


Department of Dermatology, Eulji University Hospital, 95, Dunsanseo-ro, Seo-gu, Daejeon 35233, Korea. E-mail: gentleship@eulji.ac.kr
A 43-year-old woman presented with erythematous grouped confluent papules on a plaque on her right shoulder (Fig. 1). The lesion had been present for 2 months and had progressively increased in size, with a grapefruit shape. The patient had a 6-month history of repeated intra-articular injections of triamcinolone acetonide on her right shoulder for controlling pain due to impingement syndrome. She was otherwise healthy and examination did not reveal lymph-adenopathy or any other cutaneous lesions. Laboratory analyses performed to exclude systemic diseases, such as leukaemia, were negative, including the result of acid-fast bacilli (AFB) stain and tuberculosis (TB) PCR. Histological findings showed a dense, dermal infiltrate of histiocytes with scattered lymphocytes, plasma cells, and neutrophils (Fig. 2). By immunohistochemical analysis, the histiocytes were positive for S-100 protein and CD68, but negative for CD1a (results not shown). The patient was treated with intra-lesional steroid injection therapy once a month and her skin lesions have been gradually improving.
Fig. 1. Erythematous grouped confluent papules in a plaque on the right shoulder.
Fig. 2. A dense, dermal infiltrate of histiocytes forming emperipolesis (arrow) (haematoxylin and eosin; original magnification ×400).
What is your diagnosis?
Rosai-Dorfmann disease (RDD) is a self-limited benign disease characterized by massive painless lymphadenopathy, anaemia, fever, raised erythrocyte sedimentation rate, leukocytosis and hypergammaglobulinaemia. The differential diagnosis of RDD is similar to other causes of lymphadenopathy. Non-malignant aetiologies include tuberculosis, Wegener granulomatosis, sarcoidosis, IgG4-related disease, Erdheim–Chester disease, Gaucher disease, and other histiocytic disorders, such as Langerhans cell histiocytosis. Malignant aetiologies included Hodgkin’s lymphoma, non-Hodgkin’s lymphoma, melanoma, leukaemia, and Langerhans cell sarcoma (1). RDD with extranodal involvement occurred in approximately 40% of cases, skin involvement occurred in most cases (2). However, cutaneous RDD without lymph node involvement is very rare, and only a few cases have been reported. In pure cutaneous RDD, systemic symptoms or laboratory abnormalities may not be seen, unlike in systemic RDD. In order to diagnose cutaneous RDD histopathological examination is required (see Fig. 2). The histiocytes have large vesicular nuclei, tiny nucleoli, and eosinophilic cytoplasm with feathery borders. Specifically, emperipolesis was found, i.e. large histiocytes that have intact lymphocytes inside and are strongly reactive for S-100 protein. The histiocytes are positive for CD68, but negative for CD1a (3).
RDD has good prognosis when the disease is limited to the skin. Spontaneous regression and recovery often occur over a period of months to years (4). The aetiology of the disease is unknown. In the case described here, the patient had a definite history of intra-articular injection at the eruption site, which has not previously been reported as a cause of cutaneous RDD.


 Click to show fullsize
Click to show fullsize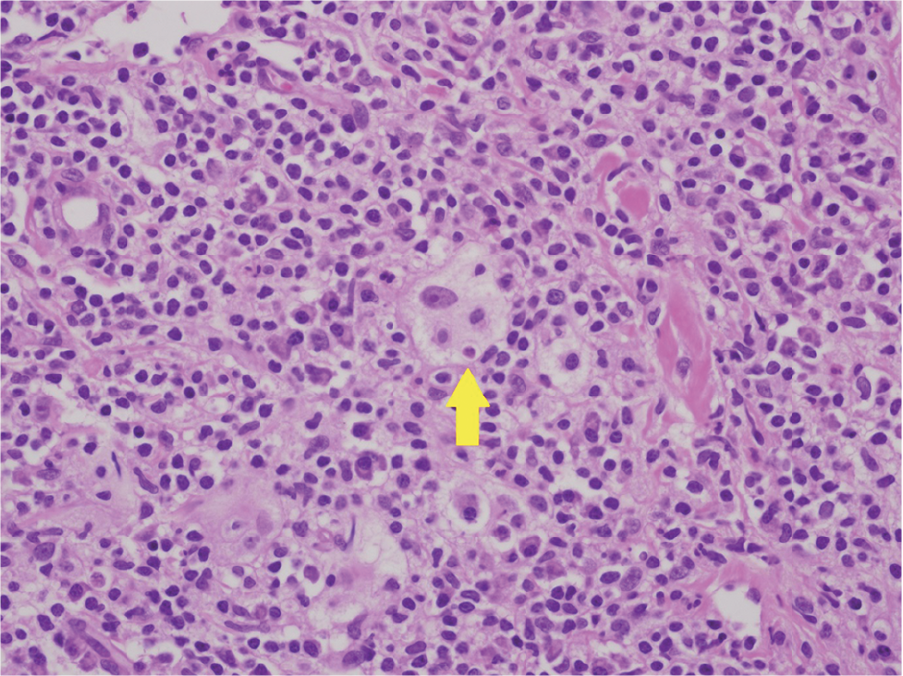 Click to show fullsize
Click to show fullsize