


1Dermatologist, rue Frans Binjé 8, BE-1030 Brussels, and 2Free University of Brussels (ULB), Institut de Recherche Interdisciplinaire en Biologie humaine et moléculaire (IRIBHM) & Service de Biostatistique et Informatique médicale (SBIM), Brussels, Belgium. E-mail: fabienne.forton@skynet.be
Diagnosing papulopustular rosacea is not always straightforward; no specific diagnostic test is currently available. A high density of Demodex mites is consistently observed in this condition. This retrospective study assesses an improved method for evaluating Demodex density among 1,044 patients presenting to our dermatology practice. The skin was cleaned with ether and Demodex densities were measured in 2 consecutive standardized skin surface biopsies taken from the same site. Mean densities in patients with rosacea and demodicosis were much higher than those in healthy controls and patients with other facial dermatoses. The optimal cut-off values for the 2 biopsies were combined and the resultant criterion (presence of a first biopsy density > 5 Demodex/cm2 or a second biopsy density > 10 Demodex/cm2) enabled confirmation of a diagnosis of rosacea or demodicosis with a sensitivity of 98.7% and specificity of 95.5%, making this a valuable diagnostic tool for dermatologists in routine clinical practice.
Key words: Demodex; rosacea; demodicosis; acne vulgaris; seborrhoeic dermatitis; standardized skin surface biopsy.
Accepted Aug 29, 2016; Epub ahead of print Aug 30, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Fabienne Forton, rue Franz Binjé, 8, BE-1030 Brussels, Belgium. E-mail: fabienne.forton@skynet.be
Rosacea is a common dermatosis, affecting approximately 10% of the population in Sweden (1). It is defined by the consensus of the National Rosacea Society (NRS) as a central face distribution of at least 1 of 4 primary features: flushing, persistent erythema, papules and pustules, or telangiectasia (2). Four subtypes of rosacea were defined by the NRS consensus: erythematotelangiectatic rosacea, papulopustular rosacea (PPR), phymatous rosacea, and ocular rosacea; and one variant (granulomatous rosacea), each associated with specific groups of symptoms (2). PPR is the most difficult to diagnose. It can be confused with other common dermatoses, such as acne vulgaris and seborrhoeic dermatitis, and can also coexist with these dermatoses (2–6). According to the consensus definition, 2 key clinical features are considered necessary for a diagnosis of PPR: persistent erythema and transient papulopustules (2). At present, no diagnostic test is available.
Demodicosis is also a frequent skin condition (3), but is underdiagnosed (3, 7–9). The definition and classification of demodicosis are still being debated (10–12). Diagnosis is suggested by the presence of non-specific features, including follicular scales, redness, sensitive skin, pruritus, perifollicular macules or papules, atypical eczematiform eruption, folliculitis, isolated inflammatory papules and pigmentation (3, 11–17) and confirmed by the presence of a high density of Demodex mites (3, 7, 10, 11, 13, 14, 18, 19) and by clinical cure after acaricidal treatment along with normalization of Demodex density (Dd) (14, 15, 17, 19).
Although a pathophysiological role of Demodex is generally accepted in demodicosis, it remains controversial in PPR (12, 20). Nevertheless, high mean Dds are consistently observed in PPR (18, 21–27), cases of PPR with low Dd values are rare (12.5–16%) (3, 25) and topical acaricidal treatment has been shown to have beneficial effects in patients with PPR, supporting a key role of the mite in this condition (19, 28). It is also beginning to be accepted that Demodex mites are one of numerous triggering factors for Toll-like receptor 2, which is implicated in the immune reaction observed in PPR (29).
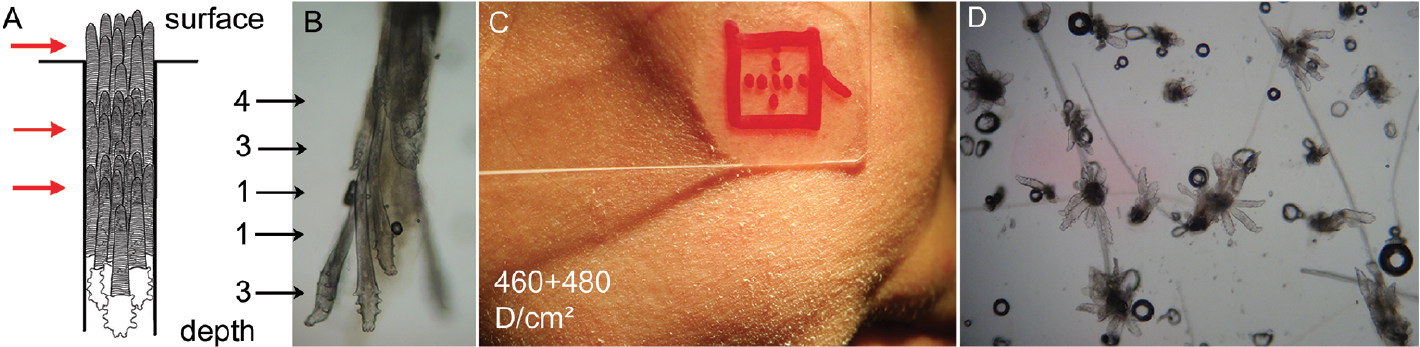
In 1971, Marks & Dawber (30) described the skin surface biopsy, a method in which the superficial part of the horny layer of the skin and the follicular content are sampled, allowing the presence of Demodex folliculorum (which mainly lives in hair follicles) to be detected. In 1993, we introduced the concept of “Demodex density”, and adapted the method of Marks & Dawber so that this density could be measured; we standardized the surface to be analysed and called this method the standardized skin surface biopsy (SSSB) (18). By comparing patients with rosacea with healthy controls, we proposed a cut-off value of 5 Demodex/cm2 (D/cm2) for a diagnosis of PPR (18), which was subsequently confirmed and adopted by others (8, 31–36). This sampling method is quick and simple, reproducible, only slightly invasive, well-tolerated by patients (3, 37), cheap and, therefore, readily available to all dermatologists; however, its sensitivity is not very high (55%) (18, 38). In 1998, to increase the sensitivity, we proposed that the skin and the biopsy slide should be cleaned with ether before the SSSB and that a second, and therefore deeper, SSSB should be performed at the same site immediately after the first (Fig. 1) (38).
Fig. 1. Demodex folliculorum dispersed along the follicles is collected by consecutive standardized skin surface biopsies (SSSBs). (A) Schematic representation of numerous Demodex mites, agglutinated at different levels (red arrows) inside the follicle. (B) Microscopic view (×100) of 12 D. folliculorum agglutinated at different levels of the follicle on a standardized skin surface biopsy (SSSB) (numbers next to the arrows indicate the number of mites at each level): this picture is relatively rarely observed because usually the follicle content breaks and the different levels are kept by stumps on the consecutive SSSBs. (C) Pityriasis folliculorum on the right cheek of a 41-year-old woman, with the lamina of the SSSB (18). The opisthosomas of the most superficial mites are visible as thin, white follicular scales at the base of the hair, giving a frosted appearance and a rough texture, often felt to be dry skin by the patient. SSSB1+SSSB2 are indicated on the figure. (D) Microscopic view (×40) of numerous D. folliculorum (n=73) as they usually appear on SSSB: 1 level of Demodex is observed in each follicle, with 1–9 D/follicle.
This approach has since been used by other groups (3, 19, 32, 37, 39, 40).
In the present study, we investigate for the first time the systematic use of this deeper second sampling for Demodex in groups of patients with PPR, demodicosis and healthy skin, but also in a group of patients with other facial dermatoses, particularly those that can resemble PPR clinically.
We determined optimal cut-off Dd values for each of the 2 consecutive samples, and combined these 2 values to obtain an overall diagnostic criterion. We then validated this criterion in patients with conditions already known to have high Dds, i.e. PPR and demodicosis.
Our aim was to provide a validated, improved and useful diagnostic tool to assist dermatologists in routine practice.
This retrospective study was approved by the Erasme Hospital ethics committee. All patients attending our dermatology practice in Brussels between 2002 and 2010 with clinical symptoms and signs suggestive of PPR (rosacea with centro-facial papulopustules) or demodicosis were included in the study.
The PPR-suggestive group was subdivided into patients with “typical PPR” (i.e. centro-facial papulopustules with persistent erythema) and those with other forms (centro-facial papulopustules without persistent erythema, granulomatous rosacea, steroid-induced rosacea). The diagnosis of demodicosis was made by an experienced dermatologist based on the combined presence of several clinical features and signs suggestive of the diagnosis, e.g. follicular scales, papules, folliculitis, pigmentation, pruritus, etc. Each of the patients with a clinical diagnosis suggestive of PPR or demodicosis had 2 successive SSSBs performed.
Patients with other facial dermatoses and healthy control patients (carefully selected to avoid including pityriasis folliculorum or erythematotelangiectatic rosacea) were also included if the consultation time was sufficient for 2 SSSBs to be performed. Patients with an uncertain clinical diagnosis, young children (under 7 years of age) and patients who had previously been treated for demodicosis and were returning for follow-up were not included.
For each patient, the date of consultation, age, sex, clinical diagnosis, location of the SSSBs and Dd values were recorded. Some of the patients with demodicosis and some of the “PPR-suggestive” patients also had other facial dermatoses, which were recorded.
The SSSB is a sampling method in which 1 cm2 of the superficial part of the horny layer and of the follicular content is collected (Fig. 1, Video S1) (18). In our study, the patient’s skin and the microscope slides were first cleaned with ether and 2 SSSBs were then performed consecutively at the same place, allowing measurement of 2 Dds (D/cm2) (superficial (SSSB1) and deep (SSSB2)). The sum of these 2 values (SSSB1+2) was also noted.
The SSSBs were performed at the site of the main skin lesions, preferably on the cheek, if affected (because the highest Dds have been observed here) (21, 23).
Continuous variables are given as means and standard error of the mean (SEM) (min–max) and qualitative variables as percentages.
Differences in continuous variables were compared between groups using an analysis of covariance (ANCOVA), including age and sex as covariates, followed by Sidak tests for multiple comparisons if required. In the absence of age and sex effects, continuous variables were compared using classical Student’s t-tests or Welch tests in case of variance inequality, or with an analysis of variance (ANOVA) followed by Sidak or Dunnett T3 multiple comparison tests, when required, according to the results of the Levene test for homoscedasticity. Differences in qualitative variables were compared between groups using exact χ2 tests.
Statistical significance was considered when p was < 0.05. All statistical tests were performed using IBM-SPSS (version 22.0) software (IBM Corp, Armonk, NY, USA). Cut-off threshold values were proposed following the criterion of Youden and calculated using MedCalc® V14 (Ostend, Belgium) statistical software.
A total of 1,044 patients were included in the analysis: 254 PPR-suggestive, 590 demodicosis, 180 other facial dermatoses, and 20 healthy controls (Fig. 2). The mean age was 44.6 years (range 7.4–98.3 years; SEM 0.5); 712 (68.2%) were women (Table SI). The mean ages of the healthy controls and the patients with other dermatoses were similar (p = 0.088) as were those of the “PPR-suggestive” and demodicosis patients (p = 0.193).
Fig. 2. Constitution of the 4 groups on the basis of the clinical examination. The number of patients in each group is indicated in orange. a445 pityriasis folliculorum, 80 follicular eczematides, 44 folliculitis, 14 pigmentation (chloasma-like without pregnancy, hormonal disorder or contraceptive pill), 6 isolated inflammatory papules, 1 isolated ocular demodicosis. b70 acne vulgaris, 33 seborrhoeic dermatitis, 10 ulerythema ophryogenes, 7 atopic dermatitis, 8 contact dermatitis, 7 dry skin (+ eczematides), 7 irritation dermatitis, 6 hyperpigmentation, 5 folliculitis, 4 perioral dermatitis, 3 chronic lupus erythematosus, 20 others.
The cheek was the most frequent biopsy site in each group: 19/20 (95%) in the healthy controls, 143/180 (79.4%) for other facial dermatosis, 485/590 (82.2%) for demodicosis and 225/254 (88.6%) for PPR-suggestive patients.
The 2 consecutive SSSBs were generally well tolerated. Mild bleeding occurred in 3 of 1,046 patients (Fig S1): after the first SSSB in 2 patients (for whom the second SSSB was not performed and the patients thus excluded), and after the second SSSB in one patient.
As expected, patients with demodicosis and PPR-suggestive patients had high mean Dds, whereas the healthy controls and patients with other facial dermatoses had low mean Dds (Table I). There were no statistically significant differences in Dds between any of the other facial dermatoses subgroups and the healthy controls. To identify the optimal cut-off values to differentiate between normal and abnormal Dds, the 2 groups with high mean Dds (“PPR-suggestive” and demodicosis) were grouped together as “Demodex +”, and the 2 groups with low mean Dds (healthy controls and other facial dermatoses) were grouped together as “Demodex –” (Fig. 2). Patients in the “Demodex –” group were younger (36.5 ± 0.9 vs. 46.5 ± 0.5 years, p < 0.001) and more likely to be female (75.0% vs. 66.6%, p = 0.023) than patients in the “Demodex +” group (Table SI).
Table I. Demodex densities in the different clinical groups
There were no statistically significant differences in the mean Dds in the 4 subgroups of PPR-suggestive patients (data not shown). Patients with “typical PPR” (215/254) had much higher mean Dds (SSSB1: 90 ± 8.2 D/cm2, SSSB2: 207.5 ± 13.6 D/cm2 and SSSB1+2: 298.5 ± 19.4 D/cm2) than the “Demodex –” group (all p < 0.001), and slightly higher values than the demodicosis group (p = 0.018 for SSSB2, p = 0.034 for SSSB1+2, p = 0.474 for SSSB1).
The mean SSSB2 was significantly higher than the mean SSSB1 in the “Demodex +” and “other facial dermatosis” groups (both p < 0.001) (Table I). The same trend was observed in the healthy controls, but was not statistically significant (p = 0.071).
Among the 844 patients in the “Demodex +” group, 647 had demodicosis or PRR alone and 197 had an associated facial dermatosis (134 seborrhoeic dermatitis, 31 acne vulgaris, 16 both seborrhoeic dermatitis and acne vulgaris, and 16 others). The mean Dds were not influenced by the presence of another facial dermatosis (Table SII). Patients with seborrhoeic dermatitis or acne vulgaris only had a high Dd if they also had demodicosis (Table SIII).
The cut-off Dd values best able to differentiate between the “Demodex +” (n = 844) and “Demodex –” (n = 200) groups were > 5 D/cm2 for SSSB1, > 10 D/cm2 for SSSB2 and > 15 D/cm2 for SSSB1+2 (Table II, Fig. 3). The optimal diagnostic criterion for PPR or demodicosis was found to be the combination of an SSSB1 > 5 D/cm2 or an SSSB2 > 10 D/cm², which had a specificity of 95.5% for the “Demodex –” group and a sensitivity of 98.7% for the “Demodex +” group. This sensitivity was statistically significantly higher than that obtained for the method based on SSSB1 alone (98.7% vs. 89.3%, p < 0.001) (Table II); the decrease in specificity (95.5% vs. 98.5%) was not statistically significant (p = 0.140).
Table II. Cut-off values provided by the comparison of “Demodex +” (n = 844) and “Demodex –” (n=200) groups
Fig. 3. Distribution of the patients according to the cut-off values proposed based on the Youden index: > 5 D/cm2 for standardized skin surface biopsy (SSSB)1, > 10 D/cm2 for SSSB2 and > 15 D/cm2 for SSSB1+2.
To validate this new diagnostic criterion, we also applied it to the 2 groups of patients already known to have high Dd values. The sensitivity was 99.2% for the “demodicosis” group (n = 590) and 98.6% for the “typical PPR” subgroup (with persistent erythema) (n = 215). Thus, with this criterion, only 6 of the 254 PPR-suggestive patients (2.4%) and 3/215 (1.4%) of the typical PPR patients had a normal Dd. Demodicosis with a normal Dd was very rare, occurring in only 5 (0.8%) of the patients. By contrast, there were 9 patients (4.5%) with high Dds in the “Demodex –” group (3/20 healthy controls and 6/180 with other facial dermatosis).
In daily practice, the clinical diagnosis of PPR and demodicosis is not always straightforward: clinical signs are non-specific, sometimes very discrete (e.g. the follicular scales of pityriasis folliculorum), and they can be atypical, mimicking other facial dermatoses. Moreover, these conditions may be present at the same time as other facial dermatoses in the same patient. At present, the diagnosis therefore relies largely on the clinical training and experience of the dermatologist. By developing and validating a more sensitive SSSB for the detection of Dds, we therefore provide a useful diagnostic tool for PPR and demodicosis to assist dermatologists in routine practice.
Our results confirm the cut-off value of > 5 D/cm2 for the SSSB1 that we established in 1993 (18), but also suggest a cut-off of > 10 D/cm2 for SSSB2 and >15 D/cm² for SSSB1+2.
The sensitivity obtained for SSSB1 (89.3%) is higher than that in 1993 (55%) (18). This can be explained by the cleaning of the skin with ether prior to the biopsy. By performing a SSSB2, we further increased the sensitivity by 5% (89.3% to 94.3%), and by combining the cut-off values of the 2 SSSBs in an overall diagnostic criterion (SSSB1 > 5 D/cm2 or SSSB2 >10 D/cm2) we increased the sensitivity by 9.4% (89.3% to 98.7%) compared with a single SSSB, a statistically significant increase. This high sensitivity and specificity may partly be explained by the exclusion of patients with uncertain clinical diagnoses.
We have confirmed, using a more sensitive method in a larger number of patients, that high Dds are associated with demodicosis and PRR, whereas low Dds are found in the skin of healthy subjects and in patients with other facial dermatoses. A limitation of our study could be the differences in age and sex among our patient groups. However, the statistical method used (ANCOVA) corrects for these potential confounders so that the observed differences in Dds cannot be explained by these demographic inequalities. We also showed that normal Dd values are rare in patients with PPR, even rarer than expected: only 1.4% (3/215) compared with 12.5% in 2005 (6/48) (3). This observation, combined with the high mean Dds in patients with PPR, does not formally prove the pathophysiological role of Demodex in PPR, but adds support to this hypothesis. The rare cases of PPR with low Dds may represent false-negative results: for example, they could represent patients with PPR associated exclusively with Demodex brevis, which live inside sebaceous glands and are therefore rarely collected by SSSB. Among the patients with demodicosis, those with low Dd values (0.8%, 5/590) may also represent false negatives or errors in clinical diagnosis.
Sattler and colleagues (25) recently proposed confocal laser scanning microscopy for the measurement of Dd. To compare the results of their study with ours, we converted the Dds expressed “per 8 × 8 mm” and “per 5 × 5 mm” by these authors into D/cm2. Using this crude estimation, 258.4 and 376.8 D/cm2, respectively, would have been found in their PPR patients and 54.2 and 89.6 D/cm2 in their control patients (25). The values they observed in rosacea are comparable with our values for SSSB1+2 (298.5 ± 19.4 D/cm2 for PPR), suggesting that the depth analysed by 2 consecutive SSSBs may be roughly equivalent to the depth analysed by confocal laser microscopy. This also explains why their measured Dds were much higher than those measured previously with only one SSSB. Indeed, our present study shows that the mean SSSB2 was approximately twice the mean SSSB1, suggesting that the majority of the D. folliculorum are located deep in the skin.
By contrast, the mean Dds in their control group far exceeded the values we found. The mean Dds of our healthy controls were very low, even after treating the skin with ether and performing 2 SSSBs, confirming previous findings (18, 21–24, 41–45). This apparent discrepancy probably results from a difference in the selection of the healthy controls. In the present study, we took care not to include patients with pityriasis folliculorum in our healthy controls, a condition that can be very discrete and difficult to identify (7–9, 11).
Confocal laser scanning microscopy requires expensive equipment that is not available to all dermatologists and this technique cannot therefore be proposed as a diagnostic tool in routine daily practice (46). Nevertheless, comparison with our dual SSSB procedure would be interesting and this non-invasive technique should be further investigated, especially for studying Dds in the scalp, where SSSB is not indicated (because of associated pain and the need for prior shaving).
None of our other facial dermatoses subgroups had higher mean Dds than the healthy controls, corroborating prior observations showing low Demodex prevalence (47, 48) or density (41) in lupus erythematous compared with PPR; low prevalence (13, 49–51) and normal Dd (8, 41, 42) in acne vulgaris; no association between presence of Demodex and seborrhoeic dermatitis or atopic dermatitis (52); normal Dds in contact dermatitis (8); no Demodex in the skin or eyelashes of patients with seborrhoeic dermatitis or acne vulgaris contrary to those with rosacea (53); and lower Dds in eyelashes in patients with greasy scales than in those with cylindrical dandruff (54). These observations suggest that Demodex proliferates only in PPR and demodicosis and not in other dermatoses, supporting our hypothesis of a causal relationship in which Demodex drives the inflammatory response: its proliferation is not just an epiphenomenon occurring as a result of an inflammatory process (11, 19).
