


1Department of Dermatology, and 2Laboratory of Pathology, University of Montpellier, Hôpital Saint-Eloi, 80 avenue Augustin Fliche, FR-34295 Montpellier Cedex 5, France. E-mail: a-du_thanh@chu-montpellier.fr
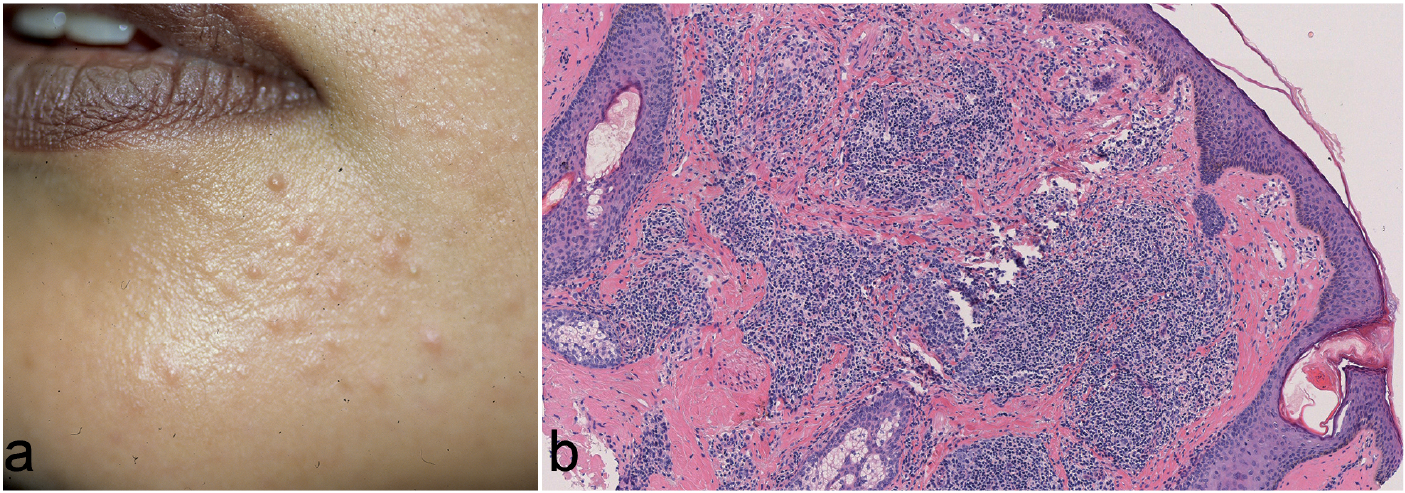
A 31-year-old woman was investigated for multiple, slightly erythematous or flesh-coloured, firm, asymptomatic papules, a few mm in diameter, located exclusively on the chin and the lower part of both cheeks (Fig. 1a). These elements had gradually emerged over the 2 previous years and were initially considered and treated unsuccessfully as retentional acne. Physical examination was otherwise unremarkable and the general status of the patient was excellent. Histological examination of a papule displayed a multi-nodular lymphocytic infiltrate of moderate density involving the upper and medium dermis that was well-limited laterally (Fig. 1b). Standard laboratory investigations and routine serologies, including serological diagnosis of Borrelia, were normal or negative. Computed tomography (CT) scan of the chest, abdomen and pelvis was unremarkable. What is your diagnosis? See next page for answer.
Fig. 1. Clinical and histological features. (a) Multiple, small-sized papules of the lower part of the face with chronic evolution. (b) multi-nodular dermal infiltrate of moderate density involving the upper and medium dermis with reactive germinal centre-like structures (Haematoxylin-eosin ×5).
What is your diagnosis? See next page for answer.
Acta Derm Venereol
On immunostaining, the infiltrate consisted mainly of Bcl2+ B lymphocytes with reactive germinal centre-like structures admixed with a relatively abundant contingent of associated T cells (Fig. 2). Plasma cells displaying a monotypic lambda light chain were scattered especially on the margins of the nodules. Cutaneous clonality could not be accurately investigated on formaldehyde-fixed, paraffin-embedded sample, but there was no dominant B-cell population in peripheral blood. In a homogeneous series of 18, mainly female patients, a particular clinical form of primary cutaeneous B-cell lymphoma, called primary cutaneous follicle centre lymphoma (PCFCL), miliary- or agminated-type was recently described as a stereotyp picture of scattered or grouped elements of small, firm and multiple erythematous papules, mainly involving the neck and face (forehead and cheeks) (1). Although clinically unusual, this specific variant seems to retain the general histological pattern of PCFCL and its indolent outcome with no extracutaneous disease or disease-related death during follow-up. The clinical pattern of facial lesions in the patient described here is very close to those reported in this series, with multiple, firm and slightly erythematous small papules of chronic evolution involving exclusively in the lower part of the face; however, with a different histopathological pattern finally diagnosed as PCMZL. From the same perspective, Barzilai et al. (2) recently reported a series of 12 patients with primary cutaneous B-cell lymphoma including both PCFCL and PCMZL presenting with small papules and nodules on the face (nose, cheeks and periocular areas) mimicking granulomatous rosacea, phymatous rosacea or a combination of both.Thus, it is likely that both main subsets of indolent primary cutaneous B-cell lymphoma can present with this quite misleading clinical pattern.
Fig. 2. Immunophenotyping of skin biopsy showing dominant bcl2+ staining of lymphocytes in the dermal infiltrate (Haematoxylin-eosin ×5).
This peculiar presentation is a significant diagnostic challenge and represents a clinical pitfall. Indeed, differential diagnosis is broad and encompasses numerous inflammatory skin conditions involving the face and presenting with papules of chronic evolution, such as acne, rosacea, folliculitis of various origins, lupus miliaris disseminatus faciei, and papular sarcoidosis, among others. In no case, including ours, was the diagnosis of lymphoma initially proposed, and all of these patients received unsuccessful treatment before a biopsy was finally performed and enabled the correct diagnosis. The diagnosis is often delayed, as a consequence; by 2 years in our patient. As an additional difficulty, a reactive lymphoid hyperplasia or a pseudolymphoma with follicular pattern may be difficult to rule out with certainty due to the relative lack of conclusive, most particularly, structural clues on these small lesions displaying a space-limited infiltrate. Moreover, a marked plasmacytic differentiation and/or a prominent T-cell component, as in our case, may obscure the neoplastic B cells and lead to misdiagnosis (3, 4). Thus, sequential biopsies may prove necessary before a definite diagnosis can be established in these lesions displaying an unusual and misleading pattern. Repeated attempts at systemic treatment (amoxicillin, tetracyclines and hydroxychloroquine) proved ineffective and the patient declined the offer of treatment with thalidomide.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize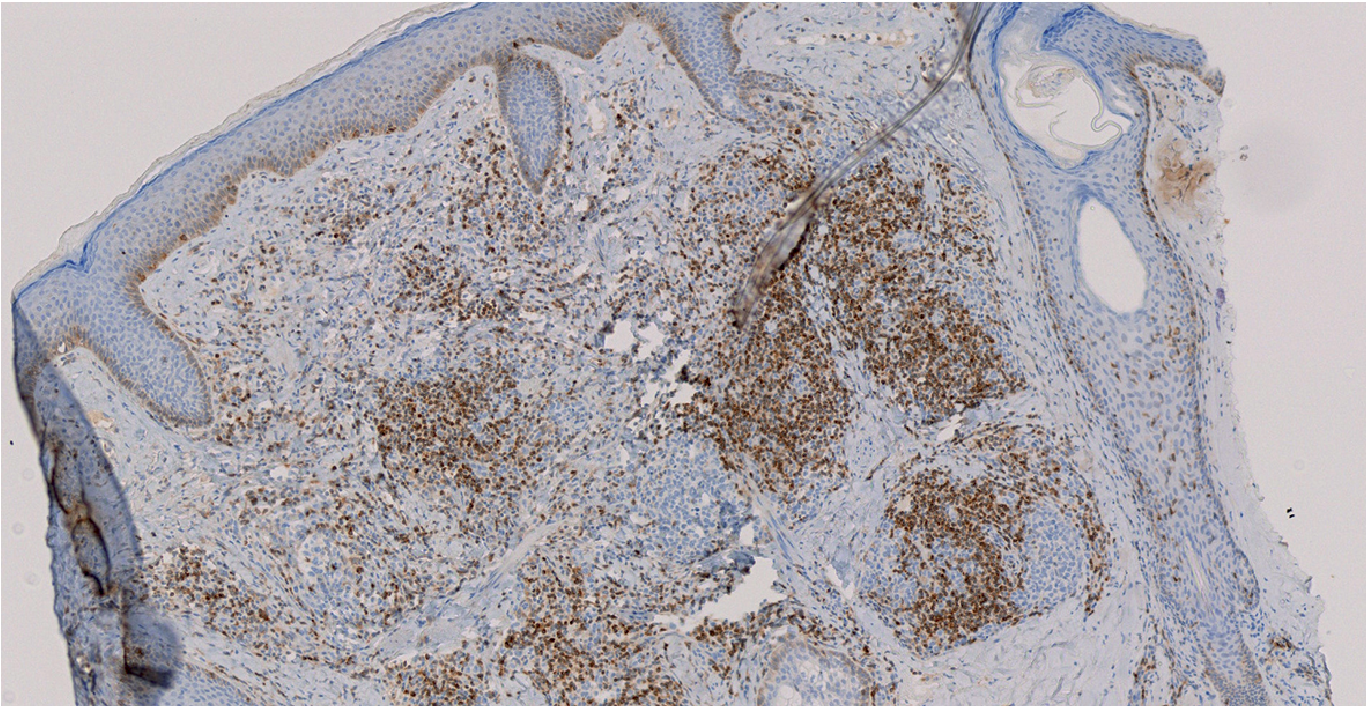 Click to show fullsize
Click to show fullsize