


Departments of 1Dermatology, Venereology, and Allergology and 2Internal Medicine II, University Hospital Würzburg, Josef-Schneider-Straße 2, DE-97080 Würzburg, 3Institute of Pathology and Comprehensive Cancer Center Mainfranken, University of Würzburg, Würzburg, Germany. E-mail: Toksoy_a@ukw.de
Accepted Nov 8, 2016; Epub ahead of print Nov 9, 2016
Worldwide, more than 95% of adults over the age of 40 years are seropositive for Epstein-Barr virus (EBV). Most EBV infections are asymptomatic and occur during childhood. An acute EBV infection in adolescence presents as infectious mononucleosis and usually heals without sequelae. However, some EBV-infected individuals develop chronic active EBV infection (CAEBV) resulting from continuous latent infection of T cells, NK cells, B cells, or epithelial cells (1–3). In particular, immunodeficient and Asian patients carry an increased risk of CAEBV. The clinical presentation of CAEBV is variable, and is characterized by fever, hepatic dysfunction, splenomegaly, lymphadenopathy and thrombocytopaenia. In addition, some of these patients show hydroa vacciniforme-like skin eruptions with oedematous swelling of the face and eyelids (4–10). CAEBV is a disease with potentially life-threatening complications, such as EBV-associated lymphomas, which are associated with a high morbidity and mortality (3, 5). We report here such a case.
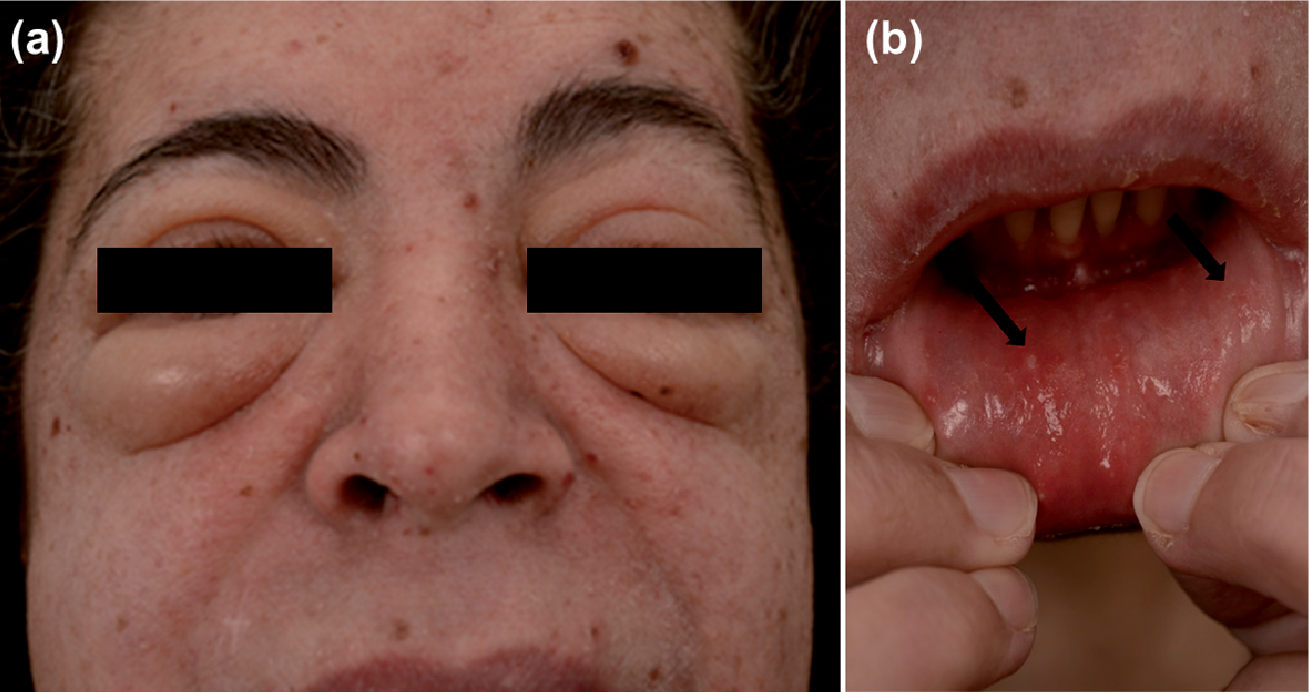
A 45-year-old Turkish woman presented with persistent swelling of the face, erosive facial papules and small oral ulcers that had developed 5 years previously (Fig. 1). As granulomatous cheilitis and Morbihan disease/oedematous rosacea had been suspected prior to first presentation at our department, the patient had been treated with several, mainly immunomodulating, therapies, including systemic corticosteroids, dapsone, methotrexate, fumarates and the tumour necrosis factor (TNF) antagonist adalimumab, without success. The clinical course was complicated by the development of diplopia and excessive B-symptoms (weight loss, night sweats and a reduced condition). Computed tomography (CT) scans revealed splenomegaly, cervical and mediastinal lymphadenopathy, hilar and para-aortal consolidations and oedematous ocular muscles.
Fig. 1. Clinical features. (a) Oedematous swelling of the eyelids and the lips. Disseminated crusty papules of the facial skin. (b) Intraoral aphthous ulcers (arrows).
Histological examination of biopsies obtained from the upper lip mucosa and facial skin showed a variable dense lymphoid infiltration. EBV+ T cells were identified within the infiltrate by EBV RNA in situ hybridization in conjunction with conventional immunohistochemical, as well as double and triple immunofluorescence staining. These EBV+ T cells were mostly CD4+ (Fig. S1a–c), although, in addition, a population of CD8+ EBV-infected T cells, and few CD79a+ B cells, could be detected (Fig. S1d). Molecular clonality analyses were consistent with oligoclonal EBV+ T-cell proliferation (Fig. S2). Subsequent lymph node and bone marrow biopsies revealed the same oligoclonal EBV+ T-cell proliferation. Blood analysis revealed increased levels of EBV DNA (6,000 copies/ml) and the presence of immunoglobulin G (IgG) antibodies against EBV antigens (EBNA-1, VCA p18, VCA p23, BZLF1, EA p138, EA p54). CAEBV infection associated with T-cell lymphoproliferation in multiple organ systems was diagnosed.
With respect to the known high risk for progression into an aggressive EBV-associated lymphoma, treatment with 2 cycles of CHOP (cyclophosphamide (375 mg/m2), doxorubicin (50 mg/m2), vincristine (2 mg), prednisone (100 mg) for 5 days) were given every 3 weeks; however, there was no clinical response and a considerable EBV load persisted in the blood (3,000 copies/ml). Therefore, the anti-CD20 antibody rituximab (375 mg/m2) was added to the protocol (R-CHOP) for a total of 4 cycles, with the aim of also specifically targeting the B-lymphocyte compartment. The patient responded to this approach (reduction in B symptoms, improvement in intraoral aphthous lesions, regression of lymphadenopathy and splenomegaly). However, the EBV load of 6,000 copies/ml only partially improved to a viral load of 1,000 copies/ml, while the hydroa vacciniforme-like skin lesions further progressed (not shown).
Seven months after the primary diagnosis of CAEBV and more than 4 years after the onset of first cutaneous indicator lesions, a follow-up CT scan revealed newly developed hepatic infiltration. A liver biopsy showed a dense infiltrate of atypical CD56–/CD3–/CD8+ and EBV+ highly proliferative cells, classified as extranodal EBV-associated NK/T-cell lymphoma (Fig. S1).
Normal distribution of NK-/T and B cells without detection of an NK/T-cell lymphoma could be observed in repetitive flow cytometric analyses of the peripheral blood and the bone marrow. Hence, an intensified chemotherapy protocol (SMILE) was initiated comprising high-dose methotrexate (2,000 mg/m2), etoposide (100 mg/m2), ifosfamide (1,500 mg/m2) and PEG-asparaginase (2,000 IE/m2). After re-induction of a partial response, the patient finally underwent reduced-intensity conditioning with fludarabine and busulfan, followed by human leukocyte antigen-matched allogeneic stem cell transplantation from a sibling donor. Day +100 staging revealed complete remission. The patient later developed limited chronic graft-versus-host disease, requiring topical and systemic immunosuppressive treatment that resolved completely. At time of writing, 18 months after transplantation, the patient is alive in complete remission and free of immunosuppressive drugs. The cutaneous manifestations, including the hydroa vacciniforme-like lesions, have resolved completely.
The diagnosis of CAEBV is often delayed for many years, as was the case in our patient, because the skin changes are non-specific and often misinterpreted as an inflammatory skin disease, such as rosacea or granulomatous cheilitis, sarcoidosis, dermatomyositis and lupus erythematosus profundus (11, 12).
Patients with EBV+ lymphoproliferative infection can be classified into 2 subgroups of T-cell and NK-cell CAEBV, depending on which cell type is predominantly infected. The subgroups present with different clinical features and prognoses. CAEBV of the T-cell type is characterized by frequent episodes of high fever and high titres of anti-viral capsid antigens (VCA) IgG and anti-early antigens (EA) IgG, whereas hypersensitivity to mosquito bites, large granular lymphocytosis, and high IgE titres are typical of the NK-cell type (11). In 12% of patients with a CAEBV+ NK/T-cell lymphoproliferative disorder, a transition into an EBV+ highly aggressive lymphoma occurs (11). Extranodal NK/T-cell lymphoma is a rare entity with a heterogeneous clinical presentation. Most of these cases are characterized by an angiocentric and angiodestructive infiltrate of EBV+ cells with an NK-cell phenotype (5, 13).
Risk factors associated with higher mortality of CAEBV represent higher age of onset (> 8 years), sex (female), splenomegaly, anaemia, thrombocytopaenia, liver dysfunction (11) and high EBV-DNA plasma concentrations (> 600 copies/ml). Our patient fulfilled the risk factors of higher age of onset, splenomegaly, high EBV-DNA plasma concentration (6,000 copies/ml) and anaemia. Hence, an upfront chemotherapy was applied, which, however, achieved only partial remission with CHOP/R-CHOP.
Nevertheless, 7 months after the primary diagnosis of CAEBV and more than 4 years after the onset of cutaneous indicator lesions our patient developed an extranodal NK/T-cell lymphoma of the liver. Therapy of NK/T-cell lymphoma is difficult and specific guidelines are lacking. Therefore, therapy is usually conducted according to treatment regimens for aggressive non-Hodgkin’s lymphomas, which include anthracycline-based (e.g. CHOP) or L-asparaginase-including protocols (e.g. SMILE). Patients with relapsed or refractory disease show a median survival of approximately 4 months with anthracycline-based chemotherapy (14). L-asparaginase-including regimens show promising outcomes in a recent study with a complete, partial, and overall response rate of 55.6%, 26.7%, and 82.2%, respectively, achieving 5-year overall survival rates of 66.9% (15).
Primary refractory cases or relapses after autologous stem cell transplantation should proceed to reduced-intensity allogeneic stem cell transplantation, preferably after re-induction of remission (16).
After diagnosis of an extranodal NK/T-cell lymphoma of the liver a consolidation therapy with SMILE was administered in our patient, followed by allogeneic stem cell transplantation. The patient has since been in complete remission; currently a period of 18 months.
KB-B received educational/travel grants and honoraria from TEVA GmbH, Roche Pharma and Bristol-Myers Squibb, MG is advisory board member of Janssen Cilag, and MW has educational grants from TEVA GmbH.


 Click to show fullsize
Click to show fullsize