


1Pediatric Division and 3Department of Dermatology, Hadassah-Hebrew University Medical Center, and 2Faculty of Medicine, Hebrew University, Ein Kerem, Jerusalem, Israel
Erythema multiforme (EM) is an immune-mediated reaction presenting as acrofacial target lesions. Most studies utilize the outdated classification, which includes EM, Stevens–Johnson syndrome and toxic epidermal necrolysis as related entities. We describe here epidemiological, aetiological, clinical, laboratory and treatment characteristics of paediatric EM. This is a retrospective single-centre study, performed between 2000 and 2013. Of 119 children given a diagnosis of EM, only 30 met clinical criteria and were included in this study. Most misdiagnosed cases were non-specific eruptions and urticaria multiforme. Mean age was 11.3 years. Fifty percent had mucosal involvement. An aetiology was observed in half of the patients. Seventy percent of patients were admitted to hospital, 46.7% were treated with systemic steroids. Sixteen percent had recurrent EM. The most common identified infectious agent associated with EM in this study was Mycoplasma pneumonia and the cases associated with this infection may represent the recent entity, mycoplasma-induced rash and mucositis. Association with herpes simplex virus was not observed. Despite being a benign, self-limiting condition, children were over-treated in terms of hospitalization and therapy.
Key words: erythema multiforme; children; erythema multiforme minor; erythema multiforme major.
Accepted Nov 8, 2016; Epub ahead of print Nov 10, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Vered Molho-Pessach, Department of Dermatology, Hadassah-Hebrew University Medical Center, Kiryat Hadassah, POB 12000, Jerusalem, 9112001, Israel. E-mail: rverem@hadassah.org.il
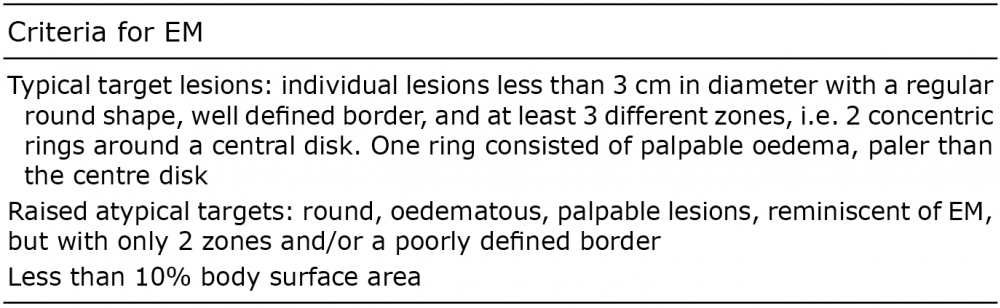
Erythema multiforme (EM) is a self-limiting, immune-mediated reaction, which manifests with a typical mucocutaneous eruption. The characteristic skin lesion of EM is the target lesion, which measures <3 cm in diameter, has a round shape and well-defined border, and consists of 3 distinct zones; 2 concentric rings of colour change surrounding a central circular zone, which tends to have a dusky appearance, manifesting damage to the epidermis in the form of a bulla or crust. Atypical lesions with only 2 different zones and/or a poorly defined border may also exist (1). The rash tends to involve acrofacial sites. It may be confined to the skin and is then termed EM minor, or it may involve mucosal membranes, and is then termed EM major (2, 3).
First described by von Hebra in 1860, EM had long been considered as part of a spectrum of diseases, including EM minor, EM major, Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) (4). These entities were thought to represent an immune reaction to one of several different aetiologies, which could be limited to the skin, extend to involve mucosal membranes, or present as a systemic inflammatory state, with significant morbidity and mortality (5). In 1993 Bastuji-Garin et al. (6) proposed a novel classification: EM as a different entity from SJS/TEN, with its own aetiology, pathophysiology and clinical course. EM has several different aetiologies; the most common cause is infectious, encompassing approximately 90% of cases (7). Herpes simplex virus (HSV) is estimated to be the cause of EM in approximately 70% of patients (8) and preceding herpes labialis is noted in 50% of subjects with EM. In these cases, EM tends to recur several times (9). Mycoplasma pneumoniae is also a prominent pathogen, which may also be associated with SJS (10, 11). Various other aetiologies have been associated with EM (drugs, auto-immune disorders, malignancy, radiation, etc.), but are considered of far less importance (3).
EM affects mostly young adults, but can also appear in children (4). Most of the previous studies describing paediatric EM refer to the outdated classification of EM as part of the EM–SJS–TEN spectrum (12–15).
The aim of this study was to characterize paediatric EM as a separate entity, and to describe epidemiological, aetiological, clinical, laboratory and treatment characteristics in this population.
This retrospective epidemiological descriptive study was conducted at the Hadassah Hebrew University Medical Center, a tertiary hospital in Jerusalem, Israel. Data on all cases of children (age range 0–18 years) with a clinical diagnosis of EM (ICD9 695.11, 695.12, 695.10.09, 695.19) who were examined at our emergency, paediatric or dermatology departments or at the dermatology outpatient clinic, between the years 2000 and 2013 were extracted. A paediatric dermatologist reviewed the medical data of all extracted cases. Only cases consistent with the classification criteria for EM, proposed by Bastuji-Garin et al. (6) (Table I) were included in this study.
Table I. Criteria for diagnosis of erythema multiforme (EM) (from Bastuji-Garin et al. (6))
The following data were retrieved from patients’ computerized medical charts: epidemiological data (age, sex, ethnicity); medical history (complaint characteristics, history of viral illness, accompanying symptoms, history of medication); physical examination (vital signs, rash description, mucosal involvement, other physical findings); laboratory data (complete blood count, basic chemistry, inflammatory markers and microbiological data) and histopathological report if a biopsy was performed.
The study was approved by the local institutional review board.
Statistical analysis was performed using SPSS version 20. Mean and standard deviations were calculated for quantitative variables, and absolute and percentage frequencies for nominal variables.
During the years 2000 to 2013, 119 children were given a diagnosis of EM at the Hadassah Hebrew University Medical Center. Based on the classification criteria for EM proposed by Bastuji-Garin et al. (6), 89 cases were excluded (Table II). Of these, 29 patients had clinical features consistent with urticaria multiforme (UM) and were all younger than 4 years. Fifty-six patients were excluded due to non-specific eruptions that did not fulfil the diagnostic criteria for EM. Thirty children, age range 4–18 years, were eventually included in this study; their demographic characteristics are presented in Table III.
Table II. Excluded cases
Table III. Demographic characteristics of patients with erythema multiforme
The mean duration of rash prior to presentation at the hospital was 5.2 ± 5.8 days (range 0–21 days).
The eruption was most commonly located on the upper limbs, followed by the lower limbs, trunk and face (80%, 70%, 56.7% and 23.3%, respectively). Fifteen patients had EM minor, and 15 had EM major. Oral involvement was observed in all 15 patients with EM major, genital involvement was observed in 4 patients, and ocular involvement in 2 patients. Five patients had involvement of more than one mucous membrane.
Data of body temperature were available for 22 children, 8 of whom (36.4%) had fever > 37.5°C. Abnormal findings on physical examination included enlarged submandibular lymph nodes in 2 patients, enlarged cervical lymph nodes in one patient and oral aphtous ulcers in one patient. Laboratory markers for inflammation or infection were elevated in up to 75% of patients tested for these markers (Table IV). Electrolytes, kidney and liver function tests were normal in nearly all cases (one child had mild hyponatraemia).
Table IV. Laboratory signs of infection in patients with erythema multiforme
Aetiologies for EM are presented in Table V. More than one-third of the patients reported a febrile illness in the month prior to the appearance of EM. Seven patients reported past history of HSV, but none had evidence of a recent HSV infection, through history, physical examination, or positive serology or PCR for HSV (the last 2 were negative in 8 children in whom these tests were performed), Tzanck smear was performed in only 2 cases, and was found to be negative in both. Mycoplasma pneumoniae infection was found in 4 out of 14 examined (positive PCR or IgM antibodies). All 4 patients were febrile, 2 had EM minor and 2 had EM major with involvement of 2 or more mucous membranes. All 4 patients presented with eruption of target lesions, limited to 1 or 2 body sites (face, trunk or extremities).
Table V. Possible aetiologies for erythema multiforme
Other, less common, possible aetiologies, were other bacterial infections, new medications and systemic lupus erythematosus. In 50% we could not identify a possible aetiology.). None of the children had a history of other dermatological disorders or an episode of EM in their family. Skin biopsy was performed in 6 children, pathology was characteristic for EM in 5 of them. Non-specific findings were observed in one patient.
Twenty-one (70%) patients were hospitalized. Hospitalization lasted for a mean of 3.4 ± 3.5 days (range 0–11 days). Fourteen patients (46.7%) were treated with antihistamines, 14 (46.7%) with systemic steroids, 10 (33.3%) with antibiotics, 10 (33.3%) with systemic acyclovir, 7 (23.3%) with intravenous fluids, and 5 (16.7%) with topical corticosteroids. In 3 patients (10%) a medication was discontinued. Five (16.7%) of the children had recurrence of the disease, with 1–11 additional episodes (mean 3.4 episodes) that recurred within 0.5–72 months (mean 19.1 months). Children experiencing recurrences were older, with a mean of 14.5 years (range 12–17.5 years). In only one patient with recurrence was there a history of previous HSV infection; however, this was not recent.
In the past 2 decades, EM has been recognized as a separate entity from SJS/TEN, and several studies examining EM in the general population have been performed (16, 17). However, until recently, there has not been specific focus on paediatric EM. In the last year, 2 retrospective studies focusing on paediatric EM were published. Keller et al. (18) performed a 10-year survey of non-bullous EM in hospitalized children. Ninety-five children were included in this study, which found a precipitating factor in the majority of patients; medications in the first year of life and medications and various infections in children older than one year old. The study was conducted by paediatricians and none of the authors were dermatologists. The lack of dermatological expertise raises doubts regarding the accuracy of EM diagnosis in this study. This is further emphasized by the findings of another recent study performed by Read & Keijzers (19), describing paediatric EM in the emergency department. Out of 70 patients given a diagnosis of EM, only 9 cases fulfilled classification criteria for EM, all were classified as EM minor, with the majority attributed to viral infections. The most common misdiagnosis was UM, a variant of annular urticaria seen in infants and toddlers. Only 30 cases of paediatric EM were included in our retrospective study, due to our adherence to strict diagnostic criteria. Therefore, out of 119 children given a diagnosis of EM in the study period, only 30 fulfilled the classification criteria after review by a paediatric dermatologist, and were included in this study. The most common misdiagnoses were non-specific eruptions and UM.
In our cohort, the mean age of affected children with EM was 11.3 ± 4.4 years, ranging from 4 to 18 years. As opposed to the studies by Keller et al. (18) and Read Keijzers (19), we did not observe EM in infants and toddlers. Most of the misdiagnosed cases in this age group were due to UM, which is characterized by widespread targetoid lesions, but is evanescent and migratory and is accompanied by acral oedema and dermatographism (20); features which are not part of EM. The ratio of males to females was 1:2, which is consistent with a slight female preponderance described previously (3), but may be skewed due to our small sample size.
In our study there were several indications of an infectious aetiology in half of the children, either a history of a preceding febrile illness in the month prior to the appearance of the eruption, fever at presentation, or a positive laboratory result for M. pneumonia, or other bacterial infections. Although nearly one-quarter of patients reported a history of HSV infection, a recent episode of HSV in the weeks prior to the appearance of EM was not documented in this study. In adults, HSV has been implicated as the most common aetiology of EM, in up to 70% of cases (8). However, the few studies focusing on paediatric EM report an association with HSV in 0–14% of cases (18, 19, 21), indicating, in accordance with our findings, that HSV is not a prominent cause of EM in children.
We did not identify other specific viral pathogens as possible triggers for EM; however, more than one-third of patients reported a recent non-specific febrile illness prior to the appearance of EM, which may have been a viral infection. Association with viral illness in children has been previously reported (19, 21), but the exact prevalence of the causative viruses in yet unknown.
Four of our patients were shown to have an infection with M. pneumoniae. Recently, a new entity was suggested for patients with EM or SJS associated with M. pneumoniae infection: Mycoplasma-induced rash and mucositis (MIRM), which is characterized by prominent mucositis and usually sparse cutaneous involvement with a polymorphous morphology, and has been described mainly in children and young adults (22). Only 2 of the 4 patients with associated Mycoplasma infection in our study had mucosal involvement. All 4 patients presented with fever and a cutaneous eruption of target lesions, limited to 1 or 2 sites, at most. It is possible that these cases actually represent MIRM. As opposed to SJS, in which medications are a common cause, EM is less associated with medications in adults, as well as in children (17, 19, 21), although Keller et al. (18) found medications, mainly penicillin, to be associated with EM in 46% of cases, especially in children younger than one year of age. It should be noted, again, that the data presented in this latter study should be regarded with caution, as the diagnosis of EM was not confirmed by a dermatologist. In our study, medications were associated with EM in only 16% of cases. The culprit medications were, either β-lactam antibiotics or non-specific anti-inflammatory drugs (NSAIDS), which is in concurrence with the literature (3). Fifteen of the cases (50%) were idiopathic.
It should be noted that we observed a high rate of C-reactive protein (CRP) and/or erythrocyte sedimentation rate in our study. This may be due to an infectious aetiology or the result of the inflammatory nature of EM. Elevated levels of CRP have been described in EM (23), but data regarding CRP levels in children with EM are lacking.
There was recurrence of EM in 16% of our patients. Recurrence is considered very common in HSV-associated EM in adults (1). However, the recurrence rate in children is unknown. The distribution of the rash was in line with the classical description in adults. EM major is usually observed in 25–60% of patients, with mostly oral involvement (3). In our study, 50% of children had some sort of mucosal involvement, mostly oral.