Although high Dds have been observed in some studies in patients with acne vulgaris (9, 34) seborrhoeic dermatitis (8, 31) or irritation dermatitis (8), it is likely that these patients had undiagnosed pityriasis folliculorum or associated demodicosis. Indeed, dermatologists rarely diagnose demodicosis (7–9) and, moreover, acne vulgaris, seborrhoeic dermatitis and demodicosis fairly commonly occur together in the same patient (Table SII, Fig. 4) (2–6, 8–11, 52, 55). We have observed in clinical practice that seborrhoeic dermatitis only becomes apparent after normalization of the Dd. Although this observation has to be confirmed, this may suggest that Malassezia and Demodex compete, and that when Demodex disappears, Malassezia can proliferate more easily. Demodex may, therefore, not be an aetiological factor in seborrhoeic dermatitis, as suggested by Karincaoglu et al. (31), but rather may benefit from the same favourable environment. Indeed, sebaceous hyperplasia, which favours seborrhoeic dermatitis and acne vulgaris, may also create better living conditions for the Demodex mite (9, 11, 19, 55, 56). Thus, while a high Dd confirms a diagnosis of PPR or demodicosis, it does not exclude the presence of another dermatosis.
In conclusion, our study confirms that high Dds are associated with demodicosis and PRR, while low Dds are found in the skin of healthy subjects and of patients with other facial dermatoses. Although the role of Demodex is not yet established in rosacea and demodicosis, our study suggests that high Dds, measured using the improved sampling method presented, could be a valuable diagnostic tool for all dermatologists in routine clinical practice.
We thank M. Parmentier, V. del Marmol and C. Verhoeven, for their constructive remarks; K. Pickett and P. Strong for proofreading; our patients for agreeing to participate in the study and allowing us to publish their photographs; and all the medical doctors and dermatologists who regularly entrust us with rosacea patients.
FMNF occasionally works as a consultant for Galderma. VdM declares no conflict of interest.


 Click to show fullsize
Click to show fullsize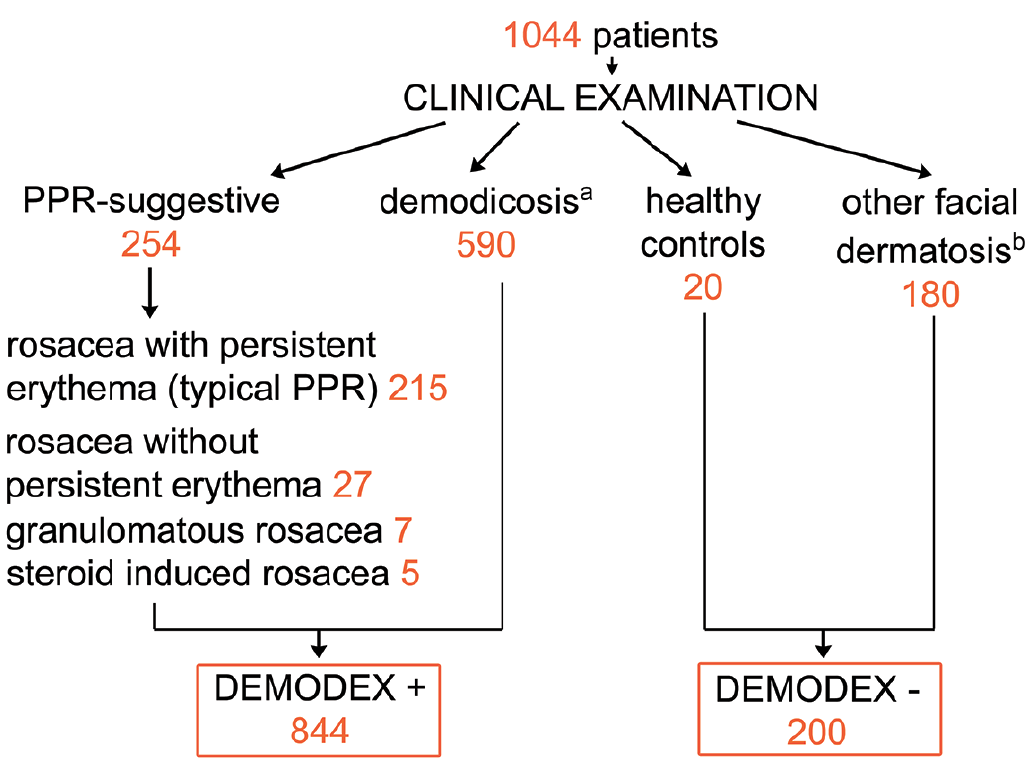 Click to show fullsize
Click to show fullsize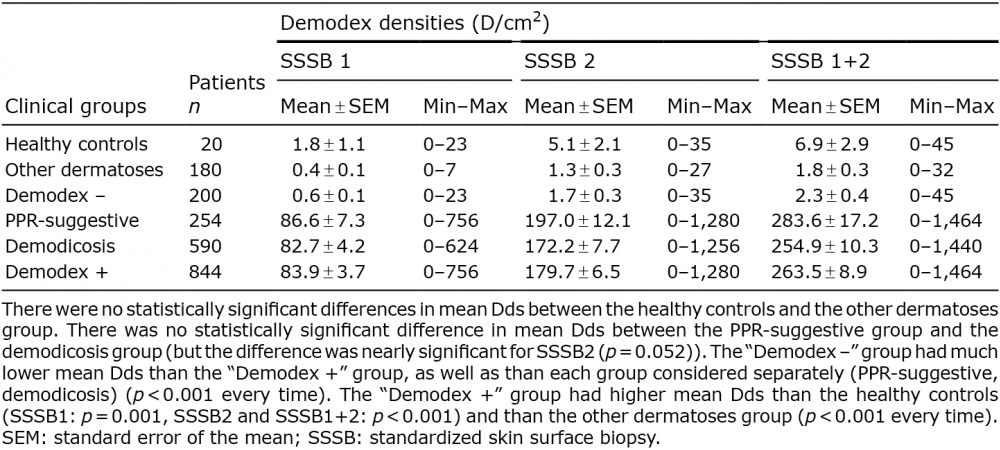 Click to show fullsize
Click to show fullsize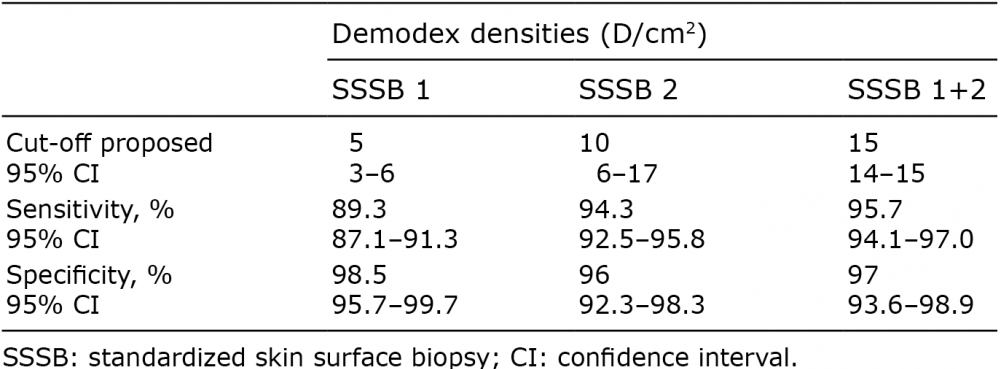 Click to show fullsize
Click to show fullsize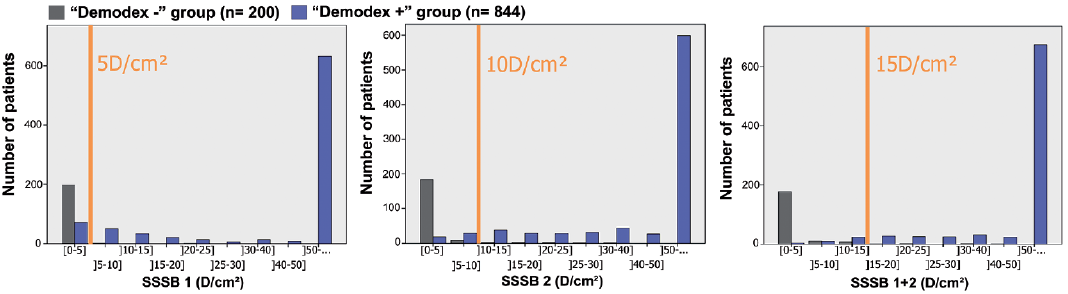 Click to show fullsize
Click to show fullsize