


1Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 2Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Nanjing, China, 3Department of Pathology, University of Mississippi Medical Center, Jackson, USA, 4Shanghai Key Laboratory of Tuberculosis, Shanghai Pulmonary Hospital, Medical School, Tongji University, Shanghai, and 5State Key Laboratory for Infectious Disease Prevention and Control, National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China
Cutaneous tuberculosis (CTB) is probably underreported due to difficulties in detection and diagnosis. To address this issue, genotypes of Mycobacterium tuberculosis strains isolated from 30 patients with CTB were mapped at multiple loci, namely, RD105 deletions, spacer oligonucleotides, and Mycobacterial Interspersed Repetitive Unit-Variable Number Tandem Repeats (MIRU-VNTRs). Fifty-eight strains of pulmonary tuberculosis (PTB) were mapped as experimental controls. Drug resistance-associated gene mutations were determined by amplicon sequencing of target regions within 7 genes. Beijing family isolates were the most prevalent strains in CTB and PTB. MIRU-VNTR typing separated the Beijing strains from the non-Beijing strains, and the majority of CTB could be separated from PTB counterparts. Drug resistance determining regions showed only one CTB strain expressing isomazid resistance. Thus, while the CTB strains belonged to the same phylogenetic lineages and sub-lineages as the PTB strains, they differed at the level of several MIRU-VNTRs and in the proportion of drug resistance.
Key words: tuberculosis; cutaneous; spoligotyping; MIRU-VNTR; RD deletion, drug resistance.
Accepted Nov 10, 2016; Epub ahead of print Nov 14, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Hongsheng Wang and Weida Liu, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12 Jiangwangmiao Road, Nanjing 210042, China. E-mail: whs33@vip.sina.com and wanghs@ncstdlc.org
Tuberculosis (TB) is a major public health problem worldwide, especially in China. Extrapulmonary TB (EPTB) is well known in the history and literature of TB; however, there are few reports on the genetic, biochemical and drug sensitivity properties of EPTB (1–3). Cutaneous TB (CTB) is a difficult to diagnose form of EPTB. One report estimated that CTB comprises approximately 1–2% of all clinical forms of TB (4, 5). Over the past 2–3 decades, CTB has been diagnosed and treated successfully at the Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, China, and strains have been cultured from skin specimens (6). The identification of CTB cases in a background of known high levels of pulmonary TB (PTB) and multidrug-resistant TB (MDR-TB) in mainland China prompted us to further characterize these archived CTB along with additional isolates derived from subsequently diagnosed cases.
Recent developments have led to rapid detection of Mycobacterium tuberculosis DNA or RNA in clinical specimens by in vitro nucleic acid amplification, enabling investigations into epidemiology, transmission and PTB outbreaks (7). IS6110-based restriction fragment length polymorphism (RFLP) has been the gold standard in genotyping for more than a decade, but this technique is laborious and expensive, and requires a large amount of chromosomal DNA (8). Spoligotyping is based on polymorphisms of the chromosomal direct repeat (DR) locus, which contains a variable number of short DRs interspersed with non-repetitive spacers (9). This method is commonly used to differentiate M. tuberculosis complex strains. Mycobacterial Interspersed Repetitive Unit-Variable Number Tandem Repeat (MIRU-VNTR) analysis (10, 11) is a rapid and simple genotyping method with a discriminatory power similar to that of RFLP (12). MIRU-VNTR has been proposed by an international consortium as a standardized genotyping scheme, with 15- and 24-loci sets demonstrated to have adequate discriminatory power for tracing transmission and investigating the phylogenetics of TB (13). Other markers, including single-nucleotide polymorphisms (SNPs) and deletions at regions of difference (RD) loci, identify deeper phylogenetic origins and their branches. Whole-genome sequencing, an emerging highly discriminatory, sensitive and affordable methodology, is yet to be universally adopted in clinics and research centres; therefore comparison of genotypes using a uniform set of markers is limited. At strain level, MIRU-VNTRs with their higher rates of change than RD and DR deletion markers, aid in breaking larger phylogenetic clusters, enabling discrimination levels suitable for tracing recent transmission links.
The Beijing family, a dominant M. tuberculosis genotype, which belongs to Lineage 2, is detected in PTB strains in China and the rest of Asia, and exhibits important pathogenic features that may be associated with drug-resistant TB (14). The lack of spacers 1–34 in the DR loci is 1 of the characteristics to generate the spoligotype (a polymorphism in the repeat units of DNA) S00034 that defines the Beijing type (15). Several large-sequence polymorphisms (e.g. RD105, RD142, RD150, and RD181) were used to further divide this family into monophyletic subgroups. RD105 deletion is observed specifically in all Lineage 2 strains and also serves as a useful biomarker for identifying Beijing family strains (16). However, not all strains deleted for RD105 are Beijing type and, on the other hand, not all strains with S00034 spoligotype are of Beijing type due to the possibility of homoplasy at the DR locus. Thus, several markers should be tested to ascertain phylogeny and Beijing family status.
The current first-line drug regimen consists of rifampicin (RIF), isoniazid (INH), pyrazinamide (PZA), ethambutol (EMB), and streptomycin (STR). Resistance to first-line anti-TB drugs is closely related to mutations in at least 7 genes: katG and inhA for INH resistance; rpoB for RIF resistance; embB for EMB resistance; pncA for PZA resistance; and rpsL and rrs for STR resistance.
Although CTB has been reported continuously during recent decades (17, 18), the molecular epidemiology of CTB has not been investigated. Moreover, little is known about the relationship among strains isolated from CTB with other EPTB and/or PTB, as well as their interactions in the transmission dynamics of these 2 diseases.
The aims of this study were therefore to define the genotypes of strains using several established universal molecular markers for TB phylogeny and strain typing, and to assess drug resistance associated with first-line drugs for TB in a panel of 30 CTB isolates through molecular screens. As a further aim, the genotypes were compared against a panel of published regional, national and global PTB genotypes to reveal any patterns unique to CTB.
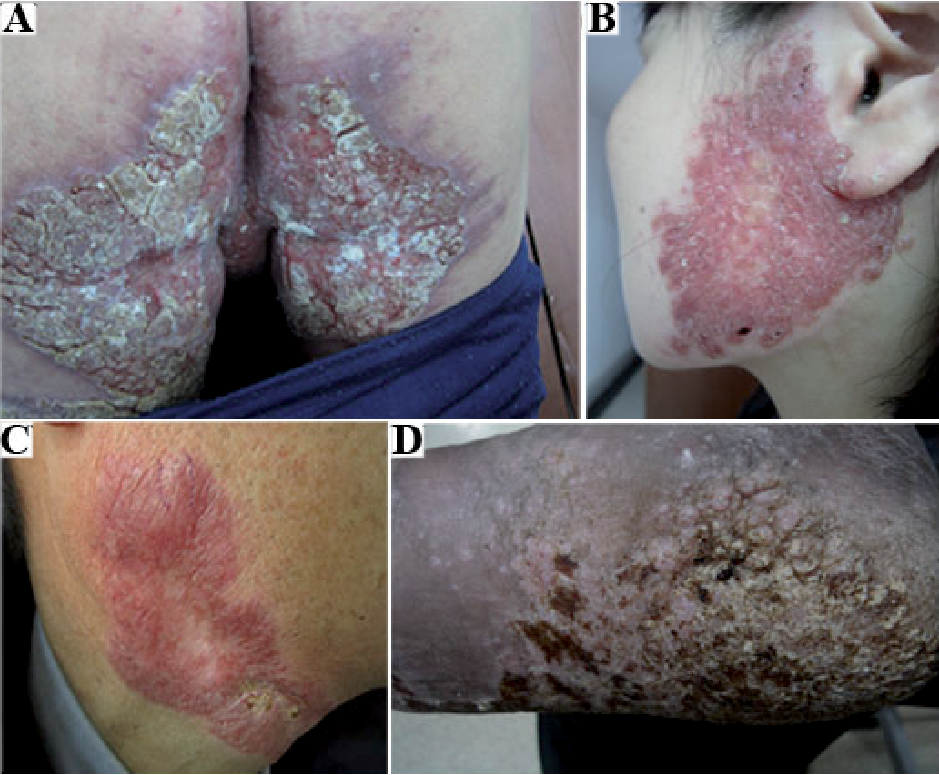
Thirty patients with CTB who presented at the Hospital of Dermatology, Chinese Academy of Medical Sciences during the study period were enrolled; 15 from Jiangsu and others from neighbouring Anhui province (Table SI). No significant differences in age, sex, and birthplace (urban or rural) were detected between the 2 groups. No lung abnormalities were seen on the enrolled patients’ chest X-rays. The spectrum of the cutaneous infections included 4 cases (13.3%) of TB ulcerosa cutis (Fig. 1A), 16 (53.3%) of lupus vulgaris (Fig. 1B), 2 (6.7%) of scrofuloderma (Fig. 1C), and 8 (26.7%) of TB verrucosa cutis (Fig. 1D). Lupus vulgaris constituted the majority of CTB in both provinces. The results of purified protein derivative (PPD) analysis were positive (induration >10 mm) in 28 of 30 cases. Ziehl–Neelsen staining for bacilli in the skin tissue samples showed positive results in 15 cases. On L-J medium, however, all 30 tissue cultures from the lesions grew brown and granular colonies at 32°C and 37°C after 1–2 months, with 37°C being the preferred growth temperature (see Table SI). Sequence analysis of PCR amplification products of hsp65 and 16S rRNA genes from DNA samples of CTB and PTB strains showed 100% similarity with M. tuberculosis genes.
Fig. 1. Cutaneous tuberculosis. (A) Ulcerosa cutis: painful, mutilating, perianal ulceration with large erosion in a 45-year-old man. (B) Lupus vulgaris: large, erythematous, infiltrated patch with scaling on the right cheek and ear of a 36-year-old woman. (C) Scrofuloderma: irregular, deep-seated nodes and ulcers in a serpiginous shape on the lateral neck of a 37-year-old man. (D) Verrucosa cutis: crusted and hyperkeratotic plaque on the heel of a 53-year-old man.
Among the 30 CTB strains, 22 (73.3%) had RD105 deletion (Fig. S1A and B). They include all 4 cases (100%) of TB ulcerosa cutis, 13 (81.3%) of lupus vulgaris, and 5 (62.5%) of TB verrucosa cutis. Two cases of scrofuloderma (100%) were caused by non-Lineage 2 strains. Among the 58 PTB strains representing both Jiangsu and non-Jiangsu patients who were genotyped by the same set of markers, 45 (77.6%) isolates lacked RD105, and the remainder (22.4%) belonged to the non-Lineage 2 strains (Fig. S1C–F).
Among the 30 CTB strains, 29 (96.7%) were successfully assigned to 5 known spoligotypes (STs), but one strain (3.3%) was undefined by referring to the SpolDB4.0 database. The predominant STs were the Beijing and Beijing-like genotype (n = 21, 70%), T1 (n = 4, 13.3%), and U (n = 2, 6.7%), thereby representing approximately 90% of the total strains (Table SII). The 58 PTB strains yielded 7 distinct STs. Among them, 2 strains (3.4%) which have identical spoligotype were undefined, whereas 56 (96.6%) were successfully clustered by spoligotyping into 6 types. The predominant STs were the Beijing genotype (n = 45, 77.6%), which completely coincided with the RD105 deletion analysis results (i.e. all 45 had RD105 deletion).
In CTB strains, the Beijing and Beijing-like family comprised 4 cases (100%) of TB ulcerosa cutis, 12 (75%) of lupus vulgaris, and 5 (62.5%) of TB verrucosa cutis. Two cases of scrofuloderma (100%) were caused by non-Beijing family strains (p < 0.01).
A high discriminatory power was obtained by MIRU-VNTR. A total of 88 distinct MIRU-VNTR genotypes were observed, i.e. no 2 isolates shared the same genotype (Fig. S2). With the multidimensional scaling method in R program, all the strains could be divided into 2 large groups: Beijing and non-Beijing genotypes (p < 0.01), and the Beijing genotyping group could be further divided into CTB and PTB subgroups (p < 0.01) (Fig. S3).
HGDI calculated for each MIRU-VNTR locus, varied significantly, from 0.895 for QUB11b to 0 for MIRU2. MIRU26, MTUB21, QUB26 and QUB11b were highly discriminatory, both for CTB and PTB strains, and the HGDI for loci in CTB were higher than for PTB (p < 0.05). Two loci ETRC and MIRU20 were significantly more discriminatory in CTB than in PTB (p < <0.01) (Table SIII).
Screening for drug resistance causing mutations was conducted on all 30 CTB strains. One strain (C1) carried a mutation in katG (Ser 315 Thr), which is responsible for INH resistance and the phenotype was subsequently verified by in vitro drug susceptibility testing. The other isolates did not present any mutations in rpoB, katG, inhA, embB, pncA, rpsL and rrs genes known to be associated with RIF, INH, EMB, PZA and STR resistance. On the other hand, the control sample set of 58 PTB DNAs, showed that 26 (44.8%) strains, which included 84.6% Beijing, 11.5% T1 and 3.8% T2 genotypes, were resistant to at least 1 drug. There were 10 strains (17.2%), 9 Beijing and 1 T1 that were of MDR type, resistant to at least INH (Ser 315 Thr in KatG) and RIF (Ser 531 Leu in RpoB), the 2 most powerful anti-TB drugs (33). The proportion of MDR-TB in the Beijing vs. non-Beijing genotype PTB strains was statistically different (p < 0.02). The overall molecular results are summarized in Table I.
Table I. Summary of molecular characteristics of Mycobacterium tuberculosis isolated from 30 cases of cutaneous tuberculosis (CTB)
CTB is a prevalent form of EPTB that involves morbidities, diagnostic and therapeutic problems for patients presenting in dermatology clinics and for their physicians in developing countries, including China. Some cases of drug-resistant CTB have been reported in a previous study (34).
Molecular characterization of multiple types of genetic markers (RD105, direct repeats and MIRU VNTRs) has determined that the dominant CTB strain in China is of the Beijing family type, which is also the genetic background of the majority of PTB strains in China. The molecular characteristics of PTB and EPTB are compared and discussed in detail in Appendix S2 (35–48). Although many of the CTB and PTB strains share a phylogenetic lineage and spoligotype family, they can be segregated as sub-populations by MIRU-VNTR markers. The PTB Beijing strains were more similar to each other than to the CTBs, with unbiased heterozygosity of 0.31 compared with 0.532, even though there were no epidemiological criteria applied in assembling the collection. This overall molecular separation could reflect divergent sources of infection, disease progression and transmission mechanisms. Continued detection of CTB and isolation of pure cultures for genotyping would enable further elucidation of their relationship with endemic PTB strains.
PTB, although treatable, remains a public health challenge due to primary and acquired drug resistance. The Beijing family of M. tuberculosis has been associated with resistance in China and other parts of the world to which it has spread. In this connection, it was important to screen the CTB strains for drug resistance using molecular tests. A nucleotide substitution in the drug resistance determining regions (DRDR) was detected in katG in 1 strain (C1) isolated from a CTB patient with lupus vulgaris, with phenotypically confirmed resistance to INH. The strain belonged to the non-Beijing family and possessed a unique 24-loci MIRU-VNTR genotype. Whether resistance to INH is innate or a consequence of medication remains unclear. On the other hand, a much higher proportion of the 58 PTBs tested carried mutations associated with resistance to at least one drug (n = 26); 10 were MDR-TB strains, resistant to the 2 most powerful anti-TB drugs, INH and RIF. Lack of mutations that confer drug resistance to TB standard treatment is good news for the treatment and control of CTB in China in the provinces sampled. It also indicates that the Beijing type per se is not associated with drug resistance (49), as > 70% of CTB were of Beijing type deleted at both RD105 or deleted at DR 1-34. These are promising findings, suggesting that, if properly diagnosed, CTB, including those of Beijing type can be treated with current regimens and controlled. Furthermore, the data indirectly imply that CTB infections are not derived from or recently related to the prevalent pool of PTB strains, a sizeable portion of which are drug resistant.
Comparison of the molecular epidemiology of CTB with that of other EPTBs would be a challenge, not only due to the paucity of such research, but also due to differences in methodologies, objectives, results and insufficient clinical/sample details, even when reports are available. Nevertheless, some common and distinctive observations can be made based on recent genotyping studies on EPTB in different countries. For example, in Russia, a study of spinal TB (TBS) found that 75% of strains were of the Beijing type, a proportion greater than that of the national prevalence of pure PTBs (50). Moreover, 95% of these Beijing TBS were multidrug resistant, bearing mutations katG315 and rpoB531 commonly found in PTBs. Furthermore, despite patients originating from different regions of the country, genotyping with a 24-locus MIRU-VNTR panel showed clustering. Therefore the infection, transmission and drug resistance mechanisms of TBS in Russia may overlap with those of recent PTB, while such trends were not seen with CTB in China.
