


1Department of Dermatology, Lewis Katz School of Medicine, Temple University, Philadelphia, 2College of Medicine, University of Tennessee Health Science Center, Memphis, USA, 3Biostatistics Unit, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, and 4Department of Dermatology and Itch Center, Leonard M. Miller School of Medicine, University of Miami Health System, 1600 NW 10th Avenue, Rosenstiel Medical Science Building – Room 2023, Miami, FL 33136, USA. E-mail: Yosipog@gmail.com
Accepted Nov 2, 2016; Epub ahead of print Nov 2, 2016
Chronic pruritus is a distressing condition with a lifetime prevalence of 25.5% (1). Itch is often reported to be especially bothersome during the evening and at night. Nocturnal pruritus (NP) is a reported feature of both dermatologic and systemic conditions and can interfere with the initiation and maintenance of sleep, resulting in deleterious effects on health, functionality, and emotional wellbeing (2, 3). In adults with atopic dermatitis (AD), sleep deficits attributable to NP have been shown to profoundly affect quality of life (QoL), functional ability, and cognition (4). In patients with psoriasis, NP has been implicated as a cause of decreased work productivity (5). Furthermore, in hemodialysis patients, pruritus and related sleep disturbances have been associated with a 17% increased mortality risk (6). However, specific, in-depth studies of NP are lacking. We used validated questionnaires to determine the prevalence, characteristics, severity, and impact on QoL of NP in the chronic itch patient population (7, 8).
This study was conducted from April 2015 to March 2016 in the outpatient clinic at Temple Itch Center. All English-speaking individuals between the ages of 10 and 100 with a diagnosis of chronic pruritus were eligible to participate. Chronic pruritus was defined as itch present for ≥ 6 weeks (9). Subjects with dementia were excluded from participation. This study was approved by the Temple University Institutional Review Board, and signed informed consent was obtained from each participant.
A total of 160 subjects with a mean ± SD age of 57 ± 16 were included in the study. Ninety-seven (60.6%) participants were female, and 63 (39.4%) were male. Subjects were identified as Caucasian (65.6%), African American (23.1%), Hispanic/Latino (5.6%), Asian (1.9%), and other (3.8%).
All participants were asked to complete two validated questionnaires: the itch questionnaire (7) and the itch quality of life survey (ItchyQoL) (8). The itch questionnaire assessed the severity of itch and several associated characteristics, including the presence and severity of NP and the degree of sleep disturbance. Overall ich severity was quantified using an 11-point numeric rating scale (NRS) anchored at 0, representing “no itching,” and 10, representing “worst itch imaginable.” Itch characteristics, including itch severity at different times of day, were measured on a scale anchored at 0 (not at all), 1 (to a minimal extent), 2 (to a mild extent), 3 (to a moderate extent), and 4 (to a great extent).
The ItchyQoL questionnaire contained 21 pruritus-specific items divided into 3 major subscales: Symptoms, Functioning (functional limitations), and Emotions (8). Participants were asked to rate each item on a scale anchored at 1 (never), 2 (rarely), 3 (sometimes), 4 (often), and 5 (all the time). Analysis of the ItchyQoL consisted of individual item scores, subscale scores, and an overall score. Higher scores indicated a lower QoL.
Each participant was examined and diagnosed by an attending physician in the dermatology department. Data pertaining to comorbid conditions were extracted from patient medical records.
All statistical analyses were performed using PASW 18.0 software (SAS, Chicago, IL, USA) with statistical significance set at p < 0.05. Descriptive statistics for quantitative variables were presented as mean ± standard deviation and as percentages for qualitative variables. Differences in quantitative outcomes were assessed using parametric tests when normality and homogeneity assumptions were satisfied; otherwise the equivalent non-parametric tests were used. Correlations were assessed using the nonparametric measure of Spearman’s rank correlation.
NP was present in 146 (91.3%) of the 160 subjects. The mean ± SD overall itch severity among subjects with NP (8.2 ± 2.1) was not significantly different from that of subjects without NP (6.8 ± 2.6). The prevalence and severity of NP were similar among different dermatologic conditions (Table SI). NP was not found to be significantly associated with age, sex, ethnicity, or the presence of comorbid conditions such as depression.
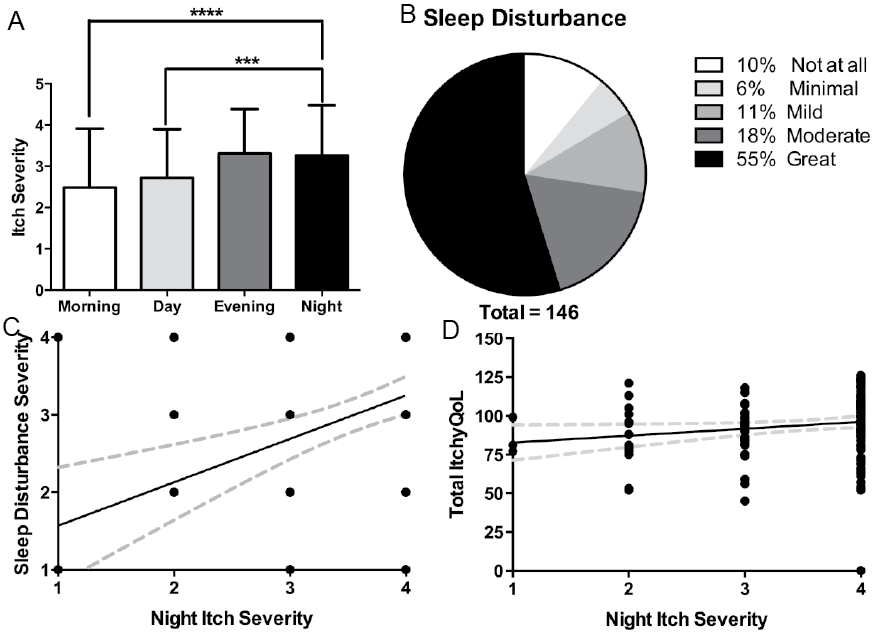
The severity of NP was significantly correlated with overall itch severity (r = 0.22, p = 0.006). On average, subjects reported significantly higher itch severity at night compared to morning or day (p < 0.0001, Fig. 1A).
Fig. 1. Characteristics of nocturnal pruritus (NP) and its correlation to sleep disturbance. A) Temporal variation in itch severity, *** p < 0.001, **** p < 0.0001. B) Degree of sleep disturbance reported by subjects with NP. C) Correlation between sleep disturbance severity and NP severity, rated as 0 (not at all), 1 (to a minimal extent), 2 (to a mild extent), 3 (to a moderate extent), or 4 (to a great extent). D) Correlation of NP severity and overall ItchyQoL score.
69 (47.3%) subjects with NP experienced itch constantly throughout the night. Of the 146 subjects with NP, 90% reported sleep disturbance, with 55% “to a great extent” (Fig. 1B). Furthermore, for subjects with NP, the severity of itch at night was significantly correlated with the severity of sleep disturbance (r = 0.35, p < 0.0001, Fig. 1C). In turn, the severity of sleep disturbance was correlated with feelings of anger and irritability (r = 0.32, p = 0.0001) as well as depression and sadness (r = 0.19, p = 0.03).
The severity of NP was significantly correlated with total ItchyQoL score (r = 0.22, p = 0.006, Fig. 1D), indicating that NP was associated with an overall reduced QoL. Specifically, the severity of NP was correlated with Functioning (r = 0.29, p = 0.0004) and Emotions (r = 0.18, p = 0.03), but not Symptoms (r = 0.15, p = 0.08) subscales.
This study demonstrates that NP is highly prevalent within a wide range of pruritic conditions. Our results corroborate previous reports that have highlighted the significance of NP in atopic dermatitis and psoriasis (4, 5). We additionally found that NP was prevalent in patients with brachioradial pruritus, prurigo nodularis, and chronic spontaneous urticaria (10). Almost all subjects with NP reported some degree of sleep disturbance, and this sleep disturbance was correlated with negative emotional states. The impact of NP on QoL highlights the need for targeted clinical intervention.
Available therapeutic options for the treatment of NP remain limited. First generation antihistamines are commonly used to provide sedation, but otherwise have little ability to relieve chronic itch. Medications with dual antipruritic and soporific effects, including mirtazapine, GABAergics (gabapentin and pregabalin), and kappa opioid agonists (butorphanol) may be able to simultaneously target both itch and sleep impairment (11, 12). We found a correlation between overall itch severity and NP severity, which suggests that using antipruritic agents to treat itch generally should impact NP as well. However, some antipruritic drugs may cause side effects that disturb sleep. For instance, nalfurafine, which is licensed in Japan to treat pruritus associated with chronic kidney disease, has been shown to reduce NP, but may also cause insomnia (13).
There are a number of limitations to our study. Notably, our subjects were recruited from a specialized itch center within a dermatology clinic and may therefore represent more severe cases of chronic pruritus than would routinely be seen in other settings. Additionally, some dermatological pruritic conditions were not well represented within our sample, and we did not investigate the role of NP in the context of pruritic systemic conditions, such as chronic kidney disease and cholestasis.
Despite these limitations, this study shows the important role of NP in QoL for the general chronic itch population. Our results confirm those of previous studies that show itch is usually more severe at night than during the day. The reasons behind this effect are still unclear. Further studies are needed to determine the underlying pathophysiology and central mechanisms that mediate nocturnal itch, with the ultimate goal of ushering in novel targeted therapies.
Conflicts of interest: ML, CS, LAN, KMS, HL, SS, RV-R, and Y-HC declare no conflicts of interest. GY is consultant, principle investigator, or scientific advisory board member for Trevi Therapeutics Inc. (TREVI), Opko, Creabilis, Chugai, Pfizer, Anacor, Celgene, Eli Lily, Johnson & Johnson, Cara, Tioga, Allergan, Glaxosmithkline (GSK)-Stiefel, and Leo Pharma (LEO) Foundation.


 Click to show fullsize
Click to show fullsize