


1Clinical, Allergological and Venereological Dermatology Section, and 2Internal Medicine, Endocrine and Metabolic Sciences Section, Department of Medicine, University of Perugia, Perugia, Italya
Psoriasis can be managed successfully with long-term biologics. Real-life clinical practice may require dose tapering as a therapeutic option to reduce the risk of drug-exposure and to increase cost-effectiveness. The responsiveness to extended intervals between adalimumab doses and the possible predictive factors of maintenance of complete clearance were studied in a retrospective 7-year single-centre analysis. Thirty patients who achieved complete clearance with adalimumab underwent dose tapering, progressively extending between-dose intervals (to 21–28 days). Sixty percent of subjects (group A) maintained complete clearance, whereas 40.0% (group B) relapsed and were switched back to the standard dosage to re-achieve complete clearance. Body mass index (BMI) and time to achieve Psoriasis Area Severity Index (PASI-100) with adalimumab standard treatment before dose tapering were significantly lower in group A than in group B (multi-variate Cox regression: p < 0.05, Kaplan–Meier analysis: p < 0.001, respectively). This study suggests that patients with lower BMI and shorter time to achieve PASI-100 with adalimumab standard dose were significantly more likely to be candidates for dose tapering.
Key words: adalimumab; psoriasis; dose tapering; long-term safety; cost-saving; patient compliance.
Accepted Nov 8, 2016; Epub ahead of print Nov 10, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Luca Stingeni, Clinical, Allergological and Venereological Dermatology Section, Department of Medicine, Azienda ospedaliero-universitaria of Perugia, Santa Maria della Misericordia Hospital, Sant’Andrea delle Fratte, IT-06129 Perugia, Italy. E-mail: luca.stingeni@unipg.it
Psoriasis (PsO) is a chronic immune-mediated inflammatory skin disease affecting approximately 2–3% of the general population worldwide (1) and impairing patient’s quality of life (2). The advent of tumour necrosis factor (TNF)-α inhibitors allows a more targeted and effective approach to the treatment of moderate-to-severe PsO and represents a major breakthrough for patients (3). Among TNF-α inhibitors, adalimumab is a recombinant, fully human, monoclonal antibody approved for the treatment of some chronic immune-mediated inflammatory diseases, including moderate-to-severe plaque PsO in adult and paediatric patients, and psoriatic arthritis (PsA) (4).
The safety and long-term effectiveness of adalimumab in the treatment of PsO were confirmed recently by observational post-marketing studies (5, 6) and real-life experiences (7, 8). Currently, continuous long-term treatment with adalimumab after the achievement of 75/90/100% reduction in the Psoriasis Area and Severity Index (PASI-75/90/100) is recommended (9). However, considering the possible dose-dependent higher risk of malignancies (10), the cost-effectiveness of this treatment (11), and the individual needs (2) of patients treated with biologic drugs, the question is whether patients in stable complete clearance (PASI-100) should be treated at full dosage, a tapered dosage, or whether treatment should be discontinued.
Adalimumab dose tapering, obtained either by increasing the interval between doses or by reducing dosage, was previously and successfully reported in a consistent proportion of patients with rheumatoid arthritis (12, 13), ankylosing spondylitis (14, 15), and with PsA (16). Dose tapering of adalimumab is rarely reported in PsO (17–21), and there is no evidence regarding predictive factors to define the profile of patients suited to this drug-specific therapeutic strategy. Carrascosa et al. (19) reported greater PASI improvement with biologics (adalimumab, etanercept, infliximab, and ustekinumab) in dose-tapered patients.
The primary objective of this retrospective study was to investigate responsiveness to dose tapering obtained with progressive extension of between-dose intervals in patients treated with adalimumab and having sustained complete clearance. The secondary objective was to identify in these patients the predictive factors of maintenance of complete clearance.
An up-to 7-year follow-up observational retrospective study was performed of patients referred to the PsO outpatient clinic within the Dermatology Section of Perugia University, Perugia, Italy, who had been optimally treated with adalimumab between 2008 and 2015. All patients received treatment with adalimumab at an initial dose of subcutaneous 80 mg, followed by a standard dose (40 mg) administered every other week (EOW), starting one week after the initial booster dose. Inclusion criteria were: (i) longstanding moderate-to-severe PsO treated with adalimumab administered EOW at standard dose; (ii) achieved and sustained PASI-100 for one year. Exclusion criteria were: (i) not achieved PASI-100; (ii) achieved but not sustained PASI-100 for one year; (iii) incomplete patient clinical records.
After one year of maintained PASI-100, the between-dose intervals were progressively extended, stepping up 3–4 days each month, up to a 21- or 28-day interval. Patients were evaluated for a minimum period of 4 years up to 7 years. In patients with PsO relapse, defined as a ≥20% loss of PASI improvement, the original schedule was immediately restored. Patients having sustained complete clearance with between-dose intervals of 21 or 28 days were included in group A, whereas those who had to be switched back to EOW administration due to PsO relapse constituted group B. Treatment efficacy was evaluated on a quarterly basis or when PsO relapsed, over a period ranging from 4 to 6 years. Adverse events were recorded at each control visit. Demographic, clinical and anamnestic PsO data, personal comorbidities and familial pathologies were recorded.
The study was carried out in accordance with the principles of the Declaration of Helsinki and all participants gave informed consent.
Statistical analysis was performed using the Mann–Whitney test to compare non-normally distributed continuous variables. Deviations from Gaussian distribution were checked using the Shapiro-Wilk test. Categorical data were analysed with the χ2 test or Fisher’s exact test. The probability of achieving PASI-100 was described with the Kaplan–Meier estimator and compared between treatment groups using a log-rank test. Proportional hazards regression analysis (Cox regression) was fitted for the prediction of relapse after dose tapering, incorporating as covariates all the variables that showed a p-value ≤ 0.25 in bivariate analysis (22). Hazard ratios (HRs) with 95% confidence intervals (95% CI) were also calculated.
All data analyses were performed using IBM-SPSS® version 22.0 (IBM Corp., Armonk, NY, USA, 2013) and a 2-sided p-value < 0.05 was considered significant.
Among the 120 patients treated with adalimumab b-etween 2008 and 2015, 30 (25.0%) patients with moderate-to-severe PsO were included in this retrospective analysis. The remaining 90 patients (75.0%) were excluded because they did not reach PASI-100 (65; 54.2%) or did not sustain PASI-100 for one year (8; 6.7%) or for incomplete records (17; 14.2%). These patients presented baseline PASI value 19.5 (11.0–40.0) and 34 (37.8%) were previously treated with other biologics (etanercept: 32; infliximab: 2), that were stopped for inefficacy or non-maintenance of efficacy.
All the 30 patients enrolled in the study were previously treated with one or more conventional therapies (cyclosporine A: 19, methotrexate: 9; phototherapy: 15), stopped for inefficacy or non-maintenance of efficacy or side-effects. Twelve patients were also previously treated with other TNF-α inhibitors (etanercept: 11; infliximab: 1), stopped for non-maintenance of efficacy.
In our study population 18 patients (60.0%), maintaining complete clearance with a tapered dose (3 patients with 21-day interval and 15 with 28-day interval; mean: 26.8 days, standard deviation (SD) 2.6 days), constituted group A; the remaining 12 (40.0%), needing to be switched back to adalimumab standard dose due to PsO relapse, formed group B. In the latter, the mean time to relapse after dose tapering was 3.8 months (SD 0.9 months) and the mean worsening of PASI during dose tapering was 5.8 (SD 1.3). These patients re-achieved PASI-100 approximately one month after the reintroduction of adalimumab approved dose and maintained PASI-100 during the remaining study period (until December 2015).
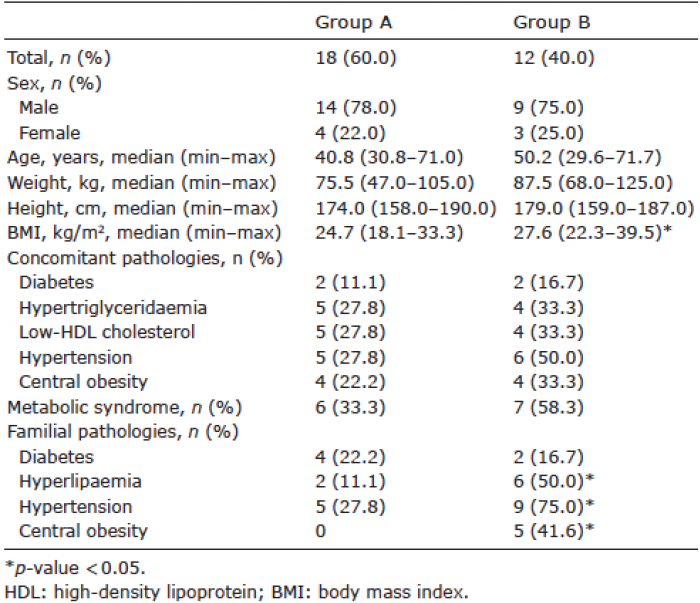
Baseline demographic data, comorbidities and familial pathologies are summarized in Table I. Patients in group A had a significantly lower body mass index (BMI) median value (24.7 vs. 27.6, p < 0.05), lower frequencies of familial hypertension (5/18 (27.8%) vs. 9/12 (75.0%); p < 0.05), familial hyperlipaemia [2/18 (11.1%) vs. 6/12 (50.0%); p < 0.05), and familial obesity (0/18 (0%) vs. 5/12 (41.6%); p < 0.05) than group B patients.
Table I. Baseline demographic data and concomitant and familial pathologies of psoriatic patients maintaining (group A) or losing (group B) complete clearance with dose tapering
PsO clinical data are shown in Table II. Group A patients showed a significant lower frequency of palmo-plantar PsO than those in group B (1/18 (5.6%) vs. 5/12 (41.7%); p < 0.05). Patients with joint involvement (PsA) were 4 in group A (22.0%) and 3 in group B (25.0%); none of the patients showed any clinical or serological PsA relapse, independently from treatment dose.
Table II. Psoriasis clinical data of patients maintaining (group A) and losing (group B) complete clearance with dose tapering
In multivariate Cox regression, which incorporated as explanatory variables those with p-value ≤ 0.25 in bivariate analysis (BMI, hypertension, familial hyperlipaemia, familial hypertension, familial obesity, and palmar/plantar localization), only BMI achieved the status of independent predictor of relapse after dose tapering (HR 1.231, 95% CI 1.008–1.504; p < 0.05).
Kaplan–Meier analysis showed that median time to achieve PASI-100 with adalimumab standard treatment was 3 months (95% CI 2.4–3.6) in group A and 9 months (95% CI 5.6–12.4) in group B; almost 78% and 94% of patients in group A vs. approximately 17% and 42% of patients in group B are likely to achieve PASI 100, at 3 and 9 months, respectively (Fig. 1). In the overall period of observation, these differences were statistically significant (p < 0.001 with log-rank test). There was no correlation between BMI and time to achieve PASI-100. In group B the median time to relapse was 3 months (95% CI 1.9–4.1), indeed 50% of patients relapsed within this time, but all patients in group B relapsed within 7 months from the start of dose tapering. In group A no relapses were observed during the observation period (median 60; minimum 36, maximum 66 months).
Fig. 1. Kaplan–Meier cumulative probability curve for achieving Psoriasis Area Severity Index (PASI-100) by months of standard therapy with adalimumab.
No serious adverse events were observed during the whole study period. None of the patients dropped out because of adverse events.
Dose tapering was performed only when patients achieved PASI-100, as reported in the literature (17, 21), while other authors (18, 20) also decreased the frequency of adalimumab administration when patients achieved PASI-75/90. In our cohort of 30 patients with moderate-to-severe PsO who achieved PASI-100 in response to adalimumab standard dosage, the majority (60.0%) maintained complete clearance. Other authors referred better outcomes with 9.4% of relapsed patients when relapse was undefined (20), and with 20% of relapsed patients when relapse was defined with less stringent criteria (≥ 50% loss of PASI improvement with respect to the score at baseline) (17). We carried out dose tapering by increasing the interval between doses up to 21 or 28 days. The elimination half-life of adalimumab, ranging from 10 to 20 days, does not explain this clinical response. This TNF-α inhibitor exhibits complex pharmacokinetic and pharmacodynamic properties due to its large protein structure and due to the turnover of specific antigenic targets that interact with adalimumab (23). Moreover, the inter-individual pharmacokinetic variability of adalimumab may influence the inter-individual variability of clinical response, not only to standard dose, but also to tapered dose.
