


Department of Dermatology, Kyoto University Graduate School of Medicine, 54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto 606-8507, Japan. *E-mail: hontetsu@kuhp.kyoto-u.ac.jp and kaba@kuhp.kyoto-u.ac.jp
Accepted Oct 6, 2016; Epub ahead of print Oct 10, 2016
Lichen planus (LP) is a T-cell-mediated chronic inflammatory disease that develops in skin and mucosa (1). LP is characterized by band-like lymphocyte infiltration in the subepithelium and necrosis of basal keratinocytes (1). Nivolumab is a monoclonal antibody to programmed death 1 (PD-1), an immune checkpoint molecule. Nivolumab facilitates T-cell activation by cancelling the suppressive effect of PD-1 signalling on T cells. It has been shown to have great efficacy in facilitating T cell activation in various cancers, including, but not limited to, melanoma and breast cancer (2). In addition, the combination of nivolumab with radiotherapy may have synergistic effects (3). We report here a case of LP that developed in the irradiated skin area during administration of nivolumab in a patient with breast cancer.
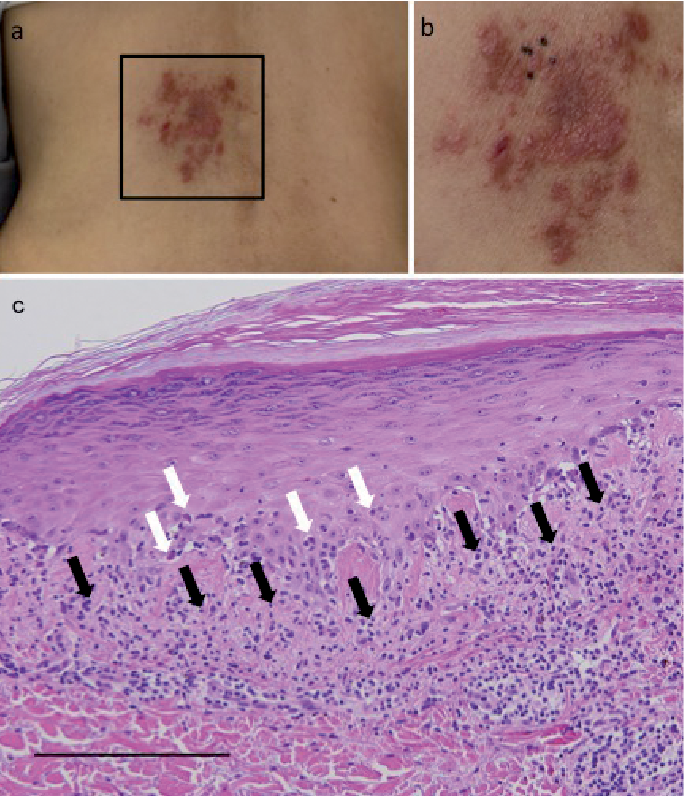
A 67-year-old woman diagnosed with breast cancer was referred to our dermatology department because of purple-coloured skin papules on the middle of her back. She had developed breast cancer and had undergone surgery at the age of 63 years. A liver metastasis was found approximately 18 months after the surgery and chemotherapy (anastrozole and tegafur-uracil). Nivolumab (2 mg/kg) was then started and administered every 3 weeks. Four months after the nivolumab treatment, the patient reported abdominal pain due to the enlargement of lymph nodes in the hepatic portal region. The liver metastasis also progressed slightly. Nivolumab was discontinued, and fractionated radiation to a total dose of 30 Gy was applied to the enlarged lymph nodes. A week after the radiotherapy, nivolumab was restarted. One month after restarting nivolumab treatment, purple-coloured papules developed on her back (Fig. 1a, b). The lesion clearly corresponded to the hepatic portal lymph nodes, which was the area of radiation (Fig. 1a). Histological analysis showed band-like lymphocyte infiltration in the upper dermis, with liquefaction and necrotic keratinocytes in the epidermis (Fig. 1c). The lesion was diagnosed as LP, and topical difluprednate treatment was started (0.05%); however, the LP lesion persisted. Since the enlarged lymph nodes regressed, nivolumab was discontinued once more. After the cessation of nivolumab, the LP lesion gradually improved by treatment with difluprednate ointment and almost disappeared 8 weeks after the last nivolumab treatment.
Fig. 1. A 67-year-old woman with breast cancer. (a) Purple-coloured papules on the middle of the back. Black square indicates the radiation area. (b) Higher magnification image of the lesion. Black dots indicate the biopsy area. (c) Haematoxylin and eosin staining (20×; scale bar 100 µm). Subepidermal lymphocyte infiltrations (black arrows) and a number of necrotic keratinocyte (white arrows) in the epithelium, were seen.
Both nivolumab and radiation have been reported to trigger LP (4, 5). In the current case, the LP did not develop during the first 4 months of nivolumab treatment. However, following radiotherapy, the LP lesion developed one month after restarting nivolumab treatment. The LP lesion was restricted to the irradiated area, and disappeared after the cessation of nivolumab treatment. Therefore, we speculate that both factors were required to fully develop LP in our case.
In LP lesions, the intensive expression of programmed death ligand 1 (PD-L1) on keratinocytes has been reported (6). In animal models PD-L1 on keratinocytes is suggested to play protective roles in interface dermatitis caused by cytotoxic CD8+ T cells (7, 8). The administration of anti-PD-1 antibody significantly increases the production of interferon-γ in patients with oral LP (9). Therefore, anti-PD-1 therapy might cause or exacerbate LP by blocking both the interaction between PD-L1 on keratinocytes and PD-1 on T cells (9). In addition, it has been reported that radiation has an immunological adjuvant effect on tumour immunity through various mechanisms, such as induction of cell death and chemokine production (10). These mechanisms may also contribute to T cell recruitment to the radiation site and trigger LP. Interestingly, psoriasis exacerbation has been recently reported in an nivolumab-treated patient (11).
Although the precise underlying mechanism remains to be clarified, the case reported here suggests that there is a close relationship between anti-PD-1 therapy plus radiotherapy and the development of LP.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize