotional domain of the total ItchyQoL score was the most noteworthy, with the largest reports being “aggravated by temperature or seasonal changes” (mean ± SD score of 3.9 ± 1.2) and “need to scratch” (3.7 ± 0.8).
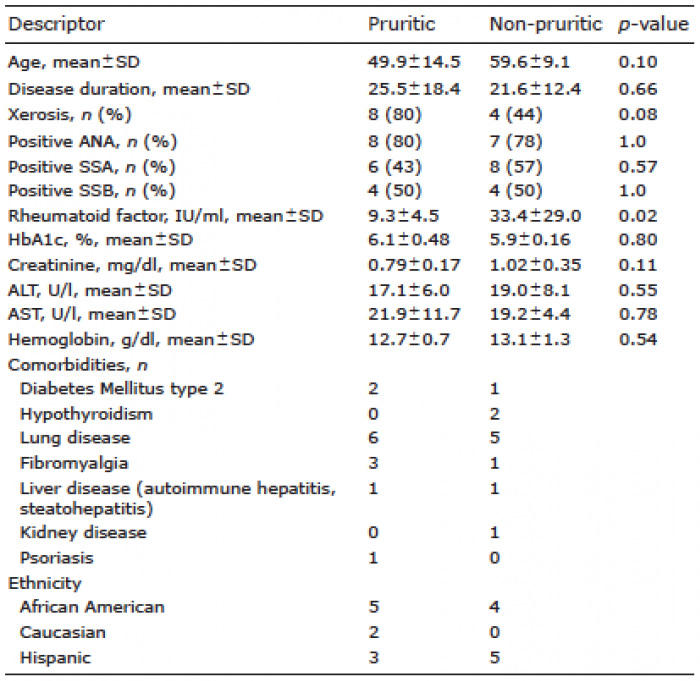
There was no significant difference in disease duration of p-SS between pruritic vs non-pruritic patients. Similarly, no differences were detected when analyzing liver enzymes (ALT, AST, ALP), creatinine, hemoglobin and serologic markers (ANA, SSA, SSB), between the 2 groups. Only RF was significantly elevated in patients without itch (p = 0.02) (Table I). None of the serologic markers were associated with xerosis (RF, ANA, SSA, and SSB) (data not shown).
Table I. Characteristics of pruritic vs non-pruritic patients
Pruritic comorbidities among the patients with chronic itch included diabetes mellitus, steatohepatitis, and psoriasis (Table I).
Interestingly, itch may be the presenting symptom in patients with SS (3). One previous study on p-SS revealed an itch prevalence of 42% (2). We found a similar prevalence with 53% of our subjects reporting to suffer from chronic itch. Itch intensity in p-SS is higher when compared to other rheumatologic disorders (8).
The exact pathophysiology of chronic itch in SS patients is not well understood; however, p-SS is highly associated with skin xerosis (2), which is a common cause for chronic itch in other dermatologic conditions such as geriatric skin (9). Although previous studies have reported a correlation between the severity of xerosis and disease duration, our current study failed to replicate these findings, suggesting that xerosis may not be the only factor involved in itch of p-SS. It has been proposed that xerosis and pruritus found in p-SS may result from eccrine sweat gland destruction (10). Indeed, this would aid in explaining our finding of increased itch severity during the summer, as patients that exhibit anhidrosis report that pruritus accompanies heat (11). However, immunohistochemical analysis has failed to demonstrate eccrine gland involvement in SS (12).
Other possible causes of chronic itch, such as diabetes mellitus, kidney or liver disease and anemia, did not demonstrate a major role in the presence of itch, as we did not uncover a relationship between chronic itch and serum levels (13, 14).
In our study, patients with chronic itch reported low QoL score (57.3 ± 18) and up to 80% mentioned sleep disturbances. Sleep disturbance has previously been shown to correlate to depressive and somatic symptoms, and has a negative impact on mental and physical function (15).
The itchiest locations were the shins. The shins are a very common location of xerosis and pruritus in the elderly (9); and indeed, similar histopathologic changes in the skin have been noted in p-SS and xerosis of the elderly (10).
SSA has been found to positively correlate to xerosis in patients with p-SS (2); however, in our study only normal RF values were correlated with itch.
This study has several limitations. Our sample size of only 19 patients made many variables difficult to analyze, such as medication effects or co-morbid conditions. A larger sample size would lend more power to our statistical analysis.
We thank Dr. Suephy Chen, MD from Emory University for giving us permission to use the ItchyQOL.


 Click to show fullsize
Click to show fullsize