


1Department of Dermatology, CHRU Montpellier, 80 avenue A. Fliche, FR-34295 Montpellier cedex, 2University of Montpellier, and 3INSERM U1058, Montpellier, France. E-mail: n-raison@chu-montpellier.fr
Accepted Nov 2, 2016; Epub ahead of print Nov 2, 2016
In the new classification of chronic urticaria, two distinct subtypes have been proposed including spontaneous urticaria and inducible (or physical) urticaria (1). By definition, chronic inducible urticaria (CIndU) is elicited by a specific trigger, such as sunlight, water, sustained local pressure, vibration, hot or cold environments.
Follicular traction urticaria (FTU) is characterized by the development of follicular urticarial papules exclusively after being triggered by hair traction or removal (2, 3).
We suggest that FTU could be a new form of CindU but further studies are needed.
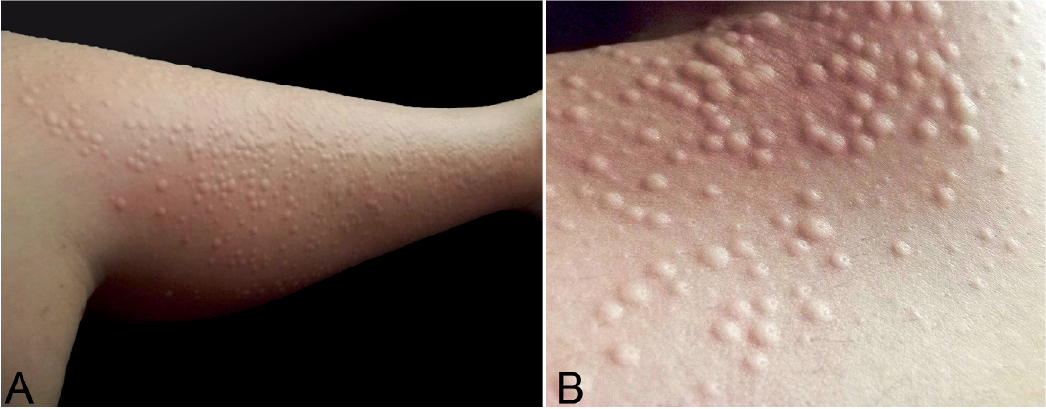
We report here a case of a patient with progressive and long-lasting hives after follicular traction. A 19-year-old woman presented with a 2-year history of pruritic eruption composed of several hundred follicular papules, sometimes confluent, and initially erupting only on her legs and pubic area within 15–30 min of waxing or using an electric epilator (Fig. 1). Three months before consultation, she developed the same eruption by plucking her armpit hair and eyebrows, but to a much lesser extent. Most of the papules were flesh-coloured or pink-red, dome-shaped with a central umbilication, sometimes with a central hair emerging.
Fig. 1. Follicular traction urticaria. (a) Follicular flesh-coloured dome-shaped papules occurring within 15–30 min after hair removal on the lower leg with electric epilator. (b) Close-up of the papules reveals inconstant central umbilication, sometimes with a central hair emerging.
Spontaneous and complete resolution of the eruption was always observed 15–18 h later. She experienced no pruritus or eruption on hairless skin, whatever the hair-removal system used, including mechanical shaving, wax or electric epilator. There was no personal or familial history of spontaneous chronic urticaria or other chronic inducible urticaria (CIndU), particularly vibratory angioedema or symptomatic dermographism. She denied taking any drug and had no other medical issues except hay fever. Physical examination revealed no abnormalities. Hair-removal testing on a small area of her right leg with an electric epilator led to small follicular itchy papules of 1–5 mm within 15 min. Histological examination of a biopsy specimen from a follicular papule was consistent with urticaria with rare dermal eosinophils. Tests for other forms of follicular inducible urticaria, especially heat, vibration, pressure or dermographic stroking with a Fric Test on the fore-arm and leg were negative (4). Desloratadine 5 mg, two tablets, 1 h before and then again immediately after the use of the electric epilator, reduced the duration but not the intensity of the eruption.
Only 2 cases of FTU have been reported in the literature (1, 2), both displaying many similarities with our case: female sex, young age (25 and 32 years old), absence of urticarial background, immediate or rapid (10 min) triggering of the eruption after follicular traction or epilation by waxes, electric epilator or tweezers, absence of apparent underlying infections or autoimmune disease, skin biopsy findings consistent with urticaria, and reproduction of the follicular urticarial papule after a hair-traction test. However, our observation appears original because of: (i) the persistence of symptoms (more than 15 h) before spontaneous resolution, as opposed to the 2 earlier cases with eruption persisting less than 3 h; and (ii) the initial localization of FTU on the bikini area for approximately 2 years before the involvement of armpits and eyebrows area. This initial localized feature with restricted anatomical distribution to the lower body area remains unexplained in the absence of an obvious contributory factor. Main differential diagnosis are transient non-itchy papules after epilation and symptomatic dermographism, especially when it is follicular, but the provocation test with the Fric Test was negative in our patient.
Furthermore, CIndU is elicited by a specific trigger, and must be confirmed by provocation/challenge and assessment of threshold (1). In our opinion, FTU, which is probably due to stimulation of perifollicular mast cells exclusively after hair traction or removal could be recognized as a specific type of CIndU; however further studies are necessary.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize