


1Department of Dermatovenereology, Sahlgrenska University Hospital, Göteborg, 2Department of Dermatovenereology, Södra Älvsborgs Hospital, Borås, 3Department of Rheumatology and Inflammation Research (current affiliation Department of Psychiatry and Neurochemistry), University of Gothenburg, Göteborg, Sweden
Lichen sclerosus is a chronic inflammatory disease associated with substantial morbidity. Knowledge of the aetiology and progression of lichen sclerosus is therefore needed. In this cross-sectional study, 100 male patients diagnosed with lichen sclerosus were interviewed and examined. Since there is a possible link between lichen sclerosus and autoimmunity, blood tests were analysed for thyroid disease, antinuclear antibodies and antibodies to extracellular matrix protein 1, but autoimmunity was found to be infrequent. In 72 participants active genital lichen sclerosis was observed and complications were common; 27 patients had preputial constriction and 12 meatal engagement. In total, 13 patients needed a referral to the Department of Urology, including one patient with suspected penile cancer. In conclusion, despite available treatment with ultra-potent steroids and circumcision, lichen sclerosus in males is frequently complicated by phimosis and meatal stenosis. However, the disease can also go into remission, as seen in 27% of our patients.
Key words: lichen sclerosus; circumcision; penile cancer; autoimmunity.
Accepted Sep 19, 2016; Epub ahead of print Sep 27, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Petra Tunbäck, Department of Dermatovenereology, Sahlgrenska University Hospital, SE-413 45 Göteborg, Sweden. E-mail: petra.tunback@derm.gu.se
Lichen sclerosus (LS) is a chronic disease and spontaneous remissions are considered rare. However, adequate treatment can usually control the disease and limit the risk of scarring, dyspareunia, meatal stenosis and malignant evolution. First-line treatment is topical ultra-potent clobetasol propionate, but if the effect is inadequate the next choice in males is circumcision (1). Also, local treatment with tacrolimus can be an alternative (1). The disease is more common in females than males (3–10: 1), but can also be seen in children and middle-aged men (age range 30–50 years) (2). In males, LS is considered to be a disease of the uncircumcised individual, although it can also persist after circumcision (3).
The aetiology of LS is unclear. Studies of females with LS have demonstrated an association with autoantibodies and autoimmune disease (4–6). These reports support the hypothesis of autoimmunity as a pathogenesis of LS in females, but this has not been universally confirmed (7). In men, the link to autoimmunity has not been investigated to the same extent, and instead a main cause is considered to be the occlusive effect of the prepuce. It is also suggested that exposure of the sensitive epithelium of glans and prepuce to urine is a pathomechanism of LS in males (8). Circumcision removes the occlusive effect of the foreskin and reduces the koebnerization and consequences of micro-incontinence after micturition. These observations suggest a sex difference in the aetiological background of LS.
The primary aims of this cross-sectional study of 100 male patients with LS were to investigate the clinical signs and complications of LS in males, the effect of circumcision, and the link between autoimmunity and LS.
The study was approved by the ethics committee of the Medical Faculty of the University of Göteborg, Sweden.
Included participants were invited to provide a blood sample for routine analysis of thyroid stimulation hormone (TSH), thyroxine (T4) and antinuclear antibodies (ANA). In addition, autoantibodies to extracellular matrix protein 1 (ECM-1), a specific skin protein, were analysed, since studies have shown an increased incidence of ECM-1 antibodies in patients with LS (10). The analysis was performed as follows: the plates were coated with 50 ?l/well recombinant human ECM-1 protein (R&D Systems, Minneapolis, USA) diluted to 5 mg/ml in 0.1 M carbonate-bicarbonate buffer at pH 9.8. The plates were incubated overnight at 4°C and blocked with 200 ?l/well of 1% of bovine serum albumin (BSA) in phosphate-buffered saline (PBS) for 30 min at room temperature. Serial dilutions (1/25, 1/50, 1/100, 1/200) of serum samples (diluted in 0.05% PBS-Tween) were incubated for 2 h at room temperature, followed by horse radish peroxidase (HRP)-labelled mouse monoclonal H2 anti-human IgG Fc (Abcam, Cambridge, UK) diluted 1:10,000 in 0.05% PBS-Tween for an additional 2 h at room temperature. Plates were developed for 20 min using 100 ?l/well tetramethylbenzidine in 0.05% phosphate-citrate buffer pH 5.0 containing 0.04% H2O2. The reaction was stopped by adding 25 ?l 1M H2SO4/well. The absorbance was measured at 450 nm with an automated plate reader (Spectra Max 340PC, Molecular Devices) (11). As a positive control HRP-labelled mouse monoclonal IgG1 anti-human ECM-1 from Novus Biologicals (Colorado, USA) was used. Also, 50 sera from males without LS and autoimmune systemic diseases were analysed in the ECM-1 enzyme-linked immunoassay (ELISA). Of these, 44 were uncircumcised, while 6 patients had been circumscribed for religious reasons. This control population was recruited from the Department of Dermatovenereology in Göteborg and they attended for sexually transmitted infection (STI)-screening, but had no ongoing signs or symptoms of an STI.
All data were analysed using R version 3.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). Statistical analyses on the results of the ECM-1 ELISA were performed using Mann–Whitney test. Fisher’s exact test was used to compare proportions. Logistic regression was used to correlate the occurrence of autoimmunity to the degree of activity in LS. All tests are 2-sided and p?<?0.05 was considered statistically significant.
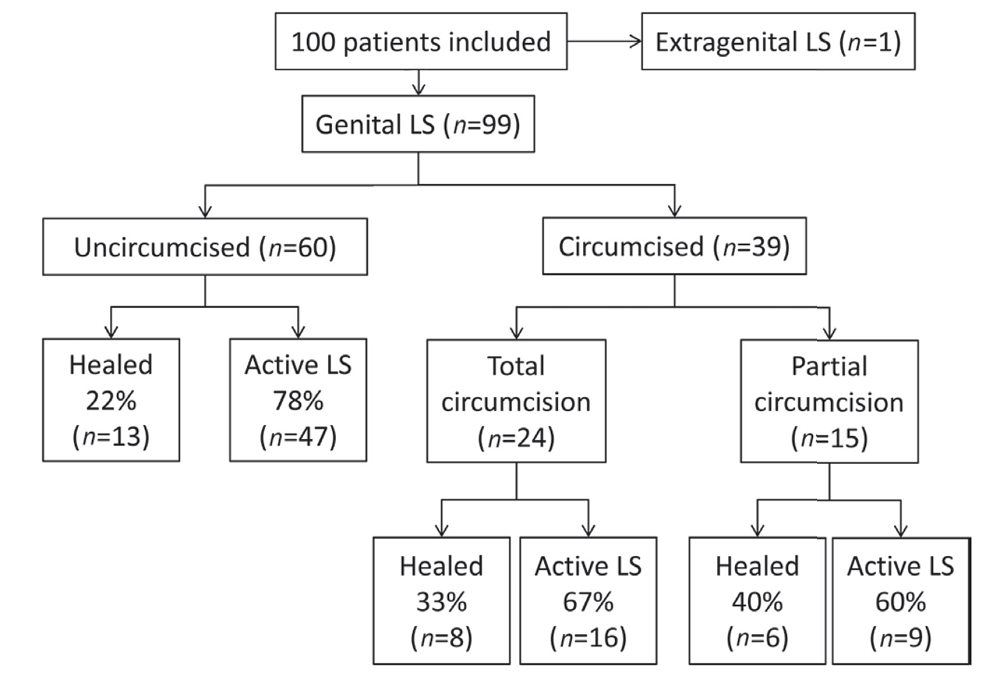
Of all included participants, 99 (99%) had genital LS, including one patient with genital and extragenital lesions. One patient had only experienced extragenital LS. An overview of the included patients is shown in Fig. 1.
Fig. 1. Disease activity in included patients. No statistical difference (p = 0.25) was found between the proportion of healed patients in the 3 groups (total or partial circumcision or un-circumcised patients).
Twenty-eight patients (28%) stated that they were cured when asked, but on clinical examination 4 of these still had active genital lesions; 2 presented with atrophy and ecchymoses in addition to hypopigmentation and 2 patients also had sclerotic, preputial constriction (these 4 were instead included in the group with active LS, see below). Conversely, 4 patients stated that they still had active disease because of remaining hypopigmentation. However, these 4 were included in the group of cured patients after examination and review of the medical history, since they had only experienced hypopigmentation for more than one year. In conclusion, 28 patients had no active LS, and this included the patient with extragenital lesions. In the 27 patients without active genital disease, 14 (52%) had remaining penile hypopigmentation, while 13 (48%) had normal genital appearances without any residues of LS. The mean duration of their disease-period was 5.4 years (range 0.5–20 years) and the mean time since healing was 5.1 years (range 1–14 years).
In the 72 patients (72%) with active LS, 30% had lesions on the glans penis, 26% preputial engagement, and 44% had lesions involving both glans penis and prepuce. None of the patients had lesions on the penile shaft. For localization and clinical description of the lesions, see Table I. None of the included patients had perianal LS, but meatal stenosis was observed in 12 individuals (12%). In 27 patients (27%), the prepuce was constricted and this included 9 males who had been partially circumcised earlier. In 4 patients (4%), the prepuce could not be retracted at all. In total, 13 patients (13%) were referred to the Department of Urology for the following reasons: 8 due to preputial constriction, 4 due to meatal stenosis and 1 due to a clinically suspected penile cancer on the glans penis. The patient with suspected penile cancer was finally diagnosed with penile intraepithelial neoplasia grade II, after total excision of the lesion, and he is still attending the Department of Urology due to repeated dysplasia. Two of the study participants had been diagnosed with penile cancer earlier; a 47-year-old man who had penile cancer in 2006 and a 64-year-old man with penile cancer in 2002 and thereafter 3 recurrences. Neither of these had suspicious malignant lesions at the current medical appointment, but both had active LS even though total circumcision had been performed earlier, at the age of 40 and 37 years, respectively. Both received a prescription of clobetasol propionate and follow-up appointments.
Table I. Clinical description of genital lichen sclerosus in the study subjects
Circumcision had already been performed in 39% (n = 39) of the patients at the clinical examination, and these were all due to phimosis. A total circumcision, with removal of the whole prepuce, had been performed in 24 of the 39 patients (62%). In 15 patients (38%) only a partial circumcision, removing the sclerotic and tight part of the prepuce, had been carried out. When separating individuals with inactive LS into circumcised and uncircumcised the following proportions were considered to be in complete remission: 35.8% of the circumcised individuals and 21.6% of the uncircumcised individuals (p = 0.17).
Extragenital LS had been present in 2 patients (2%). Firstly, a 68-year-old man with one clinically typical LS lesion on his right wrist since 10 years. He also had active genital LS and needed regular urethral dilatation at the Department of Urology. The other patient was 74 years old and had never experienced genital LS, but biopsy verified extragenital LS. His lesions had been localized in both axillae and on the trunk and resolved spontaneously after one year.
Serum samples were obtained from all 100 patients. A positive ANA was found in 5 patients at a low titre of 1/80 with a homogenous pattern, and this was considered to be unspecific after consultation with a rheumatologist. Six patients (6%) were found to be truly positive in the ANA analysis (Table II), but none had arthritis or arthralgia. They were all referred to their general practitioner for follow-up. The patient with antibodies against the mitotic spindle in the ANA-screen (Table II) had pain in his joints, but these were judged as mild and thought to be due to a concurrent hepatitis C infection. The analysis of T4 and TSH showed a mildly abnormal thyroid function in 5 patients (5%) (Table II). None of these had clinical signs or symptoms due to thyroid affection. The analysis of ECM-1 antibodies showed no statistical difference between patients with LS and controls in any of the serial dilutions (all p?>?0.05). No significant difference was seen between patients reacting in any of the autoimmune tests and the degree of activity in their LS (all p?>?0.05).
Of the included patients, 5% (n = 5) declared that they had diabetes mellitus, 8% (n = 8) vitiligo and 1% (n = 1) alopecia areata, but none reported thyroid disease. Twelve percent (n = 12) of the patients stated that a first-degree relative had diabetes mellitus, 3 % (n = 3) vitiligo and 5% (n = 5) thyroid disease, but no cases of alopecia areata were reported in close relatives.
The mean age of the included participants was 51.4 years (range 29–83) and the mean age of the included controls for the ECM-1 analysis was 35.1 years (range 22–61).
Table II. Description of positive results in the serological assays of antinuclear antibodies (ANA), thyroxine (T4) and thyroid stimulation hormone (TSH)
This study examined 100 male patients with LS. A majority of these patients had active LS, but 27% had observed no genital signs or symptoms of the disease for a mean period of 5.1 years. These patients were considered healed and 48% had no visible residues of the disease, while 52% showed remaining hypopigmentation.
However, complications were found to be common, with 27% of patients having preputial constriction and 12% meatal stenosis. When treating patients with LS, cooperation with an urologist is valuable for help with urethral dilatation and, in this study, 4 of 12 patients (33%) with meatal stenosis had to be referred for surgical intervention. Three of these patients had a meatotomy and have not had any recurrences since (noted in April 2016). The fourth patient did not undergo surgery, due to obesity and severe cardiovascular disease, and he is still being treated with regular dilatations at the Department of Urology. In a study by Kulkarni et al. (12), meatotomy was found to have a success rate of 80%, with no recurrences within the mean follow-up period of 56 months. Other possible complications in LS are genital dysplasia and cancer (13). In the present study, one patient had a suspected penile cancer at the time of the appointment and two had been treated earlier for penile cancer. This underlines the need for follow-up of males with LS, and this also applies to circumcised patients if they still have active disease.
Circumcision is not always curative, but often leads to improvement, and is said to be effective in a majority of the patients, as shown by Edmonds et al. (8) where 76% of the patients experienced resolution or stabilization of the disease after circumcision. However, in another investigation half of the men continued to have active LS after circumcision (3). In our study, as many as 64% of patients experienced active LS after partial or total circumcision. We found no statistical significance in patients with inactive disease and circumcision (partial and total) vs. no circumcision (p = 0.17), and the same was true for inactive disease in totally circumcised vs. uncircumcised patients (p = 0.44). Partial circumcision, removing only the constricted part of the prepuce, might be preferred by some patients, but, based on our data, we cannot recommend this. In this population, 15 patients had been partially circumcised and, of these, 9 had developed preputial constriction in their remaining prepuce. Two of these were urgently referred to the urologist for a total circumcision and the remaining group needed treatment with topical ultra-potent steroid.
Extragenital LS is very rarely seen in men, compared with women (8, 9) and, in our cohort, only 2 males had extragenital lesion. Also, in perianal LS there is a sex difference. In our study, none had perianal engagement, which is in agreement with other studies showing perianal LS in females but not in males (14). This difference supports the hypothesis that urine on the sensitive genital epithelium is a contributing cause in male LS. The perianal region in males does not come into contact with urine, but the prepuce and glans are exposed and these are the sites where LS is localized (8). According to this theory, LS is triggered by koebnerization from urine due to micro-incontinence. Circumcision both removes the occlusive effect of the foreskin and reduces the negative effect of micro-incontinence (15), but, in our investigation, a majority of the circumcised patients still had active LS, as already stated. Regrettably, we did not collect data on the presence of incontinence in our patients.
Of the included patients, 9% stated that they had vitiligo, 5% diabetes mellitus and 1% alopecia areata, but none reported thyroid disease. These figures are comparable to the data presented in our earlier study (9) and to the prevalence of autoimmune diseases found in populations without LS, as seen for vitiligo (16), diabetes mellitus (17), alopecia areata (18) and autoimmune thyroiditis (19). In a study by Kreuter et al. (4), LS in males and females was compared with the presence of autoimmune diseases. They showed that females with LS frequently had autoimmune diseases, especially thyroid disease, as well as circulating autoantibodies, but the prevalence in males with LS was even lower than that of the general population. They concluded that “women with LS should be screened for other autoimmune diseases, whereas screening may not be necessary in men”. Edmonds et al. (8) also found that autoimmunity in men with LS was infrequent and their results, as well as ours, strengthens the conclusion that screening for autoimmunity in men is not needed. Our data showed ANA-positivity in 6% of the patients, and this is comparable to data from the general population (20). In our study population, 5% had deviant results in the analysis of TSH and T4, and these results are compatible to levels found in the general population (21). Another theory regarding autoimmunity and the pathogenesis in LS has been the presence of autoantibodies directed at ECM-1, a specific skin protein. This protein is mutated in the rare genodermatosis lipoid proteinosis. Lipoid proteinosis shares some clinical and histological similarities with LS, and this was the starting point for the interest in ECM-1 in LS. However, in our study no difference was found in the prevalence of antibodies to ECM-1 between males with LS and healthy controls. This contradicts the hypothesis that ECM-1 antibodies have a causative role in the pathogenesis of LS. A more plausible role for ECM-1 antibodies, if they are found, is instead that they represent an epiphenomenon, as suggested by Edmonds et al. (22).
This study has both strengths and limitations. It is based on examinations of a heterogeneous group of 100 male patients with LS, some with inactive and some with active disease. A thorough clinical examination was performed, as well as an investigation of autoantibodies and autoimmunity. A weakness is that the control sera in the ECM-1 ELISA did not come from age-matched individuals, but, to our knowledge, anti-ECM-1 antibodies are not correlated with age. More importantly, a selection bias towards a group with more prominent symptoms and severe disease is a risk, based on the way the inclusion was performed, which might lead to overestimations of complications. Also, this is a cross-sectional study without systematic follow-up of patients after topical treatment, urological interventions or on the possible development of autoimmune disease. Another weakness is the lack of data regarding how LS affected the patient’s sexual health. Some individuals mentioned that LS had a negative impact on their self-esteem due to the change in genital appearance inflicted by the disease. However, these data were not asked for in a methodical way and clear conclusions cannot be drawn. In our previous study (9), as many as 56% of subjects noted that LS had a negative impact on their sexual health, which makes this an important issue to address seeing these patients.
The prevalence of autoimmune diseases and autoantibodies was not increased in our population of male patients with LS compared with studies of the general population. Total circumcision was a beneficial treatment for many patients, but the majority still had active LS after this surgical procedure. Complications of LS were commonly seen and close cooperation between the dermatovenerologist and urologist was needed for urethral dilatation, circumcision and in cases with suspected penile cancer. However, it was reassuring to see that the disease had gone into complete remission in 27% of our patients.
The authors would like to thank Anna Månesköld at the Department of Dermatovenereology, Södra Älvsborgs Hospital. This study was supported by grants from The Health & Medical Care Committee of the Region Västra Götaland (VGFOUREG-11763, -148821), the Edvard Welander Foundation and Kristina Stenborgs Stiftelse, Göteborgs Läkarsällskap. The funders were not involved in the design of the study or the interpretation of the data.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize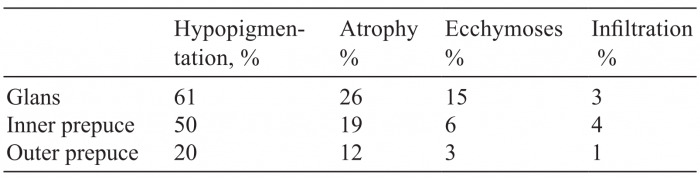 Click to show fullsize
Click to show fullsize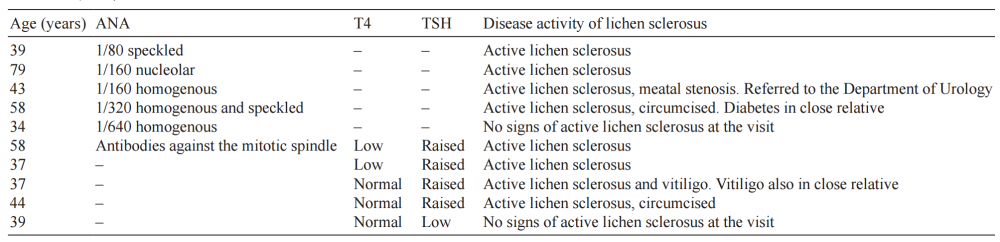 Click to show fullsize
Click to show fullsize