


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Lichen planus (LP) skin lesions are often accompanied by itch, but this symptom has not been thoroughly examined in LP. To better characterize itch in LP, 78 patients with LP were investigated. Itch was present in 94.9% of patients and was usually described as the most vexing symptom of LP. The mean ± SD severity of itch according to visual analogue scale score was 6.9 ± 2.8 points. Most patients experienced itching daily, pruritus episodes lasted longer than 1 min, and most often occurred in the evening. Itch was frequently described as burning and, for many patients, it was considered burdensome and annoying. The following factors most often increased the perceived severity of pruritus: sweating, high temperature, stress and hot water, while cold water and cold air often resulted in itch reduction. In conclusion, itch is the major subjective symptom of LP. Effective treatment of pruritus should be one of the main goals of LP therapy.
Key words: chronic dermatoses; pruritus; clinical characteristics.
Accepted Nov 8, 2016; Epub ahead of print Nov 9, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Adam Reich, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Ul. Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: adi_medicalis@go2.pl
Lichen planus (LP) is a chronic, papulo-squamous disorder of the skin, mucous membranes, nails and hair, with significant variability in its severity and evolution. LP is a rather uncommon condition, affecting approximately 0.5% of the general population in Europe, with a similar incidence in males and females (1). The typical clinical manifestations of LP on the skin include the presence of polygonal, flat-topped, violaceous papules and plaques with reticulated white lines, termed “Wickham’s striae”; however, a number of different clinical variants have also been described (2). LP lesions may appear as an isomorphic response to minor trauma (Koebner phenomenon). The disease most commonly affects the extremities, especially the flexures, such as the wrists and ankles. Involvement of mucous membranes is present in approximately 30–70% of patients with LP (2). Oral LP most commonly appears as asymptomatic or tender, white, reticulated patches or plaques (reticulated form), or as painful erosions and ulcers (erosive form). LP of the genitalia most commonly presents with pruritus or hyperalgesia, in particular in the erosive variant, and may lead to vaginal discharge or erosive forms of haemorrhage (2).
Itch is a cardinal subjective symptom of cutaneous lesions of LP. In our preliminary study we have shown that itch is the most unpleasant and bothersome symptom for the majority of patients with LP (3, 4). This is in accordance with other previously published studies, which have demonstrated that itch can greatly alter the well-being of patients with different conditions, and that subjects with chronic pruritus may have significantly impaired quality of life, and depression and anxiety (5–8). Despite its importance, clinical aspects of itch in LP have not been well characterized in the literature. The aim of this study is therefore to better describe the clinical manifestation of itch in LP, in order to increase understanding of this symptom, and help enable the development of effective antipruritic treatment strategies to improve medical care for such patients.
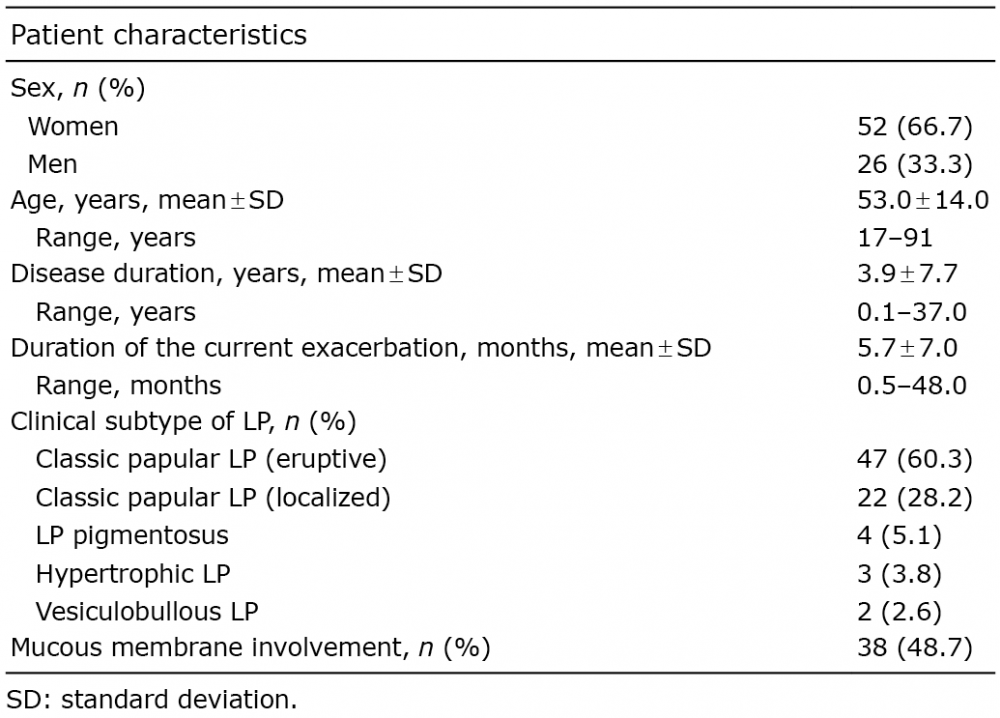
A total of 78 consecutive adult patients with LP, diagnosed based on typical clinical presentation and histology, and treated between 2012 and 2015 at the Department of Dermatology, Venereology and Allergology of the Wroclaw Medical University, Wroclaw, Poland were enrolled in the study. Patients with other dermatological conditions that could have influenced the results were not included. There were 52 (66.7%) females and 26 (33.3%) males (ratio 2:1), age range 17–91 years (mean age 53.0 ± 14.0 years). Detailed characteristics of included patients are shown in Table I; there were no patients with the predominant erosive variant in this series. Patients with LP received potent topical corticosteroids combined with phototherapy (narrow-band ultraviolet B (UVB) 311 nm or psoralen plus ultraviolet A (PUVA)) as first-line treatment, except for patients with vesiculobullous LP, who received only potent topical steroids.
Table I. Demographic and clinical characteristics of enrolled patients with lichen planus (LP)
The study was approved by the ethics committee of Wroclaw Medical University (decision 459/2012), and was conducted in accordance with the principles of the Declaration of Helsinki. All participants signed an informed consent form prior to any study procedure.
A specially designed structured questionnaire containing questions about demographic data (sex, age), duration of LP, clinical features of itch (e.g. frequency and diurnal/nocturnal variations of itch, presence of sleep disturbances, most common factors aggravating and alleviating itch) and administered therapy, were completed by the investigator, based on the patient’s history and physical examination.
Severity of itch was evaluated with 2 different methods: (i) a 10-cm visual analogue scale (VAS), on which patients indicated intensity of itch at the time of examination (VASexam) and at the time of maximal itch experienced in the previous week (VASmax) (9, 10); and (ii) the 12-item Itch Questionnaire with questions about itch severity, frequency, and localization, as well as disturbances in daily activities, sleeping and psychological well-being caused by itch (11). The scoring ranged from 0 (no itch) to 22 points (maximal itch).
The data were analysed using Statistica® 12.0 (Statsoft, Krakow, Poland). The χ2 test with Yates correction, Student t-test, Mann-Whitney U test, and Spearman’s rank correlation test were used where appropriate. p-values < 0.05 were considered statistically significant.
Itch was reported by most subjects: 74 (94.9%) patients experienced itch at some time during the course of LP, and 54 (69.2%) had pruritus during the examination. In addition, 54 (69.2%) patients claimed that they had pruritus during each outbreak of LP. Approximately one-third (n = 23) of individuals confirmed that they also experienced pruritus before onset of LP. The majority of the included patients considered pruritus the most bothersome symptom of LP (n = 51, 65.4%), followed by the fact of having skin lesions (45.4%). Only in a minority of patients were other symptoms indicated, such as burning sensation (1 patient), pain (1 patient) or difficulty eating (1 patient).
Among LP patients with itch, most experienced itch on a daily basis (n = 59, 79.7%); some (n = 11, 14.9%) experienced itch at least several times a week and only 4 (5.4%) had itch episodes less than once a week. Itch occurred most frequently in the evening (Fig. 1).
Fig. 1. Frequency of itch at various times of the day in patients with lichen planus.
Sixty subjects (81.1%) had itch limited to skin lesions, while the remaining 14 (18.9%) also experienced itch of uninvolved skin. Itch was observed on the lower extremities (n = 44, 59.5%), upper extremities (n = 42, 56.8%) and trunk (n = 34, 45.9%). Rarely, itch was observed on the face (n = 5, 6.8%), scalp (n = 3, 4.1%) or other specific locations (feet, n = 2; armpits, n = 2; nape, n = 1; skin folds, n = 1; buttocks, n = 1; ano-genital area, n = 1; oral cavity, n = 1). Generalized pruritus was found in 19 (25.7%) participants.
The intensity of itch at the time of examination (VASexam) ranged from 0 to 8 points (mean 2.8 ± 2.5 points) and at the time of maximal itch (VASmax) from 1 to 10 points (mean 6.9 ± 2.7 points). The maximal itch in LP was significantly more intense than the itch experienced after mosquito bite (mean 5.1 ± 2.4 points, range 1–10 points, p < 0.001). The itch scoring assessed with the 12-item Itch Questionnaire ranged from 1 to 19 points (mean 9.7 ± 4.1 points). The 12-item Itch Questionnaire scoring correlated primarily with VASmax (ρ = 0.52, p < 0.001) and, to lesser degree, with VASexam (ρ = 0.34, p < 0.01).
Itch was most intensive during the development of skin lesions in 37 (50.0%) patients, during the extension of skin involvement in 13 (17.6%), or when the disease was fully developed in 9 (12.2%) participants. In 12 (16.2%) patients the intensity of pruritus was independent of the disease phase, and the remaining 3 (4.1%) subjects were unable to define the moment of the most intense itch during the disease course.
Itch episodes usually lasted longer than 10 min (n = 29, 39.2%) or at least between 1 and 10 min (n = 28, 37.8%). In only approximately one-quarter of patients (n = 17, 23.0%) did itch episodes last < 1 min.
Regarding the terms used by the patients to described the feelings related to itch, it was frequently described as a burning sensation (n = 35, 47.2%), and less frequently as tickling (n = 12, 16.2%), skin warming (n = 7, 9.5%), stinging (n = 6, 8.1%), tingling (n = 5, 6.8%) or pricking (n = 5, 6.8%). Furthermore, it was often considered as burdensome (n = 42, 56.8%) and annoying (n = 39, 52.7%); for some subjects it was also distressing (n = 17, 23.0%) and unbearable (n = 10, 13.5%). Because of itch 23 (31.1%) participants admitted that they had decreased mood and 10 (13.5) felt anxious, while 20 (27.0%) became more nervous. In addition, 17 (23.0%) patients had problems with concentration due to itch.
Regarding sleep quality, 22 (29.7%) patients with LP declared that they almost always had problems falling asleep because of pruritus, and a further 19 (25.7%) had such problems at least occasionally. In addition, 23 (31.1%) participants reported that they frequently experienced awakenings during night-time sleep and 20 (27.0%) awoke in the night from time to time. Sleeping medications were taken frequently by 5 (6.8%) and occasionally by 8 (10.8%) patients with LP.
Various factors influencing itch have been mentioned in Fig. 2. Major factors exacerbating itching were: sweating (52.7%), warmth (51.3%), stress (43.2%), and hot water (41.9%), while factors commonly stated to reduce itch were cold water (32.9%) and cold air (25.7%). Patients have also used different household remedies to reduce itch; most often they applied creams or ointments (n = 27), took antihistamines (n = 6), applied alcohol or vinegar (n = 4), topical steroids (n = 3), scratched the skin (n = 3) or used other unique modalities (n = 8). Significant improvement in itch was observed shortly after initiation of treatment with potent topical corticosteroids and phototherapy in 12 (16.2%) patients, after a couple of days or weeks after beginning of treatment in 34 (45.9%) participants, or after complete resolution of skin lesions in 5 (6.8%) patients. Seven (9.5%) individuals reported that treatment of LP did not significantly improve their itch, and 16 (21.6%) had no opinion about the influence of LP treatment on itch. Regarding antihistamines, 9 (12.2%) patients claimed that they completely alleviated itch and a further 14 (18.9%) observed marked reduction in itch after their use. A small effect of antihistamines was observed by 12 (16.2%) participants, while 15 (20.3%) found them absolutely not effective. The remaining 24 (32.4%) subjects with LP did not use antihistamines to reduce itch and had no opinion about them.
Fig. 2. Influence of various factors on the intensity of itch in lichen planus.
No significant association was found between itch intensity or other clinical aspects of pruritus in LP, such as localization of itch, frequency and duration of itch episodes, and age, sex, included clinical subtypes of LP, duration of the disease, duration of the current exacerbation or involvement of mucous membranes (data not shown). However, patients who indicated pruritus as the most disturbing symptom of LP scored significantly higher on pruritus-measuring tools than the remainder of the patients with LP (mean ± SD VASexam: 3.3 ± 2.5 vs. 1.6 ± 2.0 points, p < 0.01; VASmax: 7.7 ± 2.1 vs. 5.4 ± 3.1 points, p < 0.001, 12-item Itch Questionnaire: 10.7 ± 4.1 vs. 7.8 ± 3.4 points, p < 0.01).
Itch is an essential symptom of LP. For the first time we have characterized in depth its clinical manifestation. A number of previous studies have demonstrated that itch is a frequent phenomenon in many other dermatological disorders, e.g. eczema, psoriasis, dermatomyositis, and cutaneous lymphomas (7, 12–15). Based on our results we conclude that itch is a frequent phenomenon in patients with LP and only a small portion of patients with LP does not experience itch. It seems that the prevalence of itch in LP is close to that in atopic dermatitis and more frequent than in, for example, psoriasis (7, 16). Although the comparison of the intensity of itch in different dermatoses is difficult, as no direct comparisons have been performed so far, it seems that pruritus in LP is less severe than in atopic dermatitis, because the maximal VAS in LP was approximately 7 points, while in atopic dermatitis it is stated to be approximately 8 points, but more severe than in psoriasis; usually the mean VAS in psoriasis is between 5 and 6 points (7, 12, 16). Itch in psoriasis is reported to cause significant impairment of quality of life, being one of the most relevant factors influencing the patient’s well-being (7, 8), and it seems very probable that at least similar impairment may be observed in patients with itch in LP. Itch in LP is also important because of the risk of koebnerization. As itch induces a desire to scratch, many LP patients with itch will scratch, causing minor trauma to the skin. Because of the Koebner phenomenon observed in this disease, new LP lesions may develop within such scratch marks, which may result in chronicity of the disease. Based on our previous study results itch in LP seems to respond better to treatment of LP, e.g. phototherapy and topical steroids, than itch in psoriasis may respond to treatment for psoriasis, because itch in most patients with LP subsided shortly after anti-LP treatment initiation, while in psoriasis itching alleviation was usually only observed after complete resolution of skin lesions (3). According to our own experience we suggest that phototherapy with topical corticosteroids is a good first-line treatment in many patients with LP, not only to improve skin lesions, but also to reduce itch. If this treatment combination is not helpful, one may consider a short course of cyclosporin A as an alternative, especially in patients with the most extensive lesions. The role of antihistamines in itch reduction in LP remains controversial; however, based on our results, we consider that they may be of some help in some individuals at least.
There are differences in the localization of itch between various dermatoses. In the current study the majority of patients with LP experienced itch limited to lesional skin. In contrast, Yosipovitch et al. (12) demonstrated that itch in psoriasis may also affect unchanged skin; an observation that may, to some extent, explain the phenomenon of koebnerization. Patients with LP reported slightly more itch on the lower and upper extremities, while psoriatic patients described more itch on the lower extremities and the trunk (12). Generalized itch was noted in LP and psoriasis with similar frequency (12, 17). Concerning effectiveness of therapy, itch in LP most frequently subsided shortly after anti-LP treatment initiation (62.3%), whereas in psoriasis it usually disappears only when all skin lesions are resolved (3). Regarding itch quality, itch in LP, similarly to that in patients with AD, was frequently described as a burning sensation (3). However, itch in patients with AD was also linked with pain (59%) (14).
Different factors can be inducers of itch, such as high temperature, low humidity, bathing, sweating activities and clothing, and psychological maters, such as stress, or fatigue due to sleep loss, which is sometimes even caused by itch itself. Among these, heat or warmth seems to be the major factor that provokes the itch response (18). Recent studies have identified a relationship between heat/warmth sensations and itch. As described by Murota & Katayama (19) heat stimulated itch in AD by the activation of transient receptor potential cation channel subfamily vanilloid type 1 (TRPV1), the calcitonin gene-related peptide, the vesicular glutamate transporter 2, and accumulation of artemin. Whether these receptors are engaged in the pathogenesis of itch in LP needs to be investigated.
In conclusion, this paper sets out a comprehensive clinical picture of itch in LP. Owing to its long duration, frequency and high intensity, itch in LP is a very bothersome symptom with great potential to impair quality of life of patients. Better understanding of this symptom and its features will help enable the provision of effective treatment.
This work is supported by a statutory research grant Pbmn 126 and National Science Centre grant 2012/05/N/NZ5/00882.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize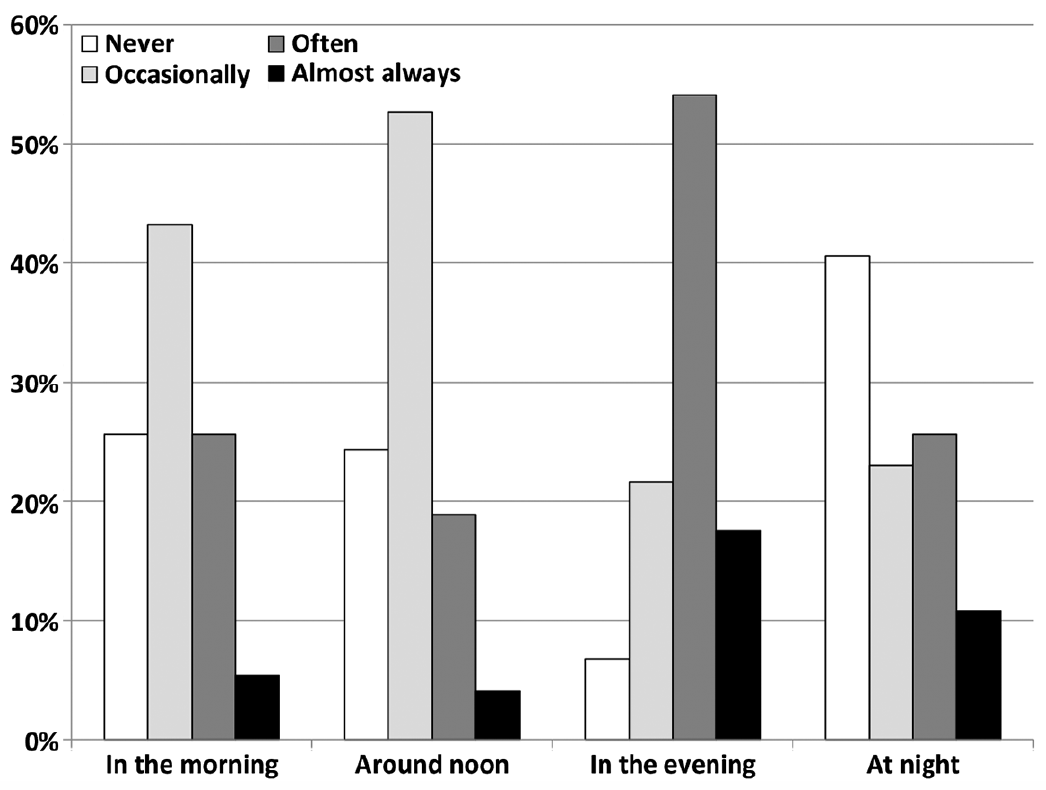 Click to show fullsize
Click to show fullsize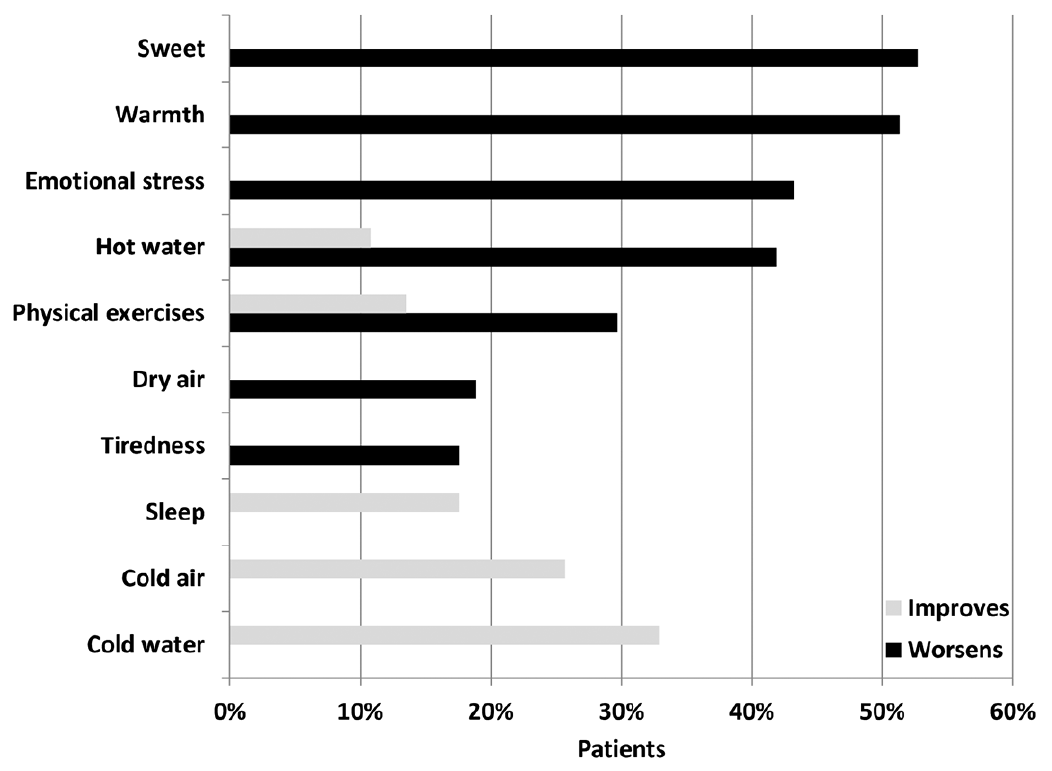 Click to show fullsize
Click to show fullsize