


1Clinical Epidemiology Unit, Istituto Dermopatico dell’Immacolata (IDI)-IRCSS FLMM, Rome, Italy, 2Department of Dermatology, Justus Liebig University, Giessen, Germany, 3Department of Psychology, University of Zaragoza, Aragon Health Sciences Institute, Zaragoza, Spain, 4Department of Public Health, Hedmark University College, Elverum, Norway, Departments of Dermatology, 5Notre-Dame de Grâce Clinic, Gosselies, Belgium, 6Zealand University Hospital, Roskilde, University of Copenhagen, Copenhagen, Denmark, 7University Hospital of Brest, Brest, France, 8Department of Dermatology and Allergology, University of Szeged, Szeged, Hungary, 9Section of Biostatistics, University of Oslo, Oslo, Norway, 10Department of Health, Medical and Neuropsychology, Leiden University, Leiden, The Netherlands, Departments of Dermatology, 11Oslo University Hospital and Institute of Clinical Medicine, University of Oslo, Oslo, 12Stavanger University Hospital, Stavanger, Norway, 13Wroclaw Medical University, Wroclaw, Poland, 14Department of Psychiatry and Psychosomatics, I. M. Sechenov First Moscow State Medical University, Mental Health Research Center, Moscow, Russia, Departments of Dermatology, 15Alcaniz Hospital, Alcaniz, Spain, 16Sisli Etfal Teaching and Research Hospital, Istanbul, Turkey, 17Cardiff University School of Medicine, Cardiff, UK, 18Department of Pharmacy, Pharmacology and Postgraduate Medicine, School of Life & Medical Sciences, University of Hertfordshire, Hatfield, UK, 19Institute of Medical Psychology, Justus Liebig University, Giessen, Germany, and 20Department of Dermatology and Venereology, Skåne University Hospital, Lund University, Malmö, Sweden
#These authors contributed equally to the study.
Skin conditions may have a strong impact on patients’ sexual life, and thus influence personal relationships. Sexual issues are difficult to discuss directly in clinical practice, and a mediated instrument may be useful to capture such information. In this study item 9 of the Dermatology Life Quality Index was used to collect information on sexual impact of several skin conditions in 13 European countries. Among 3,485 patients, 23.1% reported sexual problems. The impairment was particularly high in patients with hidradenitis suppurativa, prurigo, blistering disorders, psoriasis, urticaria, eczema, infections of the skin, or pruritus. Sexual impact was strongly associated with depression, anxiety, and suicidal ideation. It was generally more frequent in younger patients and was positively correlated with clinical severity and itch. It is important to address the issue of sexual well-being in the evaluation of patients with skin conditions, since it is often linked to anxiety, depression, and even suicidal ideation.
Key words: skin; quality of life; sexual impairment; hidradenitis suppurativa; Dermatology Life Quality Index.
Accepted Nov 2, 2016; Epub ahead of print Nov 6, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Francesca Sampogna, Clinical Epidemiology Unit, Istituto Dermopatico dell’Immacolata (IDI)-IRCCS FLMM, Via dei Monti di Creta 104, IT-00167 Roma, Italy. E-mail: fg.sampogna@gmail.com
Sexual life is an important component of health-related quality of life. Skin conditions may have a strong impact on this component, since they involve appearance, and thus affect social life and personal relationships. Several studies have investigated the impact of venereological and dermatological diseases with genital localization on sexual life (1–3). However, regardless of the localization of the affected body area, the involvement of skin in a disease may have consequences on intimacy (4, 5).
In clinical practice, it may be challenging for both the patient and the physician to discuss sensitive issues directly, so the impact of a disease on sexual life is rarely assessed. Self-assessment using questionnaires may provide a viable alternative. Several specific questionnaires aimed at measuring sexual quality of life are available (6), and even a single question from a generic or disease-specific quality of life instrument may yield some important information.
A relevant issue in the interpretation of studies on quality of life in general, and of the impact of skin diseases on sexual life, derives from the vast cultural and methodological variations between countries and study design, as well from the use of different questionnaires.
Therefore, we planned a multicentre European initiative to provide insight on the impact of skin diseases on quality of life and psychological wellbeing, using a single study design with standardized procedures and common research tools (7). The aim of the present study was to investigate the perceived impact of several dermatological conditions on patients’ sexual life, using item 9 of the Dermatology Life Quality Index (DLQI) (8), across clinical and demographic variables in 13 European countries.
Data presented in this report come from a large, cross-sectional study on the psychological burden of skin diseases conducted in 13 European countries. The materials and methods were described in detail in the main paper (7). In brief, complete data were collected on 3,635 consecutive, dermatological out-patients, and 1,359 healthy controls. The present report, being focused on the impact of skin diseases on the patients’ sexual life, is based on data collected from the dermatology-specific instrument DLQI, and therefore considers only the out-patients’ sample. The inclusion criteria were: age 18 years and over; able to read and write the local language; and not having any severe psychiatric diseases. Each patient was examined by a dermatologist who recorded the diagnosis and the presence of other physical conditions. Patients completed a questionnaire including socio-demographic variables. The Hospital Anxiety and Depression Scale (HADS) (9, 10) was used to evaluate the presence and severity of depression and/or anxiety in patients. It includes 7 items assessing anxiety and 7 assessing depression, each with 4 possible answers. For each dimension of anxiety and depression a score from 0 to 7 is considered a normal case, from 8 to 10 a borderline case, and from 11 to 21 a case in need of further examination or treatment. The clinical severity of the skin condition was evaluated by the physician as either “mild”, “moderate”, or “severe”.
The sexual impact due to the skin condition was evaluated using item 9 of the DLQI (8). The question is: “Over the last week, how much has your skin caused any sexual difficulties?”, with the possible answers “very much” (3), “a lot” (2), “a little” (1), “not at all/not relevant” (0).
The frequency of each answer for the different dermatological conditions was calculated, and the association of sexual impairment with different variables was studied, including socio-demographic (sex, age, “living in the country of origin”, education, marital status, geographical region) and clinical information (clinical severity of the skin condition, body site, and itch). The answers to item 9 were grouped in order to have a dichotomous variable “yes/no” (answers “very much” [3], “a lot” [2], and “a little” [1] vs. “not at all/not relevant” [0]). Countries were grouped into Northern Europe (Denmark, Norway), Western Europe (Belgium, France, Germany, The Netherlands, UK), Eastern Europe (Hungary, Poland, Russia, Turkey), and Southern Europe (Italy, Spain). Frequencies were compared using the χ2 test.
Logistic regression models were tested for some diseases selected on the basis of the number of patients (eczema, psoriasis, acne), and/or the strong prevalence of sexual problems (blistering disorders). The diagnosis “eczema” included atopic dermatitis, eczema, and hand eczema. The dichotomous variable DLQI_9 (presence/absence of sexual difficulties) was introduced in each model as the dependent variable. The independent variables were age, sex, clinical severity, European region, flare on scalp, flare on hands, itch, anxiety, and depression.
Data were complete for both question 9 of the DLQI and diagnosis in 3,485 patients. The 114 patients with a diagnosis, but with no answer to question 9 of the DLQI were older than patients who answered the question (mean age 56.8 vs. 46.8 years among patients who did not answer and who answered question 9, respectively, p < 0.001), and included more women (65.8% vs. 56.1%, p = 0.027). Overall, 11.7% of patients reported sexual difficulties “a little”, 5.5% “a lot”, and 5.9% “very much”. Spearman’s correlation between item 9 and the DLQI total score was 0.558. We also verified the correlation between item 9 and the sum of all the other DLQI items: the Spearman’s correlation coefficient remained in the “moderate” range, although at a lower level (i.e. 0.501).
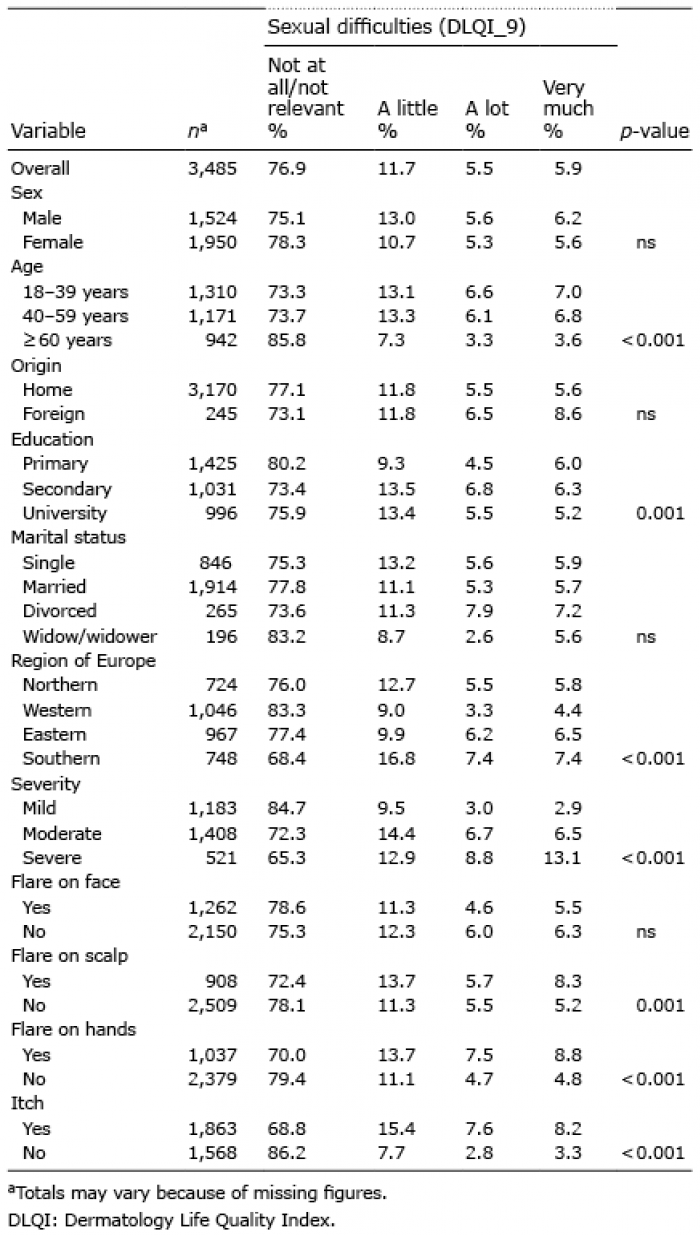
As shown in Table I, there was no significant difference between men and women, while sexual impairment was reported more frequently by younger patients. No differences were observed in patients with different marital status and different origin (i.e. either coming from a foreign country or not). In Southern countries the prevalence of sexual difficulties was significantly higher compared with the other geographical areas. In patients with a clinically severe condition, the prevalence of sexual problems was 3 times more frequent among patients answering “a lot”, and 4 times more frequent for those answering “very much” compared with patients with a clinically mild condition. Also, flares on the scalp and on the hands, as well as itch, were significantly associated with sexual problems.
Table I. Prevalence of sexual difficulties in the study population according to demographic and clinical variables
Sexual difficulties were strongly associated with both depression and anxiety (Table II). For example, among depressed patients, 24.3% reported sexual difficulties “a lot” or “very much”, compared with 7.3% of non-depressed patients. For anxiety the percentages were, respectively, 20.7% and 5.9%. Among patients who reported thoughts of suicide due to their skin condition 30.5% reported sexual difficulties “very much”, compared with 9.9% of patients who did not have thoughts of suicide.
Table II. Frequency of sexual difficulties in the study population according to mood disorders
As shown in Fig. 1, which summarizes the prevalence of the answers “a lot/very much/a little” to question 9 of the DLQI, the impairment was particularly high in patients with hidradenitis suppurativa (66.7%). Other diagnoses with a prevalence greater than 1/3 were prurigo (41.7%), blistering disorders (34.9%), and psoriasis (34.8%); these were followed by urticaria and eczema (both at 29.0%), infections of the skin (27.7%), and pruritus (27.6%). The lowest prevalence was reported by patients with non-melanoma skin cancer (6.1%), naevi (6.4%), benign skin tumours (10.8%), and melanoma (12.8%).
Fig. 1. Prevalence of positive answers to question 9 of the Dermatology Life Quality Index (DLQI) (“Over the last week, how much has your skin caused any sexual difficulties?”) in different skin conditions. NMSC: non-melanoma skin cancer.
When studying the role of sex in the different skin conditions, it was observed that in patients with acne the impact on sexual life was higher in men than in women (23.5% of positive answers to item 9 and 12.2%, respectively, p < 0.05). For all the other conditions, the difference between men and women was not significant. The higher impact on sexual life observed overall in younger patients was significant only in patients with psoriasis (38.2% of positive answers in patients up to 60 years old, and 21.6% in patients older than 60 years, p < 0.05), with blistering disorders (47.1% and 23.1%, respectively, p < 0.05), and with eczema (31.5% and 16.0%, respectively, p < 0.05).
In patients with eczema (Table III), sexual difficulties were significantly associated with young age, high severity, itch, anxiety and depression. In patients with psoriasis, sexual impairment was associated with young age, itch, anxiety, and depression. In patients with acne, sexual impact was associated with sex (higher impact in men), flare on hands, and itch. As for blistering diseases, because of the small number of patients, significance was reached only for clinical severity. However, there was a strong association between sexual impact and young age.
Table III. Logistic regression models for eczema, psoriasis, acne, and blistering disorders, with sexual impact as the dependent variables. The odds ratios (OR) were also adjusted for region
It was not possible to test the model for hidradenitis suppurativa, due to the low number of patients, however a strong association, although not significant, was observed between sexual impact and young age, clinical severity, itch, and anxiety.
In this study, the impact of dermatological conditions on sexual life was investigated with simple standardized procedures in a large population of dermatological patients recruited in different European areas. The impact was particularly high in patients with hidradenitis suppurativa, prurigo, blistering disorders, psoriasis, urticaria, eczema, infections of the skin and pruritus. The important impact of hidradenitis suppurativa, which is a chronic, debilitating suppurative skin disease (11), on quality of life and on a wide spectrum of psychophysical aspects (including fatigue, depression, stigmatization level, and overall activity) has been documented (12, 13); however, to our knowledge, sexual impact had not been specifically evaluated.
Decreased sexual functioning has been reported in patients with psoriasis (4, 14). In both studies, sexual impact was evaluated using single questions. In the first study, 40.8% of patients were sexually affected based on the question “Do you believe that since the onset of psoriasis your sexual activity has declined?”. In the other study, sexual life was impaired in 35–71% of patients with psoriasis, depending on the different aspects covered by questions from different questionnaires. Another study (15) showed that psoriasis patients had more problems with orgasm than with desire, and stated that problems with orgasm might be due to disturbed self-esteem or emotional problems rather than severity or localization of the disease. One study (16) showed that psoriasis had a detrimental effect on quality of life and sexual health, in particular when the lesions were localized on the genital area, and in women more than in men. In the present study, sexual impact in patients with psoriasis was significantly associated with young age, itch, anxiety, and depression. The relevant role of itch was previously highlighted by Yosipovitch et al. (17) who reported that, as result of pruritus, sexual desire of 35% of study participants was decreased or non-existent.
The issue of sexual life was also examined from a qualitative point of view in patients with acne, psoriasis, and atopic eczema (18). These conditions had adverse effects on participants’ self-perceived sexual attractiveness and self-confidence, and in particular psoriasis and eczema also had marked effects on sexual well-being and on capacity for intimacy.
Several studies have addressed the sexual life of patients with atopic dermatitis. Misery et al. (5) showed that 57.5% of patients with atopic dermatitis noted decreased sexual desire, and 36.7% of their partners reported that the appearance of eczema had an impact on their sexual life. A German study showed that the exchange of tenderness in patients with atopic dermatitis and psoriasis was significantly reduced (19). Sexual life was studied in detail in Turkish patients with vitiligo and chronic urticaria (20), who reported experiencing significantly more difficulties in sexual arousal and in reaching orgasm than did controls. In a large French population aged from 15 to 24 years, the presence of acne was associated with less frequent sexual intercourse compared with the control group (21). Since adolescents are the main group with acne (22), and our population did not include patients under 18 years of age, the impact of acne in total is probably even greater than what we observed. Sexual life was more impaired in men with acne, probably because it is easier for women to hide the lesions using make-up.
A possible explanation for all these findings is not only that the condition may affect the genital area, and thus result in pain or discomfort, but also that the skin has an erotogenic function, and skin lesions can make physical contact difficult. Although this issue may be very burdensome for the individual, this problem is rarely addressed during routine dermatological consultations. In the study by Niemeier et al. (19), 93% of patients with psoriasis and 96% of the patients with atopic dermatitis indicated that their attending physician had never addressed that problem.
In this study, we observed that sexual impact was strongly associated with itch, depression, anxiety, and even suicidal ideation. The cross-sectional nature of the study does not allow the sorting out of the complex interrelationship between the onset of disease, itch, the presence of anxiety and/or depression, and the sexual problems. Therefore, while it is not possible to draw any conclusion on the direction of the association, it is important to be aware that sexual impairment is often a marker for depression or anxiety, and even suicidal ideation and vice versa. Also, the correlation between item 9 of the DLQI and the DLQI total score was high, indicating that an impairment in sexual life often corresponds with a general impairment in quality of life.
An important issue is that sexual problems particularly affect young patients. It was observed (23) that, for example, the impact of psoriasis on quality of life was particularly noticeable in younger patients, while the symptomatic component, due to comorbidities, was more impaired in older patients. Sexual life is an important component of well-being, in particular in young people, and it is thus particularly impaired when a skin condition is present.
A limitation of this study is the use of a single simple question, which is not specifically validated to assess the sexual impact of dermatological conditions, and therefore does not allow one to evaluate in detail which aspects of sexual life are impaired. However, the aim of this study was to highlight the problem in general, and further studies are necessary to elucidate the single specific factors (such as, for example, shame or anger, or body site of the lesions, such as genital localization of rash, pruritus, etc.) that may be associated with a greater impairment of the patients’ sexual life in the different skin conditions. Furthermore, other complex symptoms, such as pain and itch, may be adequately screened for by simple questions, identifying and quantifying the problems before detailed analysis.
Another limitation is that patients were not asked if they have or they would like to have an active sexual life. The possible answers to question 9 of the DLQI include both “not at all” and also “not relevant”. Both of these options score 0. It would have been of interest to have analysed the data set excluding those patients who answered “not relevant”, but the data collection process did not distinguish between these 2 groups.
The results of the study reinforce the idea that it is important to take into account specific psychosocial problems, such as sexual life, when assessing severity and treatment efficacy in dermatological conditions. Having this screening, sexual impairment question “hidden” in the DLQI may make it easier to bring up the subject and address these issues in the clinic. Clinicians should be especially aware of the ability of several dermatological conditions to profoundly affect patients’ sexual well-being, which in turn is often linked to a range of psychological comorbidities.
AYF is joint copyright owner of the DLQI: Cardiff University and AYF receive royalties from its use. The other authors declare no conflicts of interest. FS and DA were supported, in part, by the “Progetto Ricerca Corrente 2015” of the Italian Ministry of Health.


 Click to show fullsize
Click to show fullsize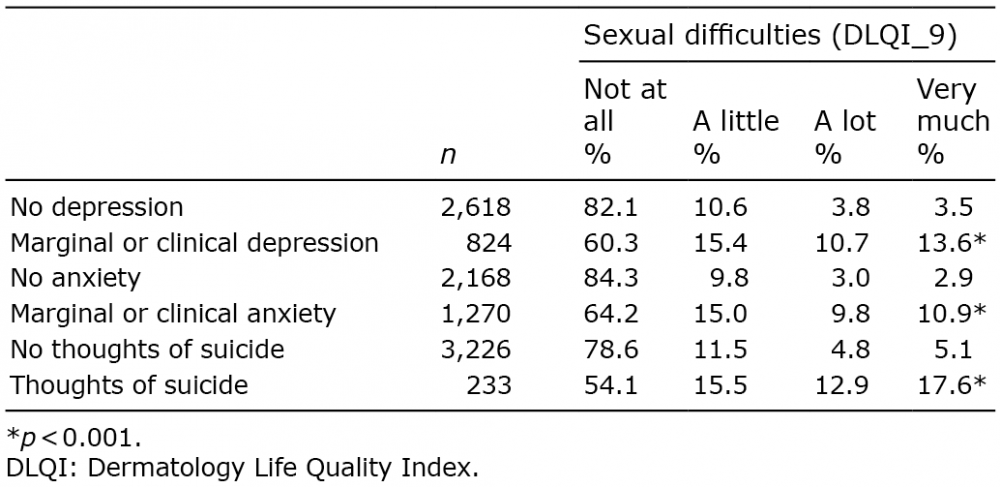 Click to show fullsize
Click to show fullsize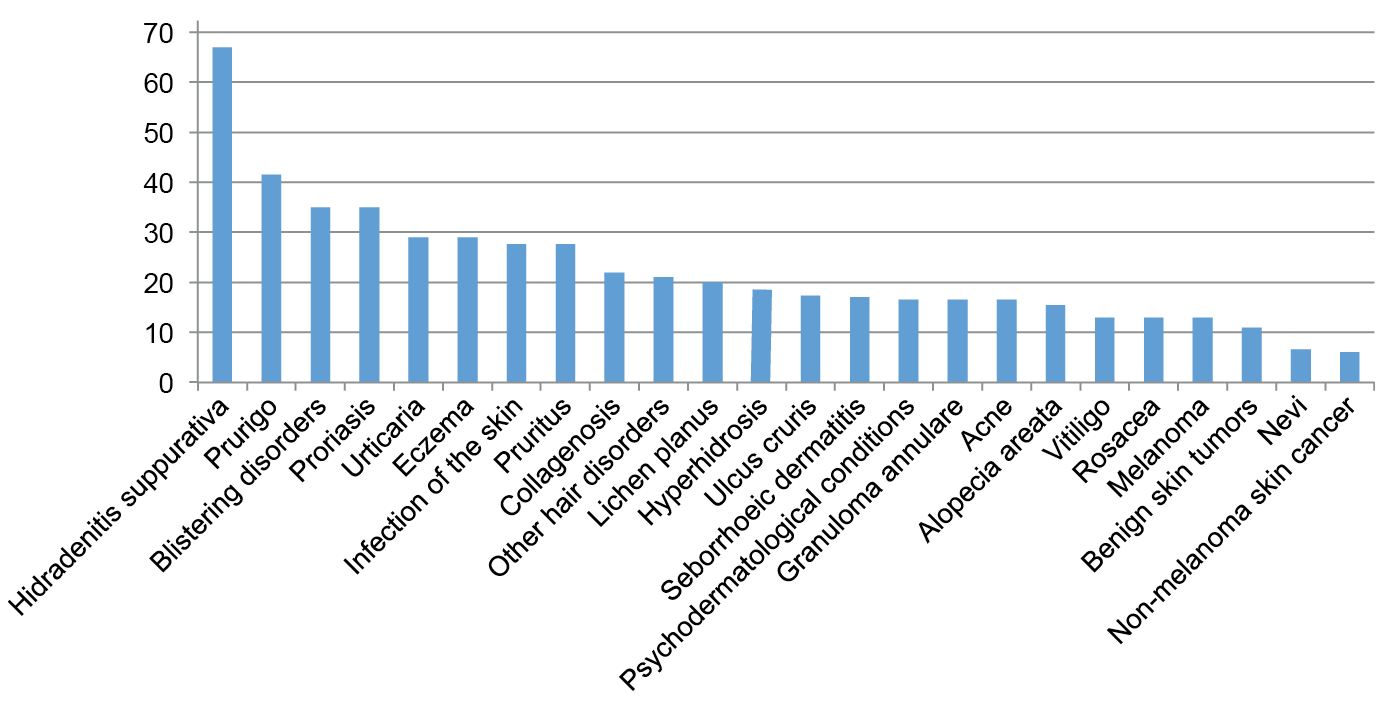 Click to show fullsize
Click to show fullsize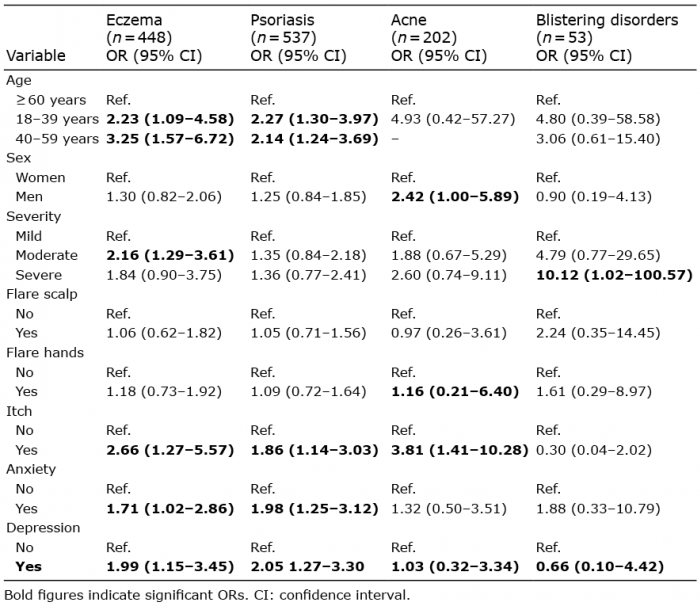 Click to show fullsize
Click to show fullsize