


1Department of Dermatology, Nantes University Hospital, 2CIC, INSERM 892, 3Service d’Anatomie et Cytologie Pathologiques, 4Laboratoire de biochimie plateforme de génétique des tumeurs, and 5Institut Urologie-Néphrologie, Nantes University Hospital, Nantes, France
The aims of this study were to determine the clinical and histological characteristics of melanoma in transplant recipients, the mutation profile (BRAF, NRAS and c-KIT genes), and the immune tolerance of the tumour microenvironment by immunohistochemical study of the expression of indoleamine 2,3-dioxygenase (IDO), PD1, PD-L1, CD8 and FoxP3. The study population comprised patients who had undergone a renal transplant in Nantes University Hospital who developed post-transplantation melanoma. Twenty cases of melanoma out of 4,663 transplant recipients were studied. The results differed from the usual data with respect to melanoma site: 40% were located on the face and were of the malignant lentigo type. The mutation profile was concordant with that of the immunocompetent population. IDO was expressed in all the sections tested, while CD8, FoxP3, PD1 and PD-L1 were poorly expressed. This reflected a highly immunodepressed tumour environment, raising the question of the inductive role of IDO on tumour immune tolerance in patients presenting with long-term immunodepression.
Key words: melanoma; organ transplant recipients; IDO; BRAF mutation; malignant lentigo.
Accepted Nov 8, 2016; Epub ahead of print Nov 10, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Brigitte Dréno, Department of Dermatology, Nantes University Hospital, 1 place Alexis Ricordeau, FR-44093 Nantes Cedex, France. E-mail: Brigitte.dreno@wanadoo.fr
Organ transplant recipients are increasing in number and their long-term survival is improving (1). The patients require long-term immunosuppressant treatment (2). The prolonged modification of the immune system of organ transplant recipients is associated with a risk of developing various forms of cancer, mainly skin cancer (3, 4). The risk of developing post-transplantation melanoma is 2- to 3-fold higher than that of the overall population, with a poorer outcome in transplant recipients (5–7). The literature on melanoma in that population is not abundant; few data are available with regard to translational research on melanoma in organ transplant recipients (8). This study had 2 objectives: a clinical objective consisting in determining the main clinical and histological characteristics of melanoma in transplant recipients. The second objective was to examine histological specimens of primary melanoma emerging post-kidney transplantation in patients at Nantes University Hospital, to determine the mutational profile (BRAF, NRAS, c-KIT genes) of the melanoma and the degree of immune tolerance of the tumour microenvironment by studying the markers of innate immunity: indoleamine 2,3-dioxygenase (IDO), programmed cell death 1 (PD1), programmed cell death ligand 1 (PD-L1), CD8 and FoxP3. The choice of innate marker has been performed to evaluate the immunosuppressive state of the microenvironment of melanoma.
IDO expression causes infiltrating effector T cells to arrest in G1, become anergic, and die by apoptosis. In addition, toxic metabolites of tryptophan can directly suppress tumour-infiltrating T cells. Finally, IDO-expressing dendritic cells can induce systemic anergy by expanding proliferation of T regulatory cells. PD-1 is an immune checkpoint protein of T lymphocytes, whose link with its ligand PD-L1 expressed by melanoma cells and dendritic cells, induces inhibition of activation of T lymphocytes. FoxP3 is a marker of T reg cells inhibiting the activation between T lymphocytes and melanoma cells and CD4 are cytotoxic T cells directed against melanoma cells
Our hypothesis was that long-term immunosuppression in such patients could induce a decrease in innate immunity, for which one of the consequences was, in particular, an increase in the prevalence of melanoma in that population.
This retrospective study included all kidney transplant recipients in the Immunology and Nephrology Department of Nantes University Hospital who developed post-transplantation melanoma from 1970 to May 2015. Patients were identified from the dermatological monitoring of transplantation recipients and software for computerized and validated transplantation data (DIVAT) (9) developed by the Immunology and Nephrology Department. DIVAT is a database that prospectively collects medical information on all adult kidney and/or pancreas transplant recipients, using software that enables data retrieval from the database for epidemiological analysis. For dermatological follow-up, organ transplant recipients are followed either in a dedicated dermatology clinic in Nantes or in outpatient clinic consultations (i.e. open-care practice), in which patients make their own appointment and take charge of their own dermatological monitoring (although they are reminded to do this at each visit); while in the dedicated dermatology clinic, appointments are made for the patients by hospital staff. The choice between open-care practice and the dedicated dermatology clinic is not made by the doctors: all organ transplant recipients are offered a dedicated dermatology clinic. Some patients declined this offer due to the distance from their home to the hospital, and others already had a dermatologist and did not wish to change their usual practice.
The clinical and histological characteristics, BRAF, NRAS and c-KIT mutations, and immunohistochemical expression of the markers IDO, PD1, PD-L1, CD8 and FoxP3 were collected.
Analysis of the BRAF, NRAS and c-KIT genes was performed on formalin-fixed paraffin-embedded sections of the primary melanoma tumours and metastases, when available. DNA was extracted from 10-µm thick sections, after macrodissection using an iPrep purification system. Detection of BRAF V600 mutations was performed by allele-specific amplification as previously described (10) (Table I). Detection of NRAS (exon 3) and c-KIT (exons 11, 13 and 17) mutations was performed by conventional Sanger DNA sequencing, as described (11). Primers used for amplification and sequencing are available upon request.
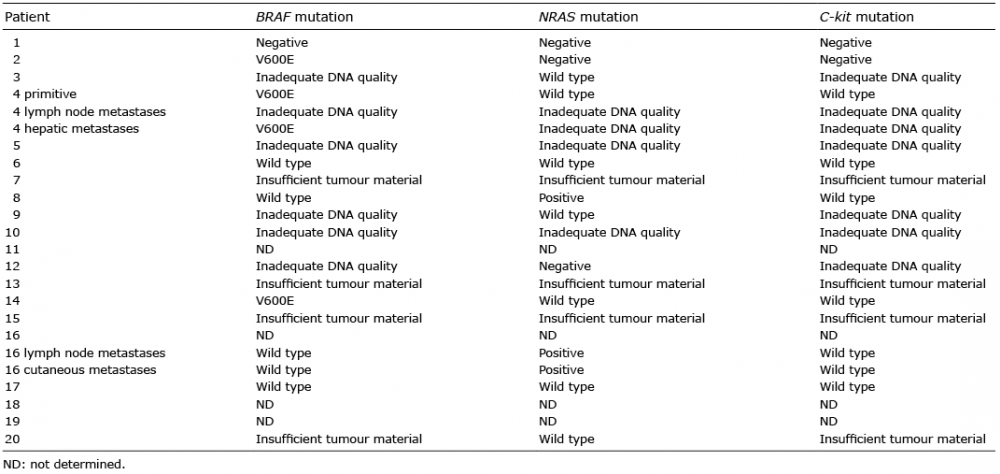
Table I. Mutations results in renal transplant patients
The immunohistochemical method is a qualitative and semi-quantitative immunoenzymatic method enabling antigen localization on tissue sections. The target antigens were recognized using specific antibodies. The expression of IDO (clone 4D2 supplied by Serotec), PD-1 (clone NAT supplied by Abcam), PD-L1 (polyclonal antibody supplied by Abcam), CD8 (clone C8/144B supplied by Dako) and FoxP3 (clone 236A/A7 supplied by Ebioscience) was investigated on the sections of the same paraffin-embedded primary melanoma specimens. The percentage of IDO- and PDL-1-positive cells represented melanoma cells, and the percentage of FoxP3 and CD8 and P-1 positive cells represented T lymphocytes. The same markers were investigated on 6 non-immunodepressed control patients whose embedded specimens were available at the Nantes pathology laboratory. The 6 control samples were the 6 primary melanomas in non-immunosuppressed patients that we had in our bank. The immunohistochemical method was implemented using the streptavidin-peroxidase method described previously (12) on paraffin-embedded sections. Slides were read using a Leica microscope by 2 independent observers under blind conditions. Labelling was assessed using the following scale: 0: no expression (0); 1: weak expression (1–25% positive cells); 2: moderate expression (25–50% positive cells); 3: high expression (50–75% positive cells); and 4: very high expression (> 75% positive cells), and the results were reported as the mean of the labelling determined by the 2 observers.
Twenty patients with 20 melanomas were included out of the 4,663 renal transplant recipients, i.e. a prevalence of 4.29/1,000 (Table II); 65% of cases were men (n = 13). Median age at transplantation was 51.9 years (age range 19.1–72.2 years). Median age at diagnosis of melanoma was 64.5 years (age range 31.3–79.6 years).
Table II. Clinical and histological characteristics of the renal transplanted patients
There were 9 deaths (45%), of which 5 (20%) related to the melanoma occurring in a median time from the diagnosis of melanoma of 1.3 years (range 0.14–8.1 years).
The mean Breslow thickness (Br) was 1.58 mm (0–18 mm) for the 17 data available. There were 9 superficial spreading melanomas, 3 nodular melanomas, 2 mucosal (ethmoidal, conjunctival) melanomas, 4 melanomas in a context of malignant lentigo, 1 unclassifiable melanoma, and 1 case of missing data. Patient with malignant lentigo were phototype I except for 1 (phototype II); for the other melanoma types, phototype was II for 66% and phototype III for 33%. Five melanomas were ulcerated, 6 were non-ulcerated and 9 had missing data. Three out of the 8 melanomas for which the data were reported occurred on a pre-existing naevus. Four melanomas were located on the trunk, 8 on the face, 4 on an arm, 2 on a leg and 2 on the mucosa. Eleven melanomas were detected during the dedicated follow-up consultation of transplant recipients in the Dermatology Department (median Br: 0.5 mm (0–6 mm)) and 9 in outpatient clinic consultation (median: 2.98 mm (0.25–18 mm)).
The 6 melanoma in non-transplant patients of our bank corresponded to: 4 men and 2 women, mean age 73 years, locations: 1 face, 1 trunk, 3 arm,1 leg; mean Br 2.07 mm (Table III).
Table III. Clinical and histological characteristics of the control patients
Mutations could not be investigated in 4 samples because the FFPE specimen had been destroyed (older than 20 years). For some of the collected sample, the percentage of tumour cells was too low, or the DNA extracted could not be amplified. In the evaluable tumours, BRAF and NRAS mutations were found in 4 cases (4/10; 40%) and in 3 cases (3/13; 23.1%), respectively. No c-KIT mutations were detected (0/9; 0%).
Fig. 1. Representative picture of indoleamine 2,3-dioxygenase (IDO) expression in cutaneous primary melanoma. (A) IDO-positive cells were detected by immunohistochemistry (×10). Negative control (B) (×10).
A total of 17 embedded specimens was analysed. Among the transplant recipients, there was no expression of PD1, PD-L1, FoxP3 (mean expression intensity, as per the scale used, of 0.06, 0.06 and 0.12, respectively). CD8 was weakly expressed in 6 out of 17 embedded specimens (mean intensity: 0.35). IDO was expressed in all the test specimens: highly in 5 specimens, very highly in 3 specimens and moderately in 7 specimens (mean expression intensity: 3).
For the control patients (n = 6), the mean intensity of IDO, PD1, PD-L1, FoxP3 and CD8 expression was 2, 1.25, 1.67, 1.17 and 1, respectively.
The number of melanomas studied, n = 20, in a single centre was substantial. The clinical data generated by the study were consistent with the published data (13, 14) except for the frequency of melanomas developing on a pre-existing naevus (15–17) that were not frequently identified. However, there were missing data. It should also be noted that there were 2 mucosal melanomas (10%) with an unusual site (ethmoidal and conjunctival) not generally identified in the literature. The site and type of melanoma also differed from the usual data (18). The trunk was a less frequent site in our patients. In contrast, 40% of melanomas were on the face and of the malignant lentigo type. Those proportions have not been reported previously. This raises the question of the role of chronic exposure to ultraviolet (UV) radiation as a risk factor in the target population. While we were not able to collate phototype and exposure to UV radiation for all the patients, the predominant phototype in the region is I–II. This is a possible explanation for the increased frequency of malignant lentigo in the study population. Patients with malignant lentigo were mainly phototype I (3/4). Our patients’ phototypes are in agreement with our region of the West of France, where more than 80% of patients are phototype I to III.
The dedicated dermatological consultations enable systematic and regular follow-up of the patients, minimizing those lost to follow-up and enabling melanoma diagnosis at an earlier stage than for patients followed up in an open-care practice with a median Breslow depth of 0.5 vs. 2.98 mm, doubtless because in outpatient clinic consultation, patients must make their own appointment with a dermatologist.
Some patients do not attend dermatological follow-up. This could reflect the difficulty of rapid and easy access to dermatological consultations in open-care practice, but may also reflect a lack of awareness by transplant recipients of the importance and need for dermatological follow-up when the patients also have numerous other specialized consultations (nephrology, urology, cardiology, endocrinology, etc.). It would doubtless be beneficial with a view to decreasing the thickness of the melanoma at diagnosis and thus enhancing the prognosis, for the transplantation team to systematically make their patients aware of the cutaneous neoplastic risks they incur and the importance of systematic dermatological follow-up. Thus, dedicated dermatological consultations for transplant recipients should be developed in transplant centres.
Analysis of the mutation profile of our transplant recipients’ melanomas was limited by the numerous non-informative analyses due to impaired DNA quality. This is explained by the age of the embedded specimens (9 embedded specimens out of 20 were more than 10 years old). Also, the fixation medium used influences the quality of material preservation. The Bouin’s fluid frequently used by histology laboratories is not recommended for molecular biology methods. Finally, 4 embedded specimens were destroyed after 20 years of storage. The difference in the number of responses for BRAF vs. NRAS is related to the fact that we were working with very fragmented DNA (FFPE specimens). The amplicon corresponding to NRAS exon 3 is shorter than the one amplified for BRAF exon 15 (162 bp and 224 bp, respectively). This probably explains the higher rate of successful sequencing for the NRAS gene. The proportion of BRAF mutant melanomas (40%) is concordant with that for immunocompetent subjects, enabling targeted therapy to be envisaged in the event of metastatic progression of the melanoma. It is to be noted that the 2 mucosal melanomas were not c-KIT mutated.
Study of the immunity of the tumour microenvironment showed that IDO was expressed in 100% of the transplant-recipient specimens and more intensely than in the microenvironment of immunocompetent patients’ melanomas. There was, however, little or no expression of CD8, FoxP3, PD1 or PD-L1. This, therefore, reflects a highly immunodepressed tumour environment inducing an absence of T-cell activation and hence the absence of CD8, PD1 and FoxP3 (19–21). The absence of CD8 infiltration having, as a consequence, an absence of INF secretion, it is logical that no PD-L1 expression was found. The current study was limited in terms of the quantity of material and hence in the choice of the immunity markers to be studied so as not to exhaust the specimens. For that reason, we were not able to test CD3 expression. The absence of PD1 expression suggests that PD1 inhibitors would not be a good therapeutic approach in transplant recipients, but this result needs to be confirmed on metastasis biopsy specimens. The absence of expression of PD-1 by T lymphocytes infiltrating the metastasis and the absence of PDL-1 expression by melanoma cells argues for thinking that anti PD-1 alone could not be a good therapeutic approach. In the literature, the clinical response with anti-PD1 has been associated with the expression of anti-PDL-1 but not with anti-PD1 (22). However, these results are debated. The strongest conclusion is that in melanoma PDL-1 negative cases, combination “ipilimumab and anti PD1” induces significantly more responses (23). However, the high risk of severe autoimmune adverse effects in the context of transplantation could be an obstacle. Clinical trials are needed to determine this.
The immunolabelling results raise the question of the inductive role of IDO on the development of tumour immune tolerance in transplant recipients. The high in situ production of IDO may be induced by the long-term anti-rejection treatments taken by transplant recipients. The median duration between transplantation and melanoma diagnosis, and hence the duration of immunosuppression, was 11.9 years (range 0.3–27.7 years) in our transplant-recipient population. IDO is a potent immunosuppressive enzyme that has gained attention in recent years. IDO-induced tryptophan degradation inhibits the proliferation of T cells, accelerates T-cell apoptosis and triggers cell cycle arrest. The published data show that there is a correlation between the intensity of IDO expression and the poor prognosis of cancers in which it is expressed (24–27). We know that melanomas in transplant recipients have a worse prognosis than those in the immunocompetent population (28, 29). This has also been found in our series. It has been shown that IDO expression can be increased in metastatic lesions and its expression is correlated with disease progression rate (30, 31). Thus, our results show that the more frequent development of melanoma in transplant recipients could be related to local IDO production induced by immunosuppressant treatments. IDO thus appears to be a molecule that may play a major role in the induction of immune tolerance of melanoma cells via the microenvironment. Until now no correlation between IDO expression and transplant drugs has been observed. However, these data need to be confirmed in a larger patient population and by quantitative reverse transcriptase PCR. This was not possible in our study due to the age of the embedded specimens and poor DNA quality. Our study was conducted only on the primary melanoma. Furthermore, the sample was too small to make a statistical comparison, which is a limitation of the current study.
In conclusion, the data generated by this study differ from those in the literature with regard to primary melanoma site, which was the head in 40% of cases in our series with a malignant lentigo histological type. The mutation profile of the melanomas in our transplant recipients was concordant with that of the immunocompetent population. Our study was the first to show that IDO could play an important role in the development of cutaneous immune tolerance from innate immunity. This finding supports the value of IDO inhibitor treatment in patients on adjuvant therapy at the primary or local/regional stage associated with targeted therapies or monoclonal antibodies at the metastatic stage.
The authors gratefully acknowledge DHU1 (University Hospital Department 1, Nantes University Hospital) for providing funding for this work.


 Click to show fullsize
Click to show fullsize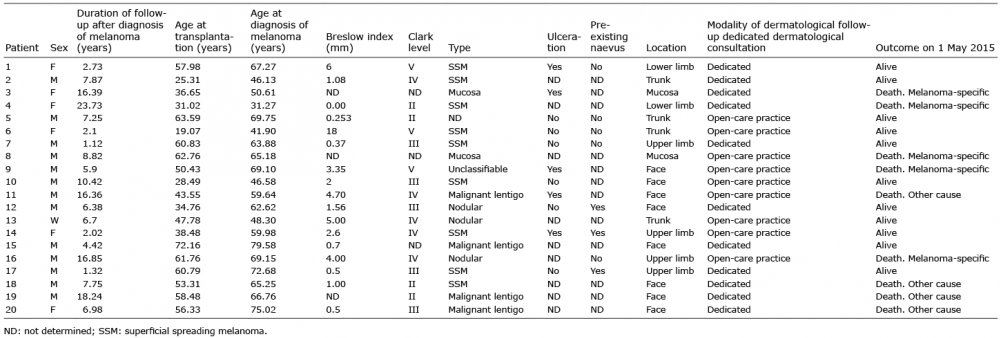 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize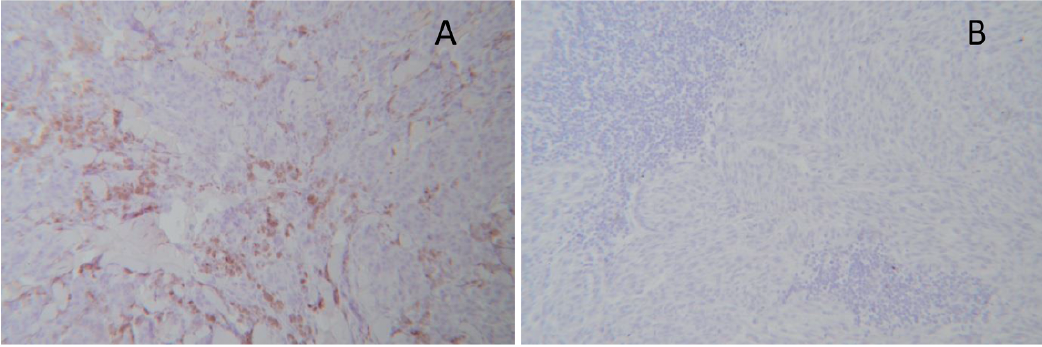 Click to show fullsize
Click to show fullsize