


1Department of Psychiatry, and 2Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Trichotillomania is an impulse control disorder characterized by repetitive pulling out of one’s hair. The aim of this study was to estimate the prevalence of trichotillomania in young adults and its association with anxiety and obsessive-compulsive disorders (OCD). A total of 339 individuals completed a questionnaire to determine the presence of trichotillomania. OCD and anxiety disorders were diagnosed according to the diagnostic criteria of the International Classification of Diseases 10th Revision (ICD-10), based on the Composite International Diagnostic Interview. Twelve persons (3.5%) reported hair pulling during their lifetime, but only 8 of them met the criteria of trichotillomania according to the ICD-10. Four individuals had stopped their behaviour prior to the study participation. The lifetime anxiety disorders were diagnosed in 5 participants with trichotillomania (62.5%), while in the group
without trichotillomania, 67 persons (20.2%) met the diagnostic criteria for anxiety disorders (p < 0.01). OCD were not diagnosed in individuals with trichotillomania, among participants without trichotillomania, 14 persons (4.2%) reported symptoms of OCD.
Key words: trichotillomania; hair pulling; CIDI.
Accepted Nov 8, 2016; Epub ahead of print Nov 9, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Ul. Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive pulling out of one’s hair, usually from the scalp and/or eyebrows, eyelashes or elsewhere, that results in noticeable hair loss (1). TTM is more commonly observed in younger patients; the mean age of onset is 12 years. It can, however, begin at any age (2, 3). Many authors suggest that TTM in children, especially at pre-school age, is relatively benign and self-limiting (4, 5) and may be seen as analogous to nail-biting or thumb-sucking; however, less is known about the clinical relevance of TTM in older patients.
The prevalence of TTM has not been studied in systematic epidemiological surveys. In the past, TTM was considered as a relatively rare disorder with the prevalence assessed as low as 0.05% (6). More recent research indicates that TTM is much more common. A survey among 2,534 students found a 0.6% lifetime prevalence of TTM for both male and female respondents. Hair pulling resulting in visible hair loss, but failing to meet diagnostic criteria, was identified in 1.5% of males and 3.4% of females (7). King et al. (8) assessed hair pulling and associated psychopathology in a group of 794 adolescents. They reported a lifetime prevalence of hair pulling of 1% (n = 8; 5 males, 3 females) and a point prevalence of hair pulling of 0.5% (n = 4). In 3 out of 4 current hair pullers, obsessive-compulsive symptoms were described, i.e. a significantly higher rate compared with the general population. Two subjects with obsessive-compulsive disorder (OCD) also had generalized anxiety disorder (8). In a group of 210 children with hair loss and scalp disorders from dermatology clinics, TTM was diagnosed in 15 cases (7.1%). The mean age of presentation was 10 years, with female predominance (10 females). In addition to the scalp, 3 cases had eyebrows involvement (9).
The prevalence of non-clinical hair pulling behaviour appears to be higher; up to 11.0% or even 15.3%, in university surveys (10, 11). These studies indicate that hair pulling is quite common. TTM is more frequently diagnosed in women. A female:male ratio varied in different epidemiological studies from as much as 2:1 to 7:1 (8, 12–14).
Psychiatric comorbidity in TTM appears to be common, with anxiety disorders, mood disorders, substance use disorders, eating disorders and personality disorders being the most common associated conditions in adults (15, 16). Anxiety disorders are observed in youths (7, 16). Some data also support a relationship between OCD and TTM. A higher frequency of OCD in patients with TTM has been reported (8, 17), as well as higher rates of hair pulling in patients with OCD (18, 19). As TTM is characterized by repetitive behaviours limited to hair pulling, it is considered as an OCD spectrum disorder. According to this approach, TTM was moved from the group of “impulse control disorders not elsewhere classified” in the previous version of the American Psychiatric Association Classification DSM-IV to the group of disorders of obsessive compulsive spectrum in recent DSM-V (20), although in International Classification of Diseases 10th Revision (ICD-10) classification it still belongs to an impulse control disorders (21).
The aim of the study was to assess the prevalence of TTM among young adults and its association with anxiety and OCD. The study was approved by the ethics committee of Wroclaw Medical University, Poland.
A total of 343 medical students of Wroclaw Medical University were initially recruited in the study. Four of them (1.2%) declined to take part. A total of 339 students participated in the study: 208 females (61.4%) and 131 males (38.6%). The mean age was 23.7 ± 1.4 years, ranging from 22 to 26 years. Written informed consent was obtained from all participants after providing full information about the study.
All participants completed the questionnaire to determine the lifetime prevalence of trichotillomania. According to the purpose of the study, the questionnaire included questions about demographic data, age at onset of TTM and data on recent hair pulling occurrence, localization, frequency and intensity of hair pulling, and on feelings accompanying the act of hair pulling. Participants were asked how often they had experienced pleasure or relief after hair pulling, specifically with tension before or when trying to resist hair pulling. They were also asked about occurrence of hair eating, whether hair pulling was intentional or automatic, and whether it occurred during other activities. In addition, all individuals completed the questionnaire that determined the presence of onychophagia and onychotillomania (the data presenting findings on onychophagia and onychotillomania were published elsewhere (22)). OCD and anxiety disorders were diagnosed according to the ICD-10 diagnostic criteria (20). Each participant was examined by 1 of 2 psychiatrists (M.G. or P.P.) using the computerized Munich version of the Composite International Diagnostic Interview (CIDI). The CIDI is a highly structuralized diagnostic instrument developed by the World Health Organization (WHO) for epidemiological research purposes (23). The CIDI is considered a diagnostic instrument with confirmed reliability and validity, which allows diagnosis of lifetime and current mental disorders according to the ICD-10 classification. The CIDI is a highly structuralized diagnostic instrument for diagnosis of mental disorders systems. It is used to assess the prevalence of mental disorders not only in the general population, but also among individuals with different medical conditions. The CIDI has a modular structure and consists of 16 modules that can be used separately, depending on the aim of the study. Moreover, the CIDI allows us to distinguish between the psychopathological symptoms of mental disorders and symptoms that are related to medical condition, pharmacological treatment or alcohol and other psychoactive substance use (24–26). Using selected modules in our study the interview took approximately 15–45 min, depending on the psychopathological symptoms reported by the participant.
All results were analysed using the software package Statistica® 12.0 (Statsoft, Warsaw, Poland). The significance of the observed differences was determined by the Pearson’s χ2 test and 2-sided Fisher’s exact test. A p-value < 0.05 was considered statistically significant.
Twelve persons (3.5%) reported hair pulling during their lifetime, 9 females (75.0%) and 3 males (25.0%). Four of them, who did not meet the diagnostic criteria of TTM, reported the following behaviours: playing with eyebrows that led to hair loss of brows, hair pulling from legs using tweezers, pulling artificial eyelashes, single incident of scalp hair pulling after a family quarrel. Eight participants (2.4%) fulfilled the diagnostic criteria of TTM (6 females and 2 males). The characteristics of participants with TTM are shown in Table I. The mean age of TTM onset was 16.9 ± 4.6 years, ranging from 11 to 24 years. Half of the individuals pulled hair from the scalp (n = 4; 50.0%), 3 (37.5%) pulled their eyebrows, 2 (25.0%) pulled the eyelashes and 1 (12.5%) pulled hair from the abdominal area. Two of them described 2 localizations of hair pulling: 1 on the scalp and eyelashes and 1 on the scalp and eyebrows. Four individuals (50.0% of group with TTM) who reported hair pulling during their lifetime had stopped their behaviour prior to study participation. The mean duration of TTM was 4.5 ± 4.2 years, ranging from 1 to 11 years. Three participants (37.5%) with lifetime TTM also reported symptoms of onychophagia and 2 persons (25.0%) reported symptoms of onychotillomania. The prevalence of onychophagia and onychotillomania in subjects without TTM was 47.3% (p = 0.73) and 0.3% (p = 0.001), respectively. Lifetime anxiety disorders were diagnosed in 5 participants with TTM (62.5%), while in the group without TTM 67 persons (20.2%) met ICD-10 criteria for anxiety disorders during lifetime. The difference in the lifetime prevalence of anxiety disorders between individuals with TTM and without TTM was statistically significant (exact Fisher’s test: p = 0.029). Individuals with TTM did not meet the diagnostic criteria for OCD. In the group without TTM OCD was diagnosed in 14 persons (4.26%). Due to the small size of the TTM group the difference in OCD prevalence could have arisen by chance alone.
Table I. Characteristics of individuals with trichotillomania
Current TTM was diagnosed in 4 individuals (1.2%): 2 females and 2 males. In this group, anxiety disorders were diagnosed in both women (1 with specific phobia; 1 with panic disorder). Males did not meet any criteria of anxiety disorders. OCD was not diagnosed in this group.
All participants with current TTM (n = 4) reported their hair pulling to be, least part of the time, an automatic behaviour. Two of them had always pulled their hair automatically. One of the participants described automatic hair pulling as a behaviour that occurred sometimes and one as often. None of participants described their behaviour as intentional, although 2 of them were not able to say if it was intentional. For 2 participants, hair pulling was often accompanied by feelings of relief or pleasure, while the other 2 had never felt relief or pleasure after pulling hair. Tension before or when trying to resist pulling hair has often been felt by one participant; another participant described it as occurring always and 2 other participants as never. Some characteristic factors related to hair pulling are presented in Table II. Analysing specific factors related to hair pulling behaviour we did not find any differences between females and males and between individuals with and without any anxiety disorder diagnosis (p > 0.05).
Table II. Characteristics of current hair pulling
Epidemiological studies on lifetime and point prevalence of TTM are scanty. Most of them estimate TTM in children, adolescents and young adults, in accordance with the fact that TTM is observed more commonly in younger individuals. The lifetime prevalence in these groups is reported as between 0.5% and 1% and the point prevalence amounts to 0.5% (7, 8). Higher rates are reported in the specific group of dermatological patients, namely up to 7% (9). In our study TTM occurred during lifetime in 8 participants (2.4%). The current TTM was diagnosed in 4 individuals (1.2%). Those rates are slightly higher than those reported in previous studies (6–8).
TTM is diagnosed more frequently in female patients. Epidemiological studies also confirm higher rates of TTM in females than males, with the female to male ratio varying between 2:1 and 7:1 (8, 12–14). Our findings are consistent with previous studies, with the lifetime prevalence in females being 2.9%, in males 1.5%, and the point TTM rates as 1.0% and 1.5%, respectively.
With the exception of 8 participants who had a lifetime TTM diagnosis, 4 individuals (1.2%) reported hair pulling that did not meet the TTM diagnostic criteria; 3 females (1.4%) and one male (0.8%). Christenson et al. (7) reported hair pulling resulting in visible hair loss, but failing to meet diagnostic criteria in 1.5% of males and 3.4% of female college students. In other studies hair pulling among university students that were not diagnosed as TTM occurred more commonly; 11.0–15.3% (10, 11). The mean age of onset of TTM is estimated to be 12 years (2, 3). In our study the age of onset was higher, almost 17 years (age range 11–24 years).
Statistically significant differences were found in the lifetime prevalence of anxiety disorders between individuals with and without TTM. Our findings are consistent with data published by Christenson et al. (15), who investigated the association of TTM and anxiety disorders among adults (15). Lifetime anxiety disorders were diagnosed in 62.5% of subjects with TTM, the rate being higher than in the general population, as well as among examined individuals without TTM (20.2%). In contrast to the findings reported by King et al. (8) or Stein et al. (17), who indicated an association of TTM and OCD, our study did not diagnose OCD among individuals with TTM, while it did diagnose OCD in 14 persons (4.3%) without TTM. Given the limited size of our group with point diagnosis of TTM, this issue needs to be explored further. We found that TTM is often accompanied by nail biting or nail picking. Three out of 8 participants with lifetime TTM (37.5%) also reported onychophagia and 2 of them (25%) onychotillomania. Moreover, in 3 of 4 persons with hair pulling that did not meet diagnostic criteria of TTM we have also reported onychophagia. Onychophagia was more common in the group without TTM (47.3% of 331 persons) than in the group with TTM, while onychotillomania occurred less frequently (0.3% vs. 25%). Due to the small size of the TTM patient group it becomes difficult to explain any differences between these groups. This kind of association needs further investigation involving a larger group of participants with diagnosis of TTM. We did not find any published data regarding onychotillomania and onychophagia in patients with TTM.
We analysed some characteristic features related to hair pulling behaviour among individuals with current TTM. Considering subtypes of hair pulling (27, 28), we could classify hair pulling as automatic behaviour in 2 of 4 individuals. Two out of 4 participants described their behaviour as intentional activity, and the other 2 could not specify whether it was intentional. In none of our cases hair pulling was identified as “focus behaviour.” All individuals, on the other hand, described their hair pulling as automatic. They reported having always pulled out hair without thinking about it, sometimes or even often during other daily activities, such as reading, watching television or working at a computer. It has been estimated (29) that approximately 75% of individuals with a diagnosis of TTM diagnosis have an automatic type of the disorder, associated with more intensive tension occurring before hair pulling, but our study could not confirm this hypothesis. Some authors indicate that automatic and focused often co-occur and characteristic features of hair pulling behaviour, such as tension or pleasure, vary in the same individuals depending on the mood, situation, etc. (30). This is consistent with the reports of our participants.
In conclusion, the findings of this study regarding the prevalence of TTM and its association with anxiety disorders are consistent with data from previous studies, but differ with respect to OCD comorbidity. However, the current study has several limitations. The examined group was recruited from students, i.e. from a non-clinical sample. None of participants with diagnosis of TTM has ever sought professional help neither by visiting a psychiatrist nor a dermatologist because of the hair pulling. We may hence assume their TTM symptoms to be less severe than in patients requiring treatment. Another limitation is the small size of the group with the diagnosis of TTM; this makes a good estimate of the frequency of single TTM characteristics. Our results on comorbidities and clinical features of hair pulling behaviours should therefore be interpreted with caution.
The authors declare no conflict of interest.


 Click to show fullsize
Click to show fullsize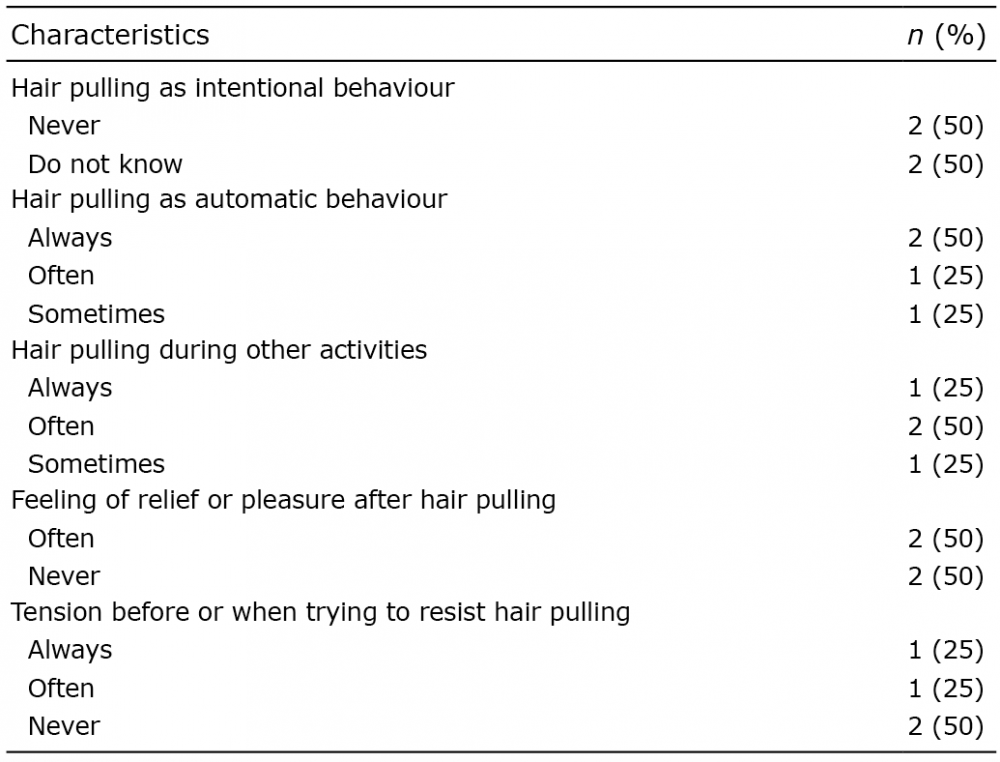 Click to show fullsize
Click to show fullsize