Since dose tapering offers relevant advantages in terms of long-term adverse events (10) and cost-effectiveness (11), we emphasize the relevance of possible clinical predictors to identify patients who could benefit from adalimumab dose tapering in order to prevent clinical relapse and to preserve patient’s compliance and quality of life. Regarding adalimumab, dose tapering was recently studied in patients with PsA (16), without clinical differences between patients with full and tapered dosage.
Our results obtained with bivariate analysis show that high BMI, some familial pathologies (hyperlipaemia, hypertension, and obesity) (Table I), and palmo-plantar PsO (Table II) appear to be clinical features predictive of relapse risk in dose-tapered patients. However, in multivariate Cox regression only BMI achieved the status of an independent predictor of relapse after dose tapering: for 1 unit of BMI increase we expect to see approximately 23% of increase in the risk of relapse. This data has never been reported in PsO, nor in rheumatological diseases treated with dose-tapered biologics; moreover, the impact of BMI on the effectiveness of adalimumab standard dose is controversial (24, 25). On the contrary, the difference in frequency of metabolic syndrome (26) between the 2 groups did not reach statistical significance.
Previous conventional and biologic therapies do not seem to influence dose tapering results. Although former therapy with other TNF-α inhibitors (mainly etanercept) was more frequent in group B patients (Table II), this data was not statistically significant.
We also emphasize that in dose-tapered patients who maintained PASI-100, the time to achieve complete clearance with adalimumab at the standard dose was shorter than in group B, as shown by Kaplan–Meier analysis (Fig. 1); furthermore, this clinical feature appeared to be unrelated to the patient’s BMI.
Sustained complete clearance in long-term follow-up (4–6 years) in all patients in our study and short time to re-achieve PASI-100 in group B patients (1 month) exclude the risk of anti-drug antibody due to dose tapering (27). In concordance with previous studies in PsA, our patients with concomitant PsA did not show neither clinical nor serological relapse, independent of treatment dose (16).
This study demonstrates the responsiveness to dose tapering obtained with progressive extension of between-dose intervals in the majority of patients treated with adalimumab. To the best of our knowledge, this is the first study of patients with PsO demonstrating predictive factors for the sustained efficacy of adalimumab in maintaining complete clearance after dose tapering. Due to the small sample size and the retrospective design of the study, our outcomes must be considered with caution. Further prospective investigations are needed to confirm that a lower BMI and a shorter time to achieve PASI-100 with the standard dose are predictors of successful dose tapering with adalimumab.
