


1Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Josef-Schneider-Straße 2, DE-97080 Würzburg, and 2Institute of Pathology and Comprehensive Cancer Center Mainfranken, University Würzburg, Würzberg, Germany. *E-mail: Wobser_M@ukw.de
Accepted Nov 10, 2016; Epub ahead of print Nov 14, 2016
Primary cutaneous T-cell lymphomas (CTCL) comprise a heterogeneous group of extranodal non-Hodgkin’s lymphomas. The most common subtype is mycosis fungoides (MF), characterized by a superficial epidermotropic infiltration of neoplastic CD3+ T cells (1). In the early stages of MF, the disease commonly presents with almost unrestricted life expectancy, whereas advanced-stage MF usually runs a more aggressive course (2). Immunohistochemical labelling of CD20 is widely used for detection of cells of the B-cell lineage (3, 4). Reactive B-cell infiltrates have been sporadically described in CTCL (5). Moreover, aberrant expression of CD20 on neoplastic T cells has been described in rare cases (6). Based on 2 patients diagnosed with CD8+CD20+ CTCL this report provides additional insight into potential diagnostic pitfalls and discusses the putative prognostic and diagnostic value of CD20+ cells in CTCL.
Patient 1. A 63-year-old man presented with macules and plaques on the upper back and the groin (Fig. 1 a, b). Biopsies revealed a dense lymphoid infiltrate with extensive epidermotropism (Fig. 1c). Further immunohistochemical staining showed a T-cell rich infiltrate with positivity for CD3 and CD5 and antigen loss of CD2. There was prevailing expression of CD8 (Fig. 1d) over CD4 and both T-cell receptor (TCR) chains β and γ were consistently positive (dual TCR expression).
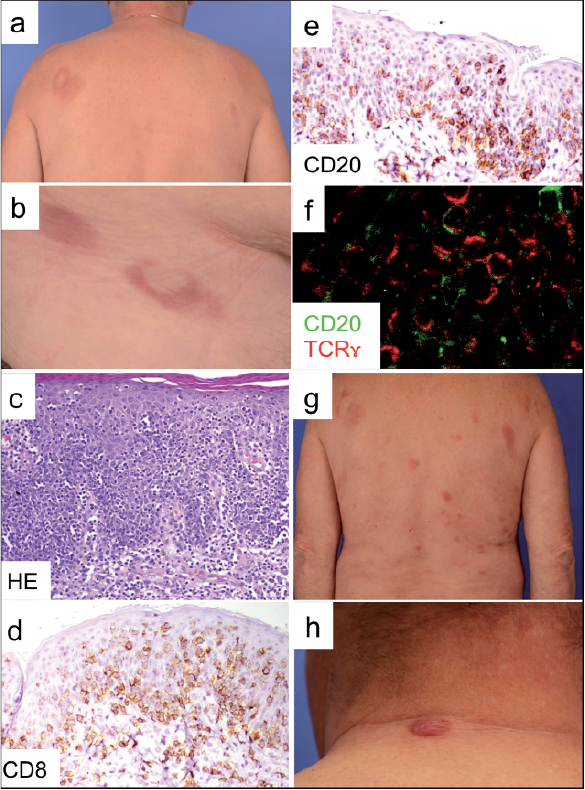
Fig. 1. Patient 1 at initial presentation with sharply defined annular, erythematous, non-scaling macules and plaques on (a) the upper back and (b) the groin. (c) Histology showing a dense, atypical lymphoid infiltrate with striking epidermotropism (haematoxylin & eosin, magnification 200×). The lymphocytes are small-to-medium-sized with atypical cytological features exhibiting irregular nuclear contours, hyperchromasia and a coarse chromatin pattern. Immunohistochemical studies demonstrate (d) CD8+ and (e) CD20+ expression of the atypical lymphocytes (magnification 400×). (f) Immunofluorescence double-staining confirms the aberrant expression of CD20+ in a significant proportion of the T-cell receptor (TCRγ+) infiltrate. Patient 1 at time of progressive disease exhibiting (g) multiple new non-ulcerated plaques and (h) a small tumour on the back of the neck.
CD56 was strongly positive within CD8+ T cells. CD30 was negative. Further immunohistochemical work-up of the atypical lymphoid infiltrate revealed strong CD20 expression (Fig. 1e). B-cell markers, such as CD79a and PAX-5, tagged only a few reactive dermal B cells. Additionally conducted double immunolabelling confirmed the aberrant expression of CD20 in a significant proportion of the TCRβ+ and TCRγ+ infiltrate (Fig. 1f). Molecular genetic characterization, based on PCR amplification of the TCRγ chain gene, demonstrated an identical clone in all samples.
Hence, diagnosis was made of an epidermotropic and phenotypically unusual CTCL with aberrant co-expression of CD20 by the neoplastic T cells. The clinical features, together with the aberrant phenotype (CD8+, CD56+, CD20+, TCRβ/γ+), led to a final diagnosis of peripheral T-cell lymphoma, not otherwise specified.
Full blood count, lactate dehydrogenase (LDH), computed tomography (CT) scan of the chest, abdomen and pelvis, and bone marrow examination, were unremarkable. After preliminary partial remission under topical steroids, the patient showed progressive disease with multiple plaques and small tumors after 2 months (Fig. 1 g, h). Repeated histological examination of new or progressive lesions invariably revealed the same epidermotropic infiltrate of CD8+, CD20+, TCRβ+, TCRγ+ neoplastic T cells with tracking of the identical clone on sequential biopsies. Methotrexate (20 mg/week) was initiated, but due to a significant further cutaneous progress, was substituted by gemcitabine 600–900 mg/m2 body surface every 2 weeks producing disease stabilization.
Patient 2. A 78-year-old man presented with a 20-year history of patches and plaques on the trunk, extremities and face (Fig. S1a). His skin lesions had previously been diagnosed as psoriasis and had been well-controlled with topical corticosteroids. In the last few weeks, however, a rapidly growing tumour had occurred on a previously persistent plaque on his left nose slope (Fig. S1b).
Biopsies of the lesions on the patient’s trunk were consistent with CD4+ CD20-MF. Histopathological examination of the tumour on the nose revealed a dense atypical, highly proliferative lymphoid infiltrate with epidermo- and slight folliculotropism (Fig. S1c). Immunohistochemistry revealed a double-positive CD4+, CD8+ T-cell phenotype (Fig. S1d, e) with dual TCR-positivity. CD56 remained negative. Staining for PAX5 and CD79a showed few, loosely intermingled reactive B cells. CD20 was co-expressed by a significant portion of the atypical T-cell infiltrate, albeit the staining pattern of neoplastic T cells for CD20 was found to be at lower intensity than that of the intermingled true CD20+ B-cells (Fig. S1f). CD30 marked only sporadically and presumably reactive inflammatory lymphocytes. Genotyping showed a monoclonal rearrangement of the TCRγ chain gene in all biopsies.
Clinically and histologically the patches and plaques on the trunk and extremities were classified as CD4+ CD20- MF. The rapidly growing tumour on the nose slope with CD8+ CD20+ neoplastic T cells showed histologically and phenotypically divergent, but clonally identical, atypical lymphoma infiltrates. Therefore, the most likely diagnosis is that of a sequentially transformed or phenotypically aberrant MF.
Under fractionated localized radiotherapy the tumour on the nose underwent rapid regression. Full blood count, LDH, CT scan and bone marrow examination were unremarkable. After exclusion of contraindications, treatment with methotrexate (15 mg/week) was initialized, leading to significant improvement in skin lesions. The patient is currently alive with residual disease.
Most CTCLs have a mature post-thymic CD3+ CD4+ immunophenotype (6). Nevertheless, deviant variations of distinct phenotypes have been reported with an uncertainty of prognostic value and there is a growing number of reports describing T-cell lymphomas and leukaemias with aberrant CD20 expression (7, 8). These T-cell lymphomas may derive from the CD20+ subset of a non-neoplastic T-cell population in peripheral blood (9, 10). The finding that many of the reported cases of CD20+ T-cell lymphoma have a CD8+ immunophenotype supports this theory (9). Another hypothesis suggests that deviant antigen expression can be regarded as a marker of activation, or that acquisition of CD20 expression occurs during malignant transformation (9, 11). In support of this hypothesis, CD20 expression has been observed to be inducible in monkey lymph node T cells upon stimulation with mitogen, IL-2 and simian immunodeficiency virus (11). Moreover, a study by Theurich et al. (12) revealed that there is a significant correlation of CD20 expression with advanced stages of CTCL. Lastly, it may be that CD20 expression has no biological or clinical significance and simply reflects aberrant expression by the tumour population in the sense of clonal evolution (6).
Patient 2 in our study presented with CD20+ neoplastic cells in the tumour, while lymphocytes in the remaining cutaneous infiltrates lacked CD20 expression despite a common clonal origin. Our observation supports the hypothesis of both a variable activation state and a putatively higher aggressive potential of the neoplastic cells within the tumour manifestation.
As has been suggested in previous reports of CD20+ CTCL, this subpopulation of neoplastic cells might be amenable to targeting by therapeutic anti-CD20 monoclonal antibodies, such as rituximab (13). Since rituximab has a low toxicity profile, its use would be of particular interest in patients with CD20+ CTCL, who are often older and present with significant comorbidities. In particular, in combination with conventional chemo-immunotherapy this treatment could add efficacy. To date, however only a few cases of CD20+ CTCL have been treated with rituximab, with variable outcomes (7, 9) and we refrained from using this rather experimental approach.
Lastly, prospective studies with larger patient numbers, as recently published by Toya et al. (14), are warranted to determine whether positivity for CD20 could serve as a prognostic marker and might be therapeutically exploited in CD20+ CTCL.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize