


Departments of Dermatology, 1Hokkaido University Graduate School of Medicine, North 15 West 7, Kita-ku, Sapporo 060-8638, Sapporo, and 2Yamagata University School of Medicine, Yamagata, Japan. *E-mail: h-ujiie@med.hokudai.ac.jp
Accepted Oct 26, 2016; Epub ahead of print Oct 27, 2016
Linear IgA bullous dermatosis (LABD) is a rare subepidermal autoimmune blistering disorder in which IgA autoantibodies to the 120-kDa and 97-kDa shed ectodomains of type XVII collagen (COL17, BP180) at the basement membrane zone (BMZ) are most frequently detected (1, 2). The aetiology of LABD remains largely unclear, although associations with drugs, infections and malignancies have been reported (1). As only a few cases of LABD in pregnancy have been reported (3), little is known about the aetiology of such cases. We report here the first case of LABD in a pregnant woman, in which the target epitope of the autoantibodies was identified as the non-collagenous 16A (NC16A) domain of COL17.
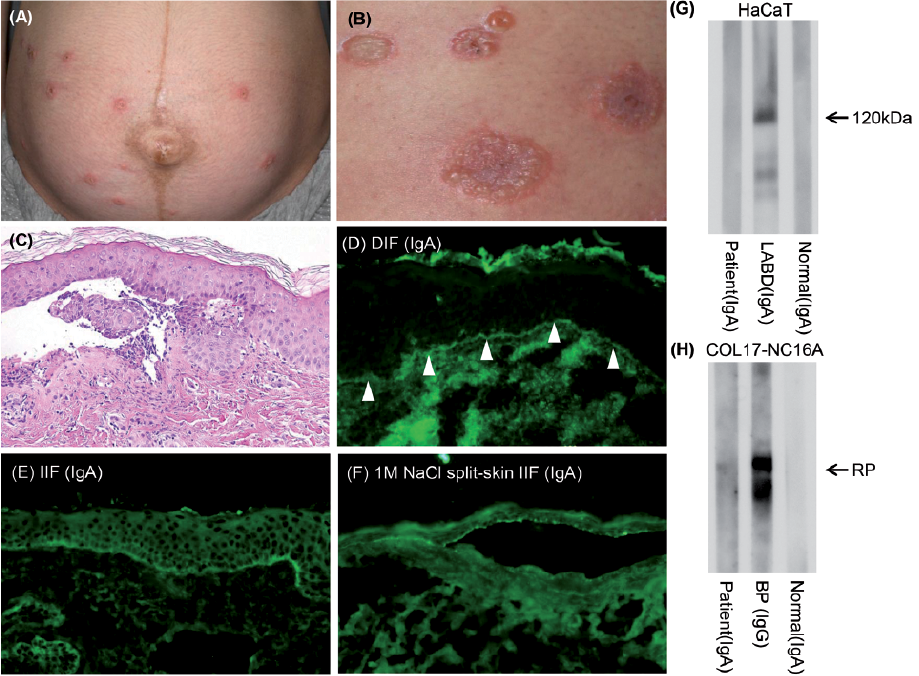
A 29-year-old woman at 38 weeks of her first pregnancy showed a 3-week history of painful pruritic eruptions on the trunk, extremities and lips. The patient had no significant medical history. Physical examination revealed numerous erythematous plaques up to 3 cm in diameter associated with tense blisters in annular arrays on the extremities, abdomen and buttocks (Fig. 1A, B). The mucous membranes were intact, except for multiple erosions on the lips. Serum levels of IgG autoantibodies to desmoglein (Dsg) 1, Dsg3, and the NC16A domain of COL17 measured by chemiluminescent enzyme immunoassay (CLEIA) were not detectable. Histopathologically, a tense blister on the left forearm exhibited subepidermal separation with a mild infiltration of lymphocytes and neutrophils (Fig. 1C). Direct immunofluorescence (DIF) revealed the linear deposition of IgA (Fig. 1D), but not of IgG, IgM or C3 at the BMZ. Indirect immunofluorescence (IIF) for the serum also showed linear deposition of IgA at the BMZ at 8× dilution (Fig. 1E). 1M NaCl-split-skin IIF was positive for IgA on the epidermal side (Fig. 1F). Based on these findings, a diagnosis of LABD in pregnancy was made. To identify the autoantigen that is targeted by the IgA autoantibody, we performed further analyses by Western blotting and enzyme-linked immunoassay (ELISA). Western blotting using a culture supernatant of HaCaT cells and epidermal extracts from a healthy control individual was negative for IgA (Fig. 1G). However, Western blotting using the recombinant NC16A domain of COL17 was weakly positive for IgA (Fig. 1H). By COL17 NC16A ELISA (MBL, Nagoya, Japan) using 1:101 diluted sera and 1:10000 diluted polyclonal rabbit anti-human IgA (Dako, Glostrup, Denmark) as a secondary antibody, the optical density 450 nm (OD 450) in our patient’s serum was significantly higher than that in the sera of normal controls (0.69 ± 0.05 vs. 0.03 ± 0.0003, p < 0.0001). Thus, the circulating IgA autoantibodies in our case were found to react with the NC16A domain, but not with the 120-kDa (LAD-1) shed ectodomains, of COL17.
Fig. 1. Clinical, histological and immunological findings in a patient with linear IgA bullous dermatitis. (A) Oedematous erythema associated with tense blisters on the abdomen. (B) Tense blisters distributed annularly. (C) The histopathology of a tense blister on the left forearm shows subepidermal separation (haematoxylin and eosin ×200). Mild infiltration of neutrophils and lymphocytes is observed (inset). (D) Direct immunofluorescence (DIF) from a blister shows the serration pattern of the linear deposition of IgA at the basement membrane zone (BMZ) (arrowheads). (E) Indirect immunofluorescence (IIF) of normal human skin for the serum is positive for IgA at the BMZ. (F) 1M sodium chloride (NaCl)-split skin IIF for the serum shows linear deposition of IgA on the epidermal side. (G) IgA antibodies in the patient’s serum do not react with a 120-kDa product in the culture supernatant of HaCaT cells, which corresponds to the molecular weight of LAD-1. (H) IgA antibodies in the patient’s serum weakly reacted with the recombinant protein (RP) of COL17 NC16A. Sera of patients with LABD and bullous pemphigoid (BP) were used as positive controls, and sera of a healthy volunteer were used as negative controls (Normal) (G and H).
Oral prednisolone, 20 mg/day (0.3 mg/kg/day), was administered, but new skin lesions continued to appear. Increasing the dose of oral prednisolone to 30 mg/day (0.5 mg/kg/day) led to remission. Her delivery was without complications, and her baby showed neither erythema nor blisters. The oral prednisolone was gradually tapered to 12 mg/day over the course of 2 months after delivery, with a mild relapse of vesicles on the extremities.
The closest differential diagnosis of our case was pemphigoid gestationis (PG), the most common autoimmune subepidermal blistering disorder in pregnancy. The clinical features of PG, such as pruritic urticarial plaques and annularly distributed vesicles, are similar to those of LABD and of our case. In PG, dermal infiltration of eosinophils is common and linear deposition of C3 ± IgG at the BMZ must be observed in perilesional skin by DIF (4). Due to the absence of these findings, we distinguished PG from our case.
LABD in pregnancy has rarely been reported. According to a case series of LABD in pregnancy, the disease usually improves by the end of the first trimester (3). In only one case did the patient experience serious problems during labour and blister formation on the neonate (3). A relapse occurred in 75% of patients within 4 months after delivery, and it was usually worse than the initial episode and required an increased dose of medication (3). As our patient still shows new skin lesions even with oral predonisolone at 15 mg/day, we should carefully follow up the patient.
To our knowledge, this is the first case of LABD in pregnancy in which the autoantigen was identified. Interestingly, the circulating autoantibodies in our case targeted the NC16A domain of COL17, but not the 120-kDa shed ectodomains of COL17, which is a common autoantigen in LABD. Although shed ectodomains of COL17 are known to be the major autoantigens of LABD, it has been reported that IgA autoantibodies in 22% of LABD cases can react to the NC16A domain of COL17 (5, 6). The vast majority of IgG autoantibodies react to the NC16A domain of COL17 in PG cases (7). Although the precise pathomechanism of PG has not been fully elucidated, aberrantly expressed human leukocyte antigen (HLA) class II molecules in the placenta, certain HLA types, and hormones, such as oestrogen and progesterone, are considered to be relevant to a breakdown of the immunological tolerance of the mother to the fetoplacental unit, which results in the production of IgG autoantibodies to the NC16A domain of COL17 (8, 9). We presumed that PG and LABD in pregnancy have overlapping pathomechanisms that may explain why the IgA autoantibodies in our case targeted the NC16A domain rather than the shed ectodomains of COL17. In conclusion, the present case shows that IgA autoantibodies to the BMZ can be produced during pregnancy.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize