


1Department of Dermatology, Johns Hopkins University, 601 North Caroline Street, 8th Floor, Baltimore, Maryland, 21287, 2Drexel University School of Medicine, Philadelphia, PA, and 3Department of Dermatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA. E-mail: kmacart1@jhmi.edu
Accepted Oct 12, 2016; Epub ahead of print Oct 14, 2016
Folliculotropic mycosis fungoides (MF) is a rare variant of cutaneous T-cell lymphoma with distinct clinical and histological features that is less responsive to therapy than the classic epidermotropic subtype of MF (1, 2). At any given stage, the folliculotropic variant has a worse prognosis than the epidermotropic variant. Due to the (peri) follicular nature of the neoplastic cells in folliculotropic MF, the T-cell infiltrate is thought to be too deep for penetration of many skin-directed treatments. Topical monotherapy is not currently recommended in the current National Comprehensive Cancer Network (NCCN) (3) guidelines as a mainstay treatment option even in patients with a low burden of disease. There is limited evidence that carmustine topical therapy (also known as bis-chlorethylnitrosourea or BCNU) may be beneficial in the treatment of folliculotropic MF. In this study, we hypothesized that topical carmustine would be a safe and effective treatment option for patients with stages I–III folliculotropic MF.
Thirteen consecutive patients with biopsy-proven, folliculotropic MF (stages IA through IIIB) treated with topical carmustine between 2009 and 2016 in the Cutaneous Lymphoma Clinic at the University of Pennsylvania were included (Figs 1 and FigS1). Review of the patients’ records was approved by the University of Pennsylvania Institutional Review Board. Median age at diagnosis was 60 years (32–80 years). Twelve of the 13 patients were men. At diagnosis, patients were noted to have the following disease stages: IA (n = 1), IB (n = 8), IIB (n = 2), IIIA (n = 1), and IIIB (n = 1) with a median time from diagnosis to initiation of carmustine of 22 months (0–144 months). At the time receiving carmustine, 4 patients were treatment-naïve and 9 patients had disease that was refractory to prior monotherapy or multimodality therapy (Table SI). All 13 patients were treated with carmustine topical therapy as formerly published under the NCCN (3) guidelines following a thorough discussion of the risks and benefits of treatment. Patients were instructed to apply topical carmustine 0.04% ointment to all affected areas. In 9 cases, patients were treated with topical carmustine plus another systemic agent, including low-dose interferon (IFN)-α or γ at 1–2 million units 3 times weekly or low-dose isotretinoin at 10–20 mg daily, while the remaining 4 patients were treated with topical carmustine as monotherapy.
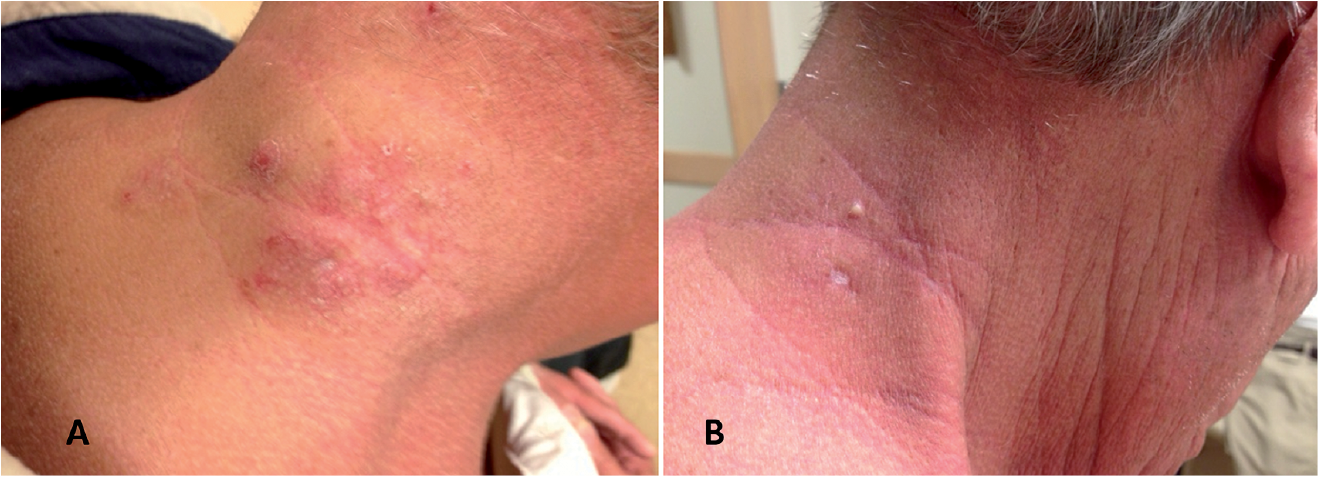
Fig. 1. Folliculotropic mycosis fungoides (MF). A) Neck of patient 11 with folliculotropic MF refractory to topical Nitrogen mustard therapy prior to treatment with topical carmustine and B) after 4 months of treatment with topical carmustine.
The primary endpoint was global response based upon physical examination of skin and nodes and peripheral blood assessment. Partial response (PR) was defined as 50% or greater improvement in involvement. Complete response (CR) was defined as full resolution of lesions on physical examination with no residual visible changes of follicular plugging or active skin lesions. Post-treatment biopsy was not routinely performed. Toxicities were scored using CTCAEv4.0 (Common Terminology Criteria for Adverse Events version 4.0).
Median treatment duration with carmustine was 12 months (3–56 months) in this cohort of 13 patients. Median follow-up was 12 months (3–56 months). Median time to achieve response (either PR or CR) was 4 months (2–8 months).
Nine patients in the study proved to have prior treatment-refractory disease (7 with stage IB, one with IIB, one with IIIB disease), see Table SI. Topical carmustine was used as monotherapy or combined with other treat-ments at the discretion of the treating physician based on the clinical presentation and the clinician’s expert judgment. Typically, if patients presented with progression of disease while receiving other systemic therapies, topical carmustine was started and a multimodality approach was pursued, often using IFNγ. For the 9 patients with previous treatment-refractory disease, all were alive at last follow-up; 5 achieved a CR, and 4 achieved PR (Table SI) at last follow-up. The 4 patients with PR demonstrated ongoing clinical improvement at the time of last follow-up on continued topical carmustine therapy.
For the 4 patients with treatment-naïve disease, stage at diagnosis included: IA (n = 1), IB (n = 1), IIB (n = 1) and IIIA (n = 1). Two patients were treated with topical carmustine monotherapy, and two patients were treated with topical carmustine with concomitant systemic IFNα (Table SI). The treatment decision for monotherapy versus dual therapy was based on the patient’s unique disease characteristics and clinician discretion with combination therapy favored for patients with more extensive or rapidly progressive disease. Of these patients, one achieved a CR and 3 patients achieved PR (Table SI) at last follow-up. All patients were alive and remained on carmustine at last follow-up. The 3 patients with PR demonstrated ongoing clinical improvement at the time of last follow-up.
Topical carmustine was generally well-tolerated. Two patients developed telangiectases (Fig. S2), one with grade 2 telangiectases diffusely involving the trunk and extremities on areas where carmustine was applied, and the other with grade 1 telangiectases. The patient with grade 2 telangiectases underwent a skin biopsy, which ruled out progressive MF and demonstrated only dilated capillary loops. The telangiectases did not regress after one year of follow-up.
This series highlights the long-term safety and efficacy of topical carmustine, not only as part of a multimodality approach, but also as monotherapy for the treatment of folliculotropic MF. Despite its safety and efficacy, topical carmustine is no longer included in the NCCN treatment guidelines for CTCL. We report one of the largest series of folliculotropic MF patients and the only study to date of the utility of topical carmustine in newly diagnosed and treatment-refractory patients with this aggressive CTCL variant. In folliculotropic MF, neoplastic cells demonstrate folliculocentric predilection with or without epidermal involvement (4). Additionally, folliculotropic MF has the ability to undergo CD30+ large cell transformation (5, 6) and to develop extracutaneous involvement (7, 8) warranting a more extensive staging workup at the time of diagnosis even for suspected T1 disease compared to T1 epidermotropic MF (3).
We believe the utility of carmustine can be explained by its mechanism of action which likely includes deeper penetration than topical mechlorethamine. It has also been determined that carmustine has the ability to undergo spontaneous (non-enzymatic) degradation with production of strong electrophiles that cause DNA alkylation and (inter/intra-strand) cross-link formation (9). The electrophilic nature of carmustine may potentially explain its efficacy in this skin lymphoma given the multiple electron-rich targets in skin as well as the role of electrophilic agents for activation of the transcription factor Nrf (Nuclear Respiratory Factor), which is important in the pathogenesis of CTCL (10–13).
Zackheim (13) first reported promising results of topical carmustine in MF patients in 1972 with subsequent studies describing responses to aqueous carmustine, with his latest study (n = 172), demonstrating high responses at 36 months approaching 92% and 64% for MF stages T1 and T2, respectively (14). However, MF is a very heterogenous disease with many subtypes. Our results build upon Zackheim’s observations, with demonstration of a high degree of efficacy for folliculotropic MF. Similar to Zackheim’s published findings, we report the most common adverse effect to be erythematous reaction and development of telangiectases, with one patient demonstrating diffuse involvement of the skin surface. No evidence of bone marrow suppression or secondary malignancy was identified with the use of 0.04% carmustine ointment. Future studies should determine the optimal treatment duration once remission is achieved.
The authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize