


1Faculty of Medicine, Section of Dermatology, University of Iceland, Reykjavik, Iceland, 2Department of Medical Sciences, Dermatology, Uppsala University, Uppsala, Sweden, 3Department of Immunology, 4Department of Anesthesiology and Critical Care, 5Department of Otolaryngology-Head and Neck Surgery, Landspitali – The National University Hospital of Iceland, Reykjavik, Iceland, and 6Department of Dermatology, University of Michigan Medical School, Ann Arbor, MI, USA
Psoriasis is a chronic inflammatory skin disease with profound effects on patients’ health-related quality of life (HRQoL). Twenty-nine patients with plaque psoriasis and a history of streptococcal-associated psoriasis exacerbations were randomly assigned to tonsillectomy (n = 15) or control (n = 14) groups and followed for 24 months. Patients were evaluated with the Psoriasis Disability Index, Psoriasis Life Stress Inventory and Psoriasis Area and Severity Index. HRQoL and psoriasis-related stress improved significantly in the tonsillectomy group compared with the control group (p = 0.037 and p = 0.002, respectively), with a mean 50% improvement in HRQoL and a mean 59% improvement in psoriasis-induced stress. Clinical improvement correlated significantly with improved HRQoL (r = 0.297, p = 0.008) and psoriasis-related stress (r = 0.310, p = 0.005). Of the tonsillectomized patients, 87% concluded that the procedure was worthwhile. Tonsillectomy may improve quality of life for selected patients with plaque psoriasis.
Key words: chronic plaque psoriasis; streptococcal throat infection; tonsillectomy; health-related quality of life; Psoriasis Disability Index; Psoriasis Life Stress Inventory.
Accepted Nov 2, 2016; Epub ahead of print xx
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Ragna Hlin Thorleifsdottir, Department of Medical Sciences, Dermatology, Uppsala University, Akademiska University Hospital, SE-751 85 Uppsala, Sweden. E-mail: ragnahlin@gmail.com
Psoriasis is a complex multifactorial disease caused by a combination of genetic and environmental factors (1), affecting approximately 2–3% of the world’s population (2). Psoriasis has a significant negative impact on many areas of health-related quality of life (HRQoL), including physical, occupational, social, psychological, and sexual wellbeing (3–5). Patients with psoriasis have reduced HRQoL, similar to that caused by major chronic illnesses such as cancer, myocardial infarction and diabetes mellitus (6). Many patients have low self-esteem and feel embarrassed, helpless, and stigmatized due to the visible nature of psoriasis (7, 8), which causes significant daily stress for patients (9). Clinical assessments, such as the Psoriasis Area and Severity Index (PASI) (10), do not adequately reflect the general impact that the disease has on the lives of patients with psoriasis, but instead give a static score of clinical disease severity (11).
Many environmental factors have been implicated in psoriasis; in particular, throat infection with β-haemolytic streptococci has been associated with both the initiation and exacerbation of psoriasis (12–15). T cells primed by streptococcal antigens in the tonsils may react with homologous antigens in the skin (16–18), and there are several reports of partial or complete remission of psoriasis after tonsillectomy (reviewed by (19–21)). We reported previously on a randomized controlled trial examining the clinical efficacy and immunological impact of tonsillectomy on plaque psoriasis. The results indicated that tonsillectomy can lead to a significant clinical improvement in plaque psoriasis, with a significant reduction in the frequency of skin-homing T cells that recognize homologous streptococcal M-protein and skin keratins (22). We report here findings related to patient HRQoL and psoriasis-induced stress and their association with clinical improvement after tonsillectomy.
Patient eligibility criteria have been detailed previously (22). Briefly, eligible patients were: ≥ 18 years of age; had moderate-to-severe chronic plaque psoriasis diagnosed by a dermatologist; had a history of sore throat-associated psoriasis exacerbation; and were willing to undergo tonsillectomy. Exclusion criteria were: underlying medical conditions, such as heart and lung diseases and bleeding disorders; alcohol or drug abuse; pregnancy; and previous tonsillectomy. Before study initiation patients were required to discontinue all psoriasis treatment except moisturizers within the previous 4 weeks.
Fifty-four patients were screened for the study, the majority of whom were referred by a dermatologist (44%) or responded to an advertisement (46%). A few patients had heard about the study by other means (6%) or were referred by an otolaryngologist (4%). Written informed consent was obtained from each patient before initiation of study participation. A total of 29 patients met the inclusion criteria.
This was a single-centre, 24-month, parallel, assessor-blind, randomized controlled trial. Data were collected within the departments of Dermatology and Otolaryngology-Head and Neck Surgery in Landspitali, The National University Hospital of Iceland, Reykjavik, Iceland, from November 2007 to January 2011. The study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments and approved by the National Bioethics Committee of Iceland (VSNb2006090015/03-15) and the Data Protection Authority of Iceland.
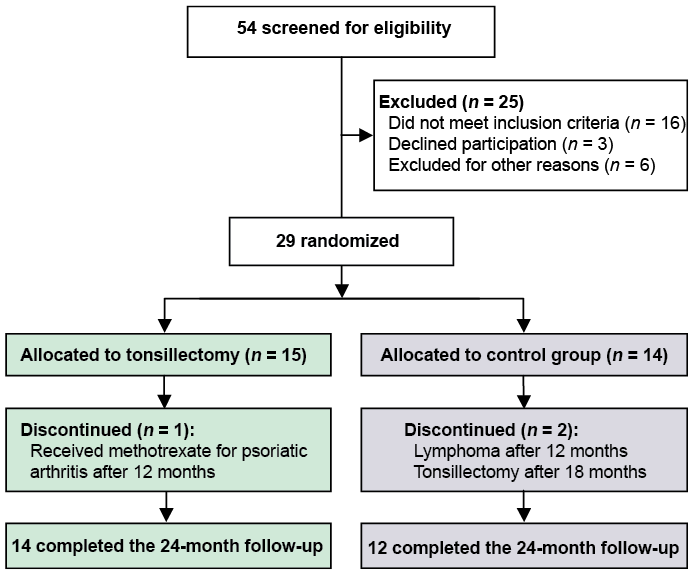
A sealed allocation sequence with a numerical code was created by the study supervisor before recruitment began, with a simple randomization in a 1:1 ratio. The 29 patients who met the inclusion criteria were allocated into tonsillectomy and control groups (Fig. 1). The allocation was concealed until the end of the study in order to reduce study bias. Recruitment and follow-up of all patients was performed by the same investigator throughout the study, who was unaware of the allocation system and thus the tonsil status of the patients. Detailed data were collected on patients’ demographics and psoriasis features. Patient-reported outcomes were measured at baseline and at months 12 and 24.
Fig. 1. CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Primary end-points were defined as clinically significant changes in HRQoL, assessed by the Psoriasis Disability Index (PDI) and Psoriasis Life Stress Inventory (PLSI) at 12 and 24 months. These parameters, along with secondary end-points, were compared with baseline scores and between the 2 groups. Secondary end-points included the correlations between the change in clinical disease severity (Psoriasis Area and Severity Index, PASI score) and HRQoL scores (PDI and PLSI) as well as evaluation of a study-specific questionnaire, applied at the end of the study.
HRQoL was assessed with a psoriasis-specific questionnaire, the Psoriasis Disability Index (PDI) (23). The PDI is a validated self-administered questionnaire covering aspects of functional disability owing to psoriasis in the preceding 4 weeks. The PDI addresses 15 issues that can group to 5 domains: daily activities, work/school, personal relationships, leisure, and treatment. The PDI score is rated on a 4-point scale, with grades from “not at all” to “very much” and the total score, ranging from 0 to 45, is calculated by summing the scores given to each question. The total score can therefore range from none to maximal impairment of quality of life.
Psoriasis-related stress was assessed with the Psoriasis Life Stress Inventory (PLSI) (24). The PLSI is a 15-item questionnaire that estimates psychosocial stress due to psoriasis. For each question the patients must rate the level of stress experienced over the previous 4 weeks on a 4-point scale, ranging from “not at all” to “very much.” The PLSI score, ranging from 0 to 45, is calculated by summing the scores for each question. Both the PDI and PLSI have been used in the English version for evaluation of psoriasis. The questions were translated into Icelandic using the translation-back-translation procedure and validated by the Nordic Quality of Life study (25). The patients completed both questionnaire at study entry and at 12 and 24 months.
After the 24-month study period, participants answered a study-specific questionnaire with the aim of rating the overall experience of having tonsillectomy as a treatment for psoriasis. The questionnaire was composed of 20 multiple-choice questions, rated on a scale ranging from “not at all” to “very much” and 3 short-answer questions. The questions addressed difficulties associated with the tonsillectomy, recovery time, complications, and whether the operation had been worthwhile. Also, questions about self-perceived improvement in psoriasis, psoriasis nails and/or psoriatic arthritis and regarding HRQoL and psoriasis stress. Moreover, participants were asked about the use of psoriasis treatments, such as moisturizers, topical treatments or systemic therapy, and if they had experienced sore throat or streptococcal throat infections with subsequent exacerbation of psoriasis after removal of their tonsils.
Clinical follow-up has been detailed previously (22). Briefly, clinical severity was assessed by PASI score (10) at study entry and at 2, 6, 12, 18 and 24 months. The use of psoriasis treatment agents during the follow-up period was monitored closely.
Patient demographics were summarized descriptively and data were tested for normality using the Kolmogorov-Smirnov test. PDI and PLSI scores at months 12 and 24 were compared between the groups and with baseline scores using analysis of variance (ANOVA) test for repeated measurements. Data for months 12 and 24 were analysed with the intent-to-treat method, where any missing data were replaced using the last observation carried forward (LOCF) method. Square root transformation of the results was used to better approximate normality in the ANOVA model. Statistical significance was defined by p < 0.05. Spearman’s rank correlation analysis was performed to evaluate the relationships between clinical improvement and improvement in HRQoL (PDI and PLSI scores) from baseline to month 24. Data analyses were performed using R software, version 2.10 (The R foundation, Austria).
Of the 54 patients with psoriasis who were screened, 38 met all the inclusion criteria. Six eligible patients were excluded due to chronic disease, ongoing systemic psoriasis treatment and pregnancy, and 3 declined to participate after screening. Thus, a total of 29 patients with plaque psoriasis and a history of psoriasis exacerbation during or after a sore throat were enrolled in the study (Fig. 1). Fourteen patients in the tonsillectomy group and 12 in the control group completed the 24-month follow-up, which took place from November 2008 to January 2011. One patient in the tonsillectomy group was started on methotrexate to treat his psoriatic arthritis after 12 months of participation. Two patients in the control group did not complete the study, one was diagnosed with lymphoma after 12 months, and the other violated the protocol by having tonsillectomy after 18 months of follow-up. There were no clinically meaningful differences between the groups and, although the tonsillectomy group had slightly higher baseline PASI, PDI and PLSI scores compared with the control group, these differences were not statistically significant (Table I).
Table I. Demographic data for the 29 participating patients with psoriasis
There was a significant improvement in HRQoL after tonsillectomy (Fig. 2A). The mean PDI score decreased significantly in the tonsillectomized group, both with time (p = 0.026) and compared with the controls (p = 0.037, 95% confidence interval (CI), 1.43–3.58). The patients’ quality of life improved in mean by 50%.
Fig. 2. Changes in health-related quality of life (HRQoL) and psoriasis-induced stress of the 29 participating psoriasis patients during the 24-month follow-up. Panel A: Tonsillectomized patients reported an improvement in HRQoL with a significant decrease in the mean Psoriasis Disability Index (PDI) score, both with time (p=0.026) and compared with the controls (p = 0.037, 95% confidence interval (CI) 1.43–3.58). No corresponding changes were observed for the control group. Panel B: Tonsillectomized patients reported less daily stress associated with their psoriasis, which was reflected in significantly decreased Psoriasis Life Stress Inventory (PLSI) score, both with time (p < 0.001) and compared with the controls (p = 0.002, 95% CI 1.39–3.10). The control group observed no corresponding changes. TX: tonsillectomy group. *Statistical significance.
The patients’ quality of life improved in mean by 50%. In accordance with a report (26), we divided the PDI data into 5 domains, to identify the areas that were most influenced by the tonsillectomy (Table II). There were significant changes in HRQoL associated with work and/or school after 12 and 24 months (p = 0.02 and p = 0.022, respectively) compared with the control group. The change in HRQoL associated with relationships was significant after 12 months (p = 0.04) and the change in HRQoL linked to the treatments was significant at 24 months (p = 0.04). No corresponding improvement in PDI scores (p = 0.803, 95% CI 3.38–4.23) or PDI domains was observed in the control group.
Table II. Mean changes in domains of the Psoriasis Disability Index (PDI) before and after tonsillectomy of the 29 participating patients with psoriasis
The tonsillectomized patients reported that their stress associated with having psoriasis decreased considerably after the tonsillectomy (Fig. 2B). Their PLSI score decreased significantly both with time (p < 0.001) and compared with the controls (p = 0.002, 95% CI 1.39–3.10), and improved, in mean by 59%. The control group did not exhibit any significant improvement in psychosocial stress related to coping with psoriasis (p = 0.654, 95% CI 2.67–3.56).
A significant positive correlation was observed between clinical improvement and increased HRQoL (r = 0.297, p = 0.008) (Fig. 3A). Likewise, there was a significant positive correlation between improvement in PASI score and improved psoriasis-related stress (r = 0.310, p = 0.005) (Fig. 3B).
Fig. 3. Correlation between clinical improvement, improved health-related quality of life (HRQoL) and psoriasis-related stress of the 15 tonsillectomized patients with psoriasis during the 24-month follow-up. Panel A: A significant positive correlation was noted between the change in clinical status (PASI score) and change in health-related quality of life (PDI score) (r = 0.297, p = 0.008). Panel B: Likewise, there was a significant positive correlation between the change in clinical status and the change in psoriasis-related stress (PLSI score) (r = 0.310, p = 0.005). Spearman’s rank correlation test. PASI: Psoriasis Area and Severity Index, PDI: Psoriasis Disability Index, PLSI: Psoriasis Life Stress Inventory.
At the end of the study, all the patients who had tonsillectomy answered a short, study-specific, questionnaire. Twelve (80%) patients felt that the surgery had been quite difficult and that the recovery took more time than they had expected. No major post-operative complications were reported, but one patient had minor bleeding the day after the procedure. Nevertheless, 13 (87%) of the patients thought that the surgery was worthwhile and 12 (80%) concluded that their psoriasis had improved markedly after the surgery. Two patients did not think that there was any clinical difference regarding psoriasis symptoms and one was unsure. When asked about the use of moisturizers, topical treatments and other psoriasis treatments during the 2 years after the tonsillectomy 12 (80%) patients reported less or fewer psoriasis treatments after the surgery. One out of 4 patients who had concomitant psoriasis arthritis reported an improvement in arthritis after the tonsillectomy.
We and others (22, 27, 28) have previously reported that tonsillectomy can have marked clinical benefits for selected patients with psoriasis. We now extend these findings to demonstrate that the improvement in clinical activity of psoriasis achieved through tonsillectomy, despite being an overall difficult procedure to go through, leads to a significant positive impact on the activities of daily life and psychosocial wellbeing of patients. Thus, the HRQoL improved by 50% and tonsillectomized patients reported almost 60% lower psoriasis-related stress after the surgery. Furthermore, we found that the increased HRQoL and improved psoriasis-related stress correlated positively with the observed clinical improvement, as assessed by PASI scores.
Patients with psoriasis have a 10-fold higher frequency of symptomatic streptococcal throat infections than matched household controls (14), and the asymptomatic carrier rate for group A, C and G Streptococci has been reported to be as high as 44% in patients with plaque psoriasis and a known history of psoriasis exacerbation associated with sore throat (29). Furthermore, up to 70% of Icelandic patients with plaque psoriasis report an exacerbation of psoriasis symptoms during streptococcal throat infections (30). Thus, the genetic background of patients with psoriasis appears to be permissive for both streptococcal carriage and symptomatic streptococcal throat infections, and the latter has long been associated with flares of guttate psoriasis (12, 15, 31) as well as worsening of chronic plaque psoriasis (13, 14). It would be of interest to measure antistreptolysin O (ASO) titres (32) in patients who have tonsillectomy and correlate titres with both clinical improvement and increased HRQoL. We have recently reported that patients who benefit most from tonsillectomy, both clinically and in terms of quality of life, significantly more often have psoriasis onset associated with a throat infection. Furthermore, these patients reported an increased frequency of streptococcal throat infections per lifetime and were carriers of both copies of HLA-Cw*0602 (33). The mechanism whereby HLA-Cw*0602 predisposes to psoriasis is currently unknown. Our data, and those of others (17, 34–37), are consistent with the hypothesis that autoantigens presented in the binding pockets of HLA-Cw*0602 on epidermal cells are recognized by CD8+ T lymphocytes infiltrating lesional epidermis (18).
Although not yet validated, our end-of-study questionnaire gave an insight to the experience of having tonsillectomy to treat plaque psoriasis. Despite the risk of having the surgery, risk of post-operative complications and prolonged recovery time, 87% of the patients thought that the procedure was worthwhile, and 80% reported a marked improvement, which is concordant with the recorded reduction in PASI scores, ranging from 30% to 90%, in 87% of patients (22). Furthermore, 80% of the patients reported that their need for psoriasis treatment in the form of moisturizers, topical treatments, ultraviolet light treatment or other treatments was noticeably less after the tonsillectomy. This is in accordance with our previous finding that patients with plaque psoriasis needed less symptomatic treatment after tonsillectomy compared with controls (22).
One out of the 4 patients with concomitant plaque psoriasis and psoriatic arthritis (PsA) reported at the end of the study that his arthritis had improved after the tonsillectomy. Interestingly, this patient was homozygous for HLA-Cw*0602, which is strongly associated with cutaneous psoriasis (38, 39), early onset psoriasis (40–42), and psoriasis exacerbations after streptococcal throat infection (43, 44). There are very few studies that have explored a possible link between PsA, the tonsils and streptococcal throat infections. DNA encoding the 16S ribosomal RNA gene of group A streptococci has been found in the blood and synovial fluid of patients with PsA (45), and synovial T cells from patients with PsA have been reported to respond to streptococcal superantigens, but not to conventional streptococcal antigens (46).
There is currently no cure for psoriasis, and available treatments only offer symptomatic relief, as psoriasis typically relapses when treatments are discontinued. Our results suggest that selected patients with plaque psoriasis and a history of sore throat-associated exacerbation could benefit from tonsillectomy, both with respect to clinical measures of disease severity (PASI) as well as improved quality of life and reduced disease-related stress. Although our patient cohort was followed for only 2 years, we have observed that the improvement remains at least 5 years post-tonsillectomy (unpublished data). We therefore conclude that tonsillectomy may be a significant addition to the current psoriasis treatment for a selected patient group, and offer a long-lasting improvement. However, more robust trials and long-term follow-up of tonsillectomized patients with plaque psoriasis are needed.
The authors are indebted to Dr Andrew Finlay for his permission to use the Psoriasis Disability Index questionnaire and the staff at Landspitali-The National University Hospital of Iceland dermatology outpatient centre, ENT department and Immunology department for their assistance during the study.
This study was supported in part by the Icelandic Research Fund and Landspitali University Hospital Research Fund. AJ is supported by NIH K01 AR064765, the National Psoriasis Foundation USA and the Babcock Memorial Trust. JEG is supported by NIH K08 AR060802, R01 AR069071, The A. Alfred Taubman Medical Research Institute as the Kenneth and Frances Eisenberg Emerging Scholar Award, and the Doris Duke Charitable Foundation Grant (#2013106). The funding institutions had no role in the study.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize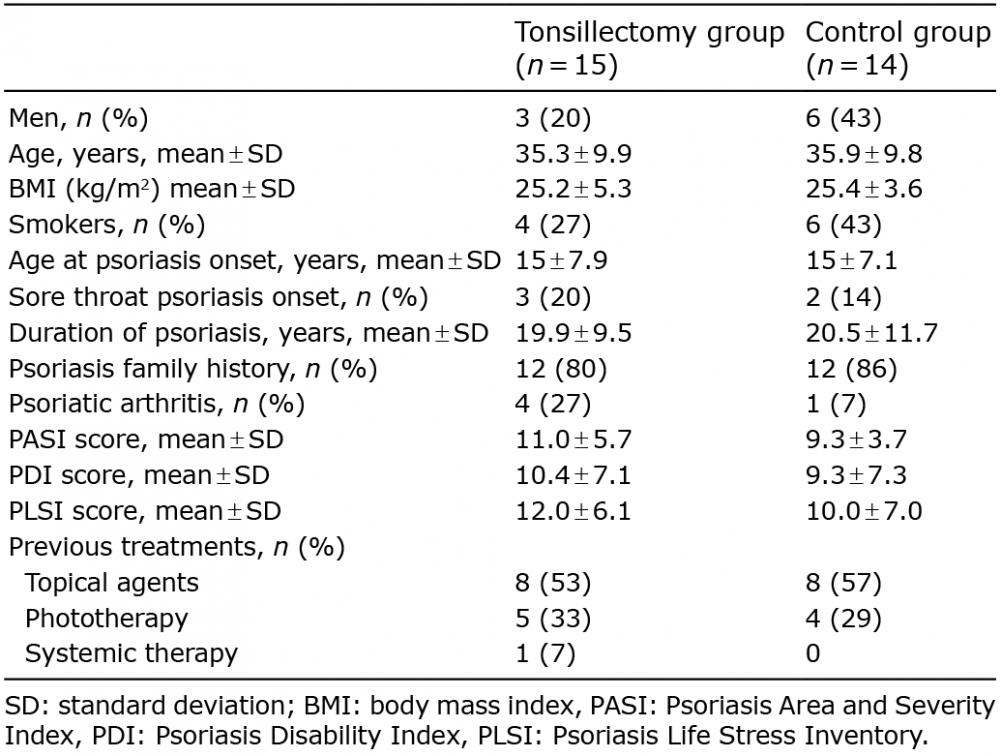 Click to show fullsize
Click to show fullsize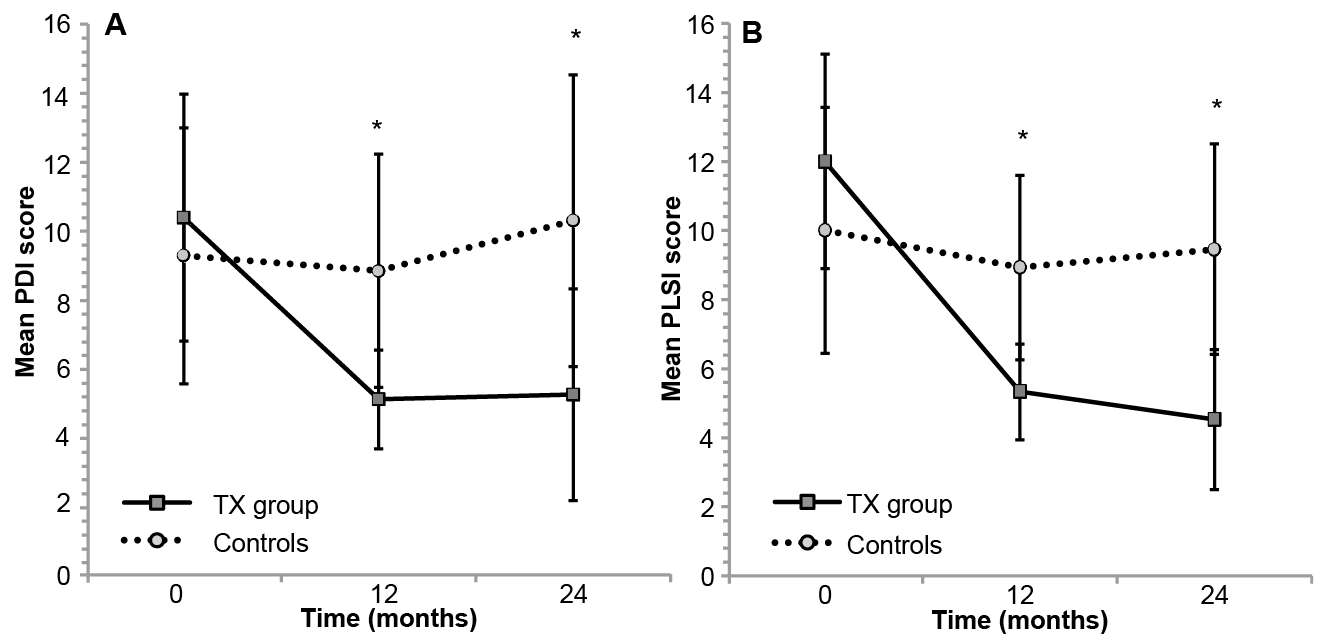 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize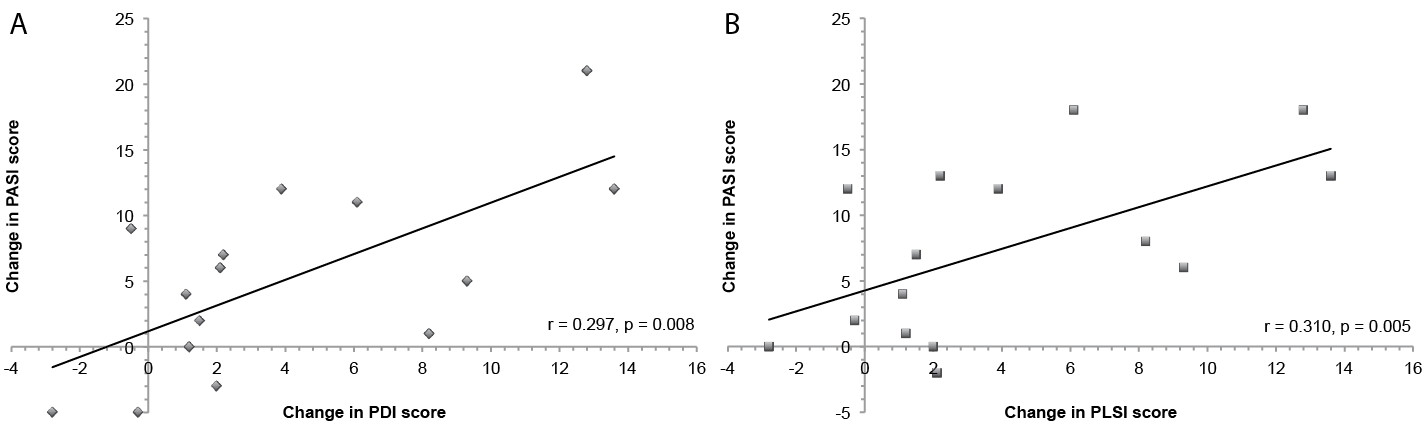 Click to show fullsize
Click to show fullsize