EM was treated relatively aggressively at our medical centre. Seventy percent of the children were hospitalized, for a mean of 3.4 days. One possible explanation for the high rate of admission is that most children with EM who are seen by a primary care physician are not referred to the hospital, and those who are seen at the emergency room are those whose condition is more severe. Another possible explanation is that since the admitting physician in our medical centre is almost always a paediatrician, with less experience than dermatologists in distinguishing EM from SJS/TEN, there may have been a fear of the children having SJS or TEN. In concordance with the literature, it seems that, among paediatricians, there is less awareness of the difference between EM and SJS/TEN (7, 15, 18, 21).
Patients were treated with fluids, anti-virals (despite a lack of evidence for acute HSV infection), antibiotics, topical and systemic steroids and anti-histamines. The prevalent use of systemic corticosteroids (in almost half of the children) is puzzling considering the controversy regarding the utility of steroids in EM and the self-limiting nature of EM (13–15, 21), but is possibly explained by the high percentage of EM major.
This study has several limitations. First, it is a retrospective study resulting in incomplete documentation; in addition, this is a single-centre study, so it is difficult to generalize the conclusions, although our medical centre is tertiary and serves a population of approximately 1.5 million people. Referral bias is a limitation of this study.
This descriptive study sets out the epidemiological, clinical, laboratory and therapeutic characteristics of paediatric EM. This is one of the few epidemiological studies specifically describing characteristics of paediatric EM since the separation of EM from TEN and SJS. It has the advantage of being supervised by a paediatric dermatologist who reviewed all the medical files, while other studies were performed by paediatricians. The most important findings of this study are the lack of EM in infants and toddlers < 4 years and the high rate of misdiagnosis, especially in patients with UM, in this age group. Paediatricians and dermatologists should be aware of the diagnostic criteria for EM and the differential diagnosis from UM. Larger studies in children are required to better characterize paediatric EM.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize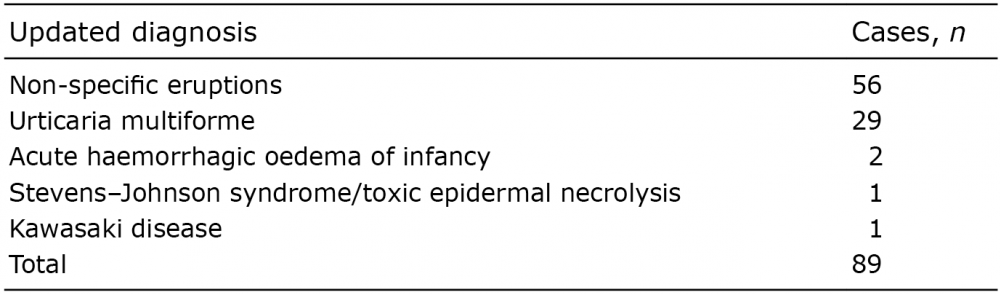 Click to show fullsize
Click to show fullsize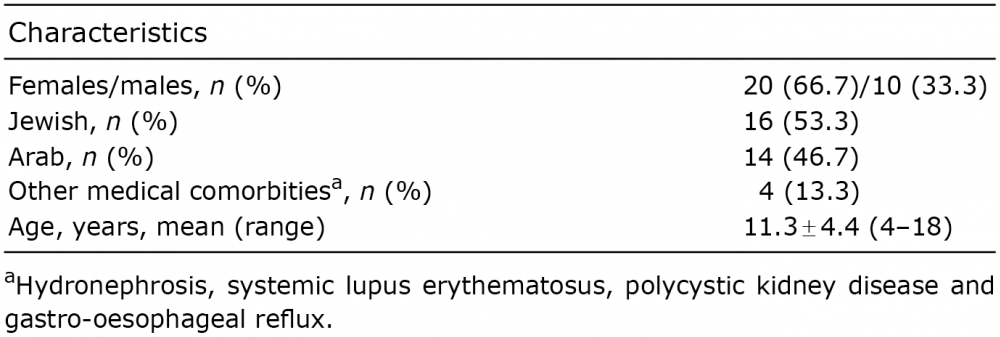 Click to show fullsize
Click to show fullsize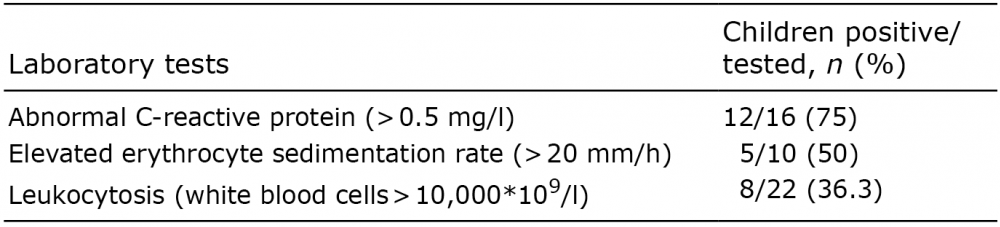 Click to show fullsize
Click to show fullsize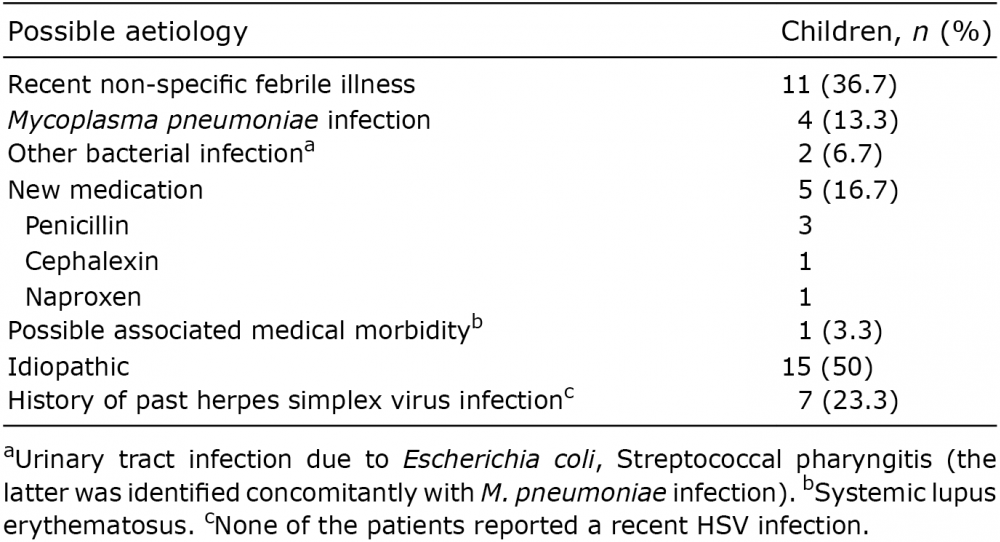 Click to show fullsize
Click to show fullsize