Dose tapering of adalimumab, obtained either by increasing the interval between doses or by reducing dosage, is rarely reported in PsO. In fact, there is no evidence of predictive factors to define the profile of patients who are suited to increasing the interval between doses of adalimumab. Lower BMI and short time to achieve PASI-100 with the standard dose appear to be predictors of successful dose tapering with adalimumab. This drug-specific therapeutic strategy involves relevant advantages in terms of drug-exposure risk, cost savings, and patient compliance.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize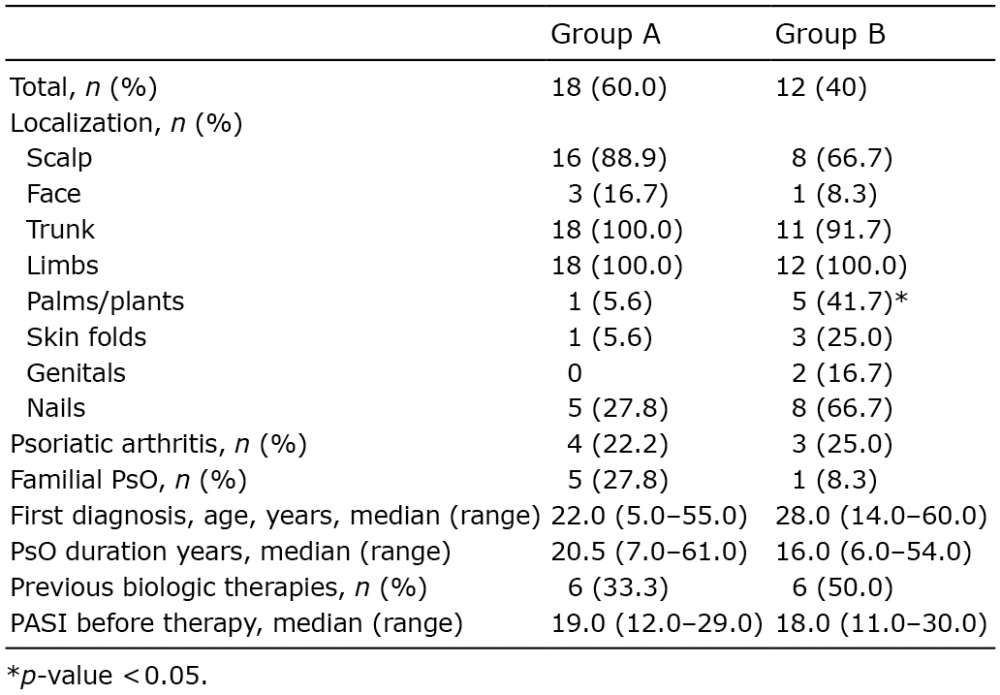 Click to show fullsize
Click to show fullsize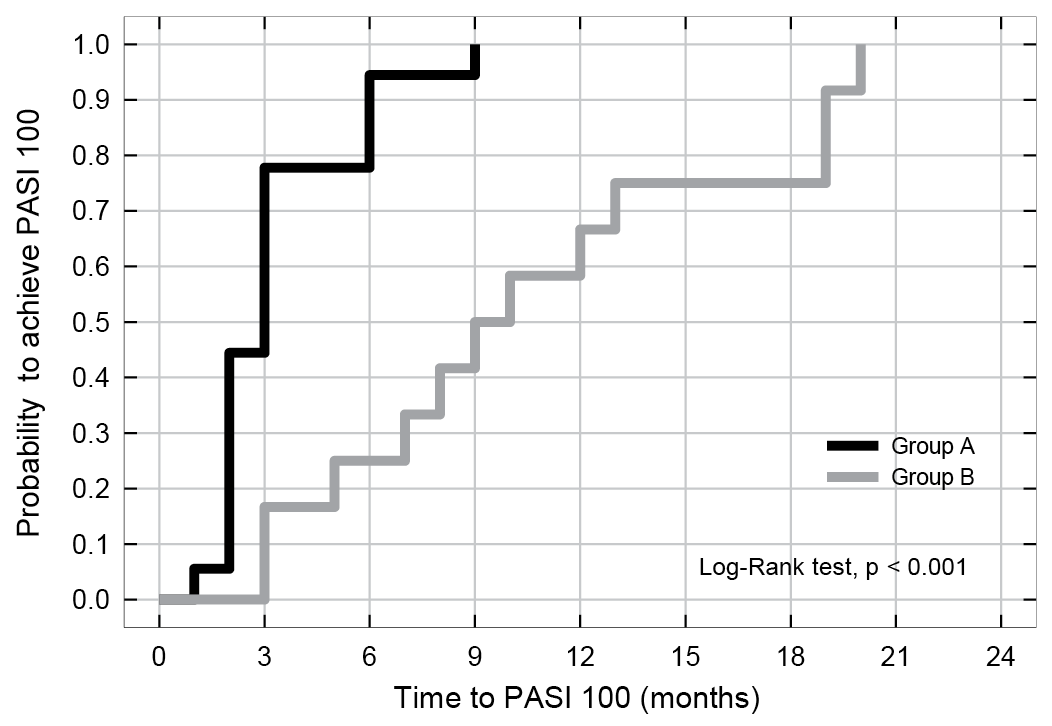 Click to show fullsize
Click to show fullsize