In a collection of 67 EPTB strains cultured from a variety of anatomical sites and sample types from patients in Puducherry and neighbouring districts, in South India, spoligotyping showed that EA1 lineage predominated, followed by orphan and Beijing types. EA1 is more frequent in South India than in the North where CAS predominates (35). Thus EPTB in South India reflected those of local PTB strains, although there were no matches for the majority of spoligotypes to the SITVIT database2. This could indicate lack of clustering among the EPTB. Dual-drug resistance was detected in 2 isolates and single-drug resistance in 15 isolates; these were not associated with any particular lineage in this study. Some other studies (51–53) show that EPTB were generally of the same clade(s) as regional PTBs. Moreover, clustering and drug resistance were detectable at variable levels, unlike the CTB in China, which did not cluster at the level of MIRU-VNTRs and were drug sensitive.
In conclusion, this first worldwide exploration of the molecular characteristics of CTB shows that they are predominantly of Beijing family type. These analyses reveal that, while the CTB strains belong to the same phylogenetic lineages and sublineages as the PTB strains, they differ at the level of several MIRU-VNTRs and in the proportion of drug resistance. Continued surveillance for CTB and early diagnosis alongside the collection of skin specimens and culture isolation of the pathogen, molecular genotyping and DRDR screening, as in this study, would further our understanding of the origin of this EPTB and assist in controlling its spread and the emergence of drug resistance (Table I).
The authors would like to thank the study participants and their caregivers.
Funding. This work was supported by the National Natural Science Foundation of China (grants 81371751), Jiangsu Provincial Special Program of Medical Science (grants BL2012003), and the 12th Five-Year Infectious disease research project (grants 2012ZX10001-003).
The authors declare no conflicts of interest.
2SITVIT is composed of spoligotype international types (SIT) and VNTR International Types (VIT). It is a publicly available international database for Mycobacterium tuberculosis. It contains two major types of molecular markers: Spoligotypes and VNTR-MIRU markers.
 Appendix S1 Appendix S2 Figure S1 Figure S2 Figure S3 Table SI Table SII Table SIII
Appendix S1 Appendix S2 Figure S1 Figure S2 Figure S3 Table SI Table SII Table SIII

 Click to show fullsize
Click to show fullsize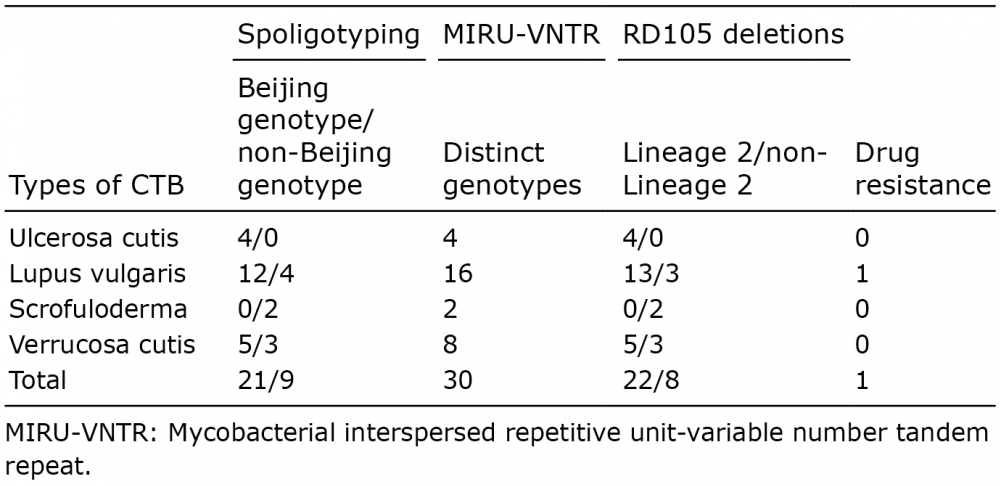 Click to show fullsize
Click to show fullsize