


1Institute of Dermatology, Department of Clinical-Surgical, Diagnostic and Pediatric Science, and 2Department of Pathology, IRCCS Foundation Policlinico San Matteo, University of Pavia, Pavia, Italy. E-mail: v.brazzelli@smatteo.pv.it, vbrazzelli@libero.it
Accepted Nov 8, 2016; Epub ahead of print Nov 9, 2016
Human herpesviruses (HHVs) are frequently considered as aetiological agents or cofactors in cutaneous diseases (1). However, clearly established HHV-7 associations are rare. We describe here a case in which diagnostic techniques led to viral detection and a better dermatological diagnosis.
A 50-year-old man was referred to the department of dermatology with a diffuse erythemato-papular rash, spreading from the trunk to the limbs and neck, accompanied by intense pruritus (Fig. 1).
Fig. 1. Erythematous papular eruption on the trunk.
The patient’s medical history was unremarkable, no prodromal symptom was present, and he denied drug use, both routinely and in the days before the eruption. Laboratory investigations were negative or within normal ranges, except for mild lymphocytosis (3.9 × 103/mm3; normal range 1.5–3 × 103/mm3). A diagnosis of urticaria papulosa/insect bites was suspected.
The patient returned 3 days later due to persistent lesions. Skin biopsies were performed and the histological findings showed an interface dermatitis, with rare lymphocytes along the dermo-epidermal junction, and a scarce, superficial perivascular lymphocytic infiltrate. The epidermis showed a mild spongiosis, lymphocytes exocytosis and rare single necrotic keratinocytes. No eosinophils were evident. An orthokeratotic stratum corneum with a preserved basket-weave aspect was seen, demonstrating the acute nature of the process (Fig. 2).
Fig. 2. Histological examination of a papule: (a) An interface dermatitis, with lymphocytes along the dermo-epidermal junction, and a scarce, superficial, perivascular lymphocytic infiltrate (haematoxylin and eosin (H&E) ×10). (b) The epidermis shows a mild spongiosis, lymphocytes exocytosis and rare single necrotic keratinocytes. No eosinophils are evident. The stratum corneum is orthokeratotic, with a preserved basket-weave aspect (H&E ×40).
The most common infectious agents associated with cutaneous rashes (secondary syphilis, HSV 1–2, VZV, CMV, EBV, HHV-6, HCV, HBV, HIV, parvovirus B19, Coxsackie and echovirus) were excluded by serological testing or count of DNA copies in blood samples. The only notable finding was the detection of circulating HHV-7 DNA (800 copies/ml) in the blood, which is considered significant for active infection. A diagnosis of HHV-7 related papular rash was suggested.
Four weeks after the beginning of the eruption, the rash cleared completely without scaling and HHV-7 DNA was undetectable in blood samples.
HHV-7 was discovered in 1990 as a new member of the beta-herpesvirus subfamily. It is closely related to HHV-6, sharing a strong genetic homology and the CD4+ cells tropism (1).
Unlike HHV-6, HHV-7 does not integrate into the host DNA; thus, detection of HHV-7 DNA in patient blood using real time PCR implies active infection (1).
Primary infection occurs early in life and manifests as exanthema subitum, or other febrile illnesses mimicking measles and rubella. According to serological studies, it is estimated that more than 90% of children up to the age of 5 years present with HHV-7 primary infection. Reactivation is extremely common and can be totally asymptomatic. HHV-7 has recently been identified as an emerging pathogen in transplant recipients and may exacerbate graft-versus-host disease (2, 3).
From a dermatological perspective, the possible association of HHV-7 with pityriasis rosea has been a matter of discussion since 1997, when Rebora et al. (4) suggested a causative role of HHV-7 in the pathogenesis of the disease. Currently, the only cutaneous rash clearly associated with HHV-7 is exanthema subitum, which is also associated with HHV-6, although HHV-7 and HHV-6 are also considered in the aetiology of lichen planus, graft-versus-host disease, recurrent vulvar ulcers and drug-induced hypersensitivity syndrome (5–7).
Specific HHV-7 cutaneous papular rash has not been described so far; HHV-7 reactivation is often unapparent and asymptomatic, but the concomitant detection of HHV-7 DNA in the blood of a patient with cutaneous rash could be considered to be linked to the dermatological symptoms. Furthermore, the clinical remission of the skin eruption and the disappearance of HHV-7-DNA in the blood are indicative of a correlation.
The histopathological findings in our case exclude insect bites, but suggest viral rash and/or drug eruption. The patient denied drug intake, thus we correlate this papular rash with HHV-7 infection.
In conclusion, although no specific treatment is known for many viral exanthemas, their recognition allows clinicians to differentiate such diagnoses from other cutaneous diseases and to provide more accurate answers to patients’ questions.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize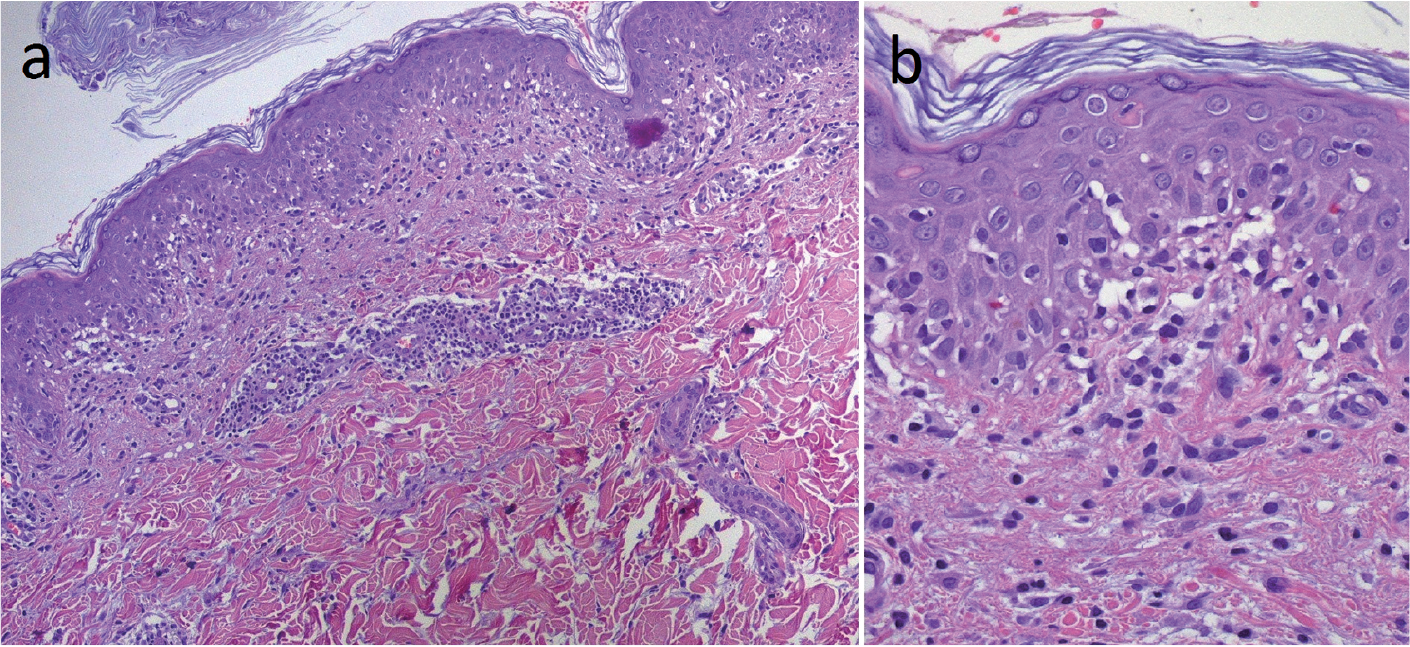 Click to show fullsize
Click to show fullsize