


Lower vitamin D serum levels are linked to increased melanoma risk and poorer survival. Naevus counts are associated with both melanoma risk and survival and to leucocyte telomere length. Vitamin D is also linked to telomere biology with higher levels of vitamin D in individuals with longer leucocyte telomere length despite adjusting for age. Using the TwinsUK data, we explored the association between naevus count, leucocyte telomere length and vitamin D serum levels. Increasing vitamin D levels were associated with increasing naevus count: serum levels were 73.3 nmol/l in individuals with less than 50 naevi compared to 78.8 nmol/l in individuals with more than 50 naevi (p = 0.002). In the final regression model, using naevus count as a continuous variable, vitamin D remained associated with higher naevus counts despite adjustment for age, weight, height, season of sampling and twin relatedness (p = 0.02). Further adjustment for leucocyte telomere length, decreased the magnitude of the association but it remained significant so leucocyte telomere length is not the sole driver of this association. Having large numbers of naevi is associated with higher vitamin D serum levels.
Key words: vitamin D; melanoma; naevus count; 25(OH)D.
Accepted Nov 17, 2016; Epub ahead of print Nov 21, 2016
Acta Derm Venereol
Corr: Simone Ribero, MD, PhD, Department of Twin Research and Genetic Epidemiology, King’s College London, St Thomas’ campus, Westminster Bridge Road, London, SE1 7EH, UK. E-mail: simone.ribero@unito.it
Higher vitamin D (25(OH)D) levels have been shown to protect from melanoma and furthermore from melanoma recurrence (1). It is unclear whether 25(OH)D serum levels are protective per se, or, are a proxy marker for other protective factors in melanoma (2). It is possible that higher 25(OH)D is a reflection of healthier lifestyle which in turns confer some protection against cancer in general (3).
Twin studies have shown that naevus number is an heritable trait (4) and genome-wide association studies for melanoma and naevus counts have identified many SNPs explaining the genetic variation associated both with naevi number and melanoma risk (5–7). Naevus counts decrease with age. High naevus counts are also associated with longer leucocyte telomere length (LTL) despite adjusting for age which suggests that naevi number and size and senescence are linked (8).
Mounting evidence suggests that, in addition to its well described roles in skin, bone, and muscle physiology (9), 25(OH)D acts as an inhibitor of the inflammatory response through several pathways. The inhibitory effect of vitamin D on the inflammatory response (10) also leads to a potential link between this vitamin and LTL biology (11), suggesting a potential role of 25(OH)D in senescence (12). The relationship between vitamin D and melanoma is quite complex as many possible confounders may affect the significance of the association. It has been shown that both melanoma risk and melanoma recurrence may be increased in those with low vitamin D (13–15). The aim of this study was to look at the associations between number of naevi (the strongest melanoma risk factor) and 25(OH)D serum levels.
Ethics Committee approval for this study was obtained from the Guy’s and St Thomas Hospital NHS Trust, London. Subjects were not aware of the hypotheses being tested as they were part of a large study investigating many age-related diseases and traits for which informed written consent was obtained (www. twinsuk.ac.uk).
Three thousand five hundred and one consecutive women were recruited from the Twins UK Adult Twin Registry in London (wwww.twinsuk.ac.uk) between January 1995 and December 2003. The twins involved in this study have previously been shown to be representative of the UK singleton population in general (16). All were adult females aged between 18 and 79 years of age.
The validated protocol for naevus counts has previously been published elsewhere (17). In particular, a naevus was defined as a melanocytic lesion ≥ 2 mm in diameter to avoid any confusion with ephelides. Skin type was assessed according to the Fitzpatrick classification.
Total 25(OH)D levels were measured by radioimmunoassay using Diasorin RIA kit (Diasorin, Minnesota, USA) as previously described (10).
DNA was extracted from isolated leukocytes after an overnight fast and the mean leukocyte terminal restriction fragment length (LTL) was measured using the Southern blot method as described previously (18). The laboratory conducting the LTL measurements was blinded to all characteristics of the white cell donors.
All statistical analyses were performed using the Stata statistical software (Stata 12 Corp, USA). The covariates included height, weight, season of 25(OH)D measurement, LTL (as reflecting the chronological age), age and skin type according to Fitzpatrick. BMI is usually reported as a covariate to adjust for 25(OH)D level, but we preferred to include height and weight separately as height has been previously associated with naevi, while weight was not (19).
Associations between 25(OH)D levels and skin type, age, season of sampling, height and weight were investigated using Pearson correlations and linear regressions. For categorical data, chi square test was used. Logistic regression was used for calculating risk of low 25(OH)D serum levels in relation to skin type and with adjustments for age and season of sampling. Multicollinearity between variables was tested with the variance inflation factor, without significant results. All analyses were adjusted for the fact that the twin pairs were related using the command cluster in logistic regressions. Model selection was carried out by using the Bayesian Information Criterion, in which the potential confounders were analysed by assessing the top 10 models as generated by the Bayesian Information Criterion. The resultant linear regression residual plots were checked for violations of linear relations.
Three thousand five hundred and one Caucasian women have been included in the study. Mean age of volunteers was 46.5 years (range 18–79). Mean 25(OH)D levels was 75 nmol/l (median 68 nmol/l, range 5–300). 25(OH)D levels were influenced by season of blood sampling (r = 0.34 p < 0.0001): mean 25(OH)D level during the spring and summer months was 85.2 nmol/l compared to 65.4 nmol/l in the autumn and winter months (p < 0.001). Mean ± SD height was 163 ± 7 cm and was not correlated with 25(OH)D (beta 0.07, p = 0.50). Mean ± SD weight was 67.5 ± 12.9 kg and was inversely correlated with 25(OH)D (beta –0.35, p < 0.001). 25(OH)D levels decreased with age (coeff –0.15, p = 0.04).
There was a positive association between LTL and season adjusted 25(OH)D, when adjusting for height, weight and age (beta 2.48, p = 0.013). There was a positive association between skin type and 25(OH)D, with higher levels in skin type 3/4 compared to skin type 1/2 (beta 3.96, p = 0.017) when adjusted for season and age at time of sampling.
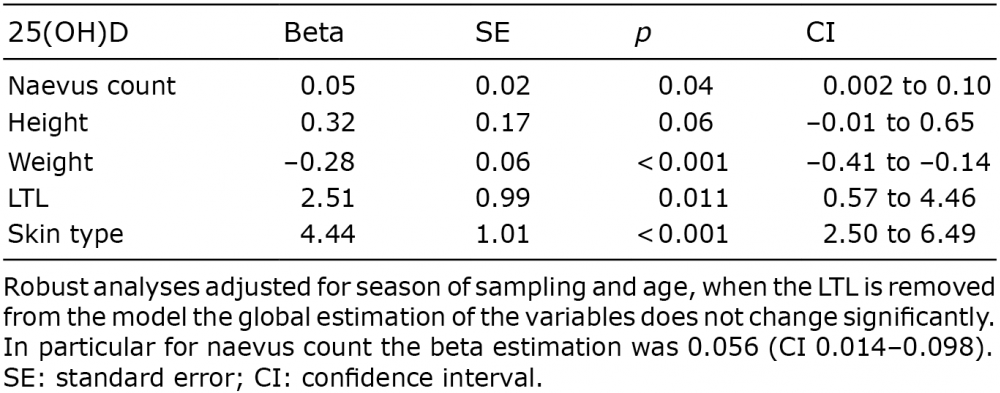
Naevi count were negatively associated with age (beta –0.52, p < 0.001) even after adjustments for height and weight. Mean total naevus count was 32 (range 0–298). Age-adjusted naevus count was positively associated to season-adjusted 25(OH)D (beta = 0.04, p = 0.02). Mean 25(OH)D was 73.3 nmol/l in twins with less than 50 naevi compared to 78.8 nmol/l (p = 0.002) in those with 50 or more naevi. This association between naevi and season-adjusted 25(OH)D was maintained even after adjustments for age, height, weight, season of sampling and skin type (beta = 0.056 p = 0.009) (Table I). Furthermore, the positive association between naevus count and 25 (OH)D was maintained even after adjusting for age-adjusted LTL with a slight decrease in the strength of the association (beta = 0.050 p = 0.036) (Table I).
Table I. Linear model for the association between 25(OH)D and naevus count, height, weight, skin type and further adjustment for leucocyte telomere length (LTL)
High numbers of naevi is one of the most powerful risk factor for melanoma which suggests a lack of senescence in melanocytes of individuals at high risk (4). We report, for the first time, a positive correlation between the number of naevi and serum levels of 25(OH)D after adjustment for age, weight, height, season of sampling and twin relatedness.
The association between skin type and 25(OH)D previously published using the TwinsUK dataset showed that lower levels of vitamin D are found in skin type I and II compared to skin type III and IV (20). However, our analyses on the association between 25(OH)D and naevi are adjusted for skin type. If skin type was a confounder, it would act the other way round as lower 25(OH)D levels would have been expected in fairer individuals who usually have more naevi (21) but the reverse was found with higher naevus counts associated with higher vitamin D levels, so skin type is unlikely to be a factor driving this association.
Melanoma and high naevus counts have been linked to longer LTL. 25(OH)D serum levels have also been reported to be an index of ageing as the levels decrease with age (10) so our findings of higher 25(OH)D in subjects at higher risk of melanoma supports the notion that the biological age of individuals with high naevus count might be younger than their chronological age, in line with their longer LTL and higher 25(OH)D levels. LTL was likely to play a role in the 25(OH)D-naevus count association reported here, as naevi count have previously been linked to longer LTL (8). However, despite adjusting for LTL, the association between naevi counts and 25(OH)D remained, so LTL does not fully drive the correlation and other factors must be involved.
A number of cohort studies have addressed a possible protective effect of 25(OH)D on melanoma risk (15). Despite this, no association has been reported between 25(OH)D supplementation and melanoma risk (22). It is therefore possible that higher 25(OH)D serum levels are proxy for other environmental and/or genetic factors which may impact on melanoma risk but not 25(OH)D intake alone. The fact that this study found a positive association between naevus count and higher vitamin D and that high naevus count confer a higher risk of melanoma may be seen as not supporting results of previous studies reporting a higher risk of melanoma with lower vitamin D levels (3). However, melanomas in individuals with low vitamin D (more likely to be older, with skin type 1 or 2 with thicker melanoma tumours) are likely to be quite different from melanomas associated with high naevus counts which affect younger individuals and are associated with thinner melanomas more often of the superficial melanoma type (14). So it is important to separate melanomas associated with high naevus counts from those with low naevus counts as the divergent melanoma pathways in terms of phenotypic risk factors have already been well described (23). High naevus counts whilst increasing melanoma risk, have also been found to offer survival advantage after adjusting for all melanoma prognostic factors (24). The same prognostic value was also maintained in positive sentinel lymph node (SLN) patients (stage III), who have usually worse prognosis (24–26). The association between 25(OH)D levels and improved melanoma survival (lower Breslow thickness and less ulceration) has been reported before in large studies (10, 14). SNPs determining 25(OH)D serum levels, have not yet been linked to melanoma prognosis or to melanoma prognostic factors such as Breslow thickness, ulceration or mitosis but sample size may be an issue for some of these studies. So it is possible that previous reports of vitamin D being protective in melanoma recurrence and death may be, in part, driven by LTL and naevus counts but this needs to be confirmed.
A limitation of the TwinsUK study is that all subjects were females. For historical reasons, the Twin Research Unit recruited mostly females. Despite this, the analyses are unlikely to be affected, as there are no reported effects of sex on 25(OH)D levels (27) as well as significant gender effects on total body naevus count and on its distribution (28, 29).
We have demonstrated that naevus count should be taken in consideration when looking at the association between 25(OH)D serum levels and melanoma risk. Telomere length, in part, influences the association between vitamin D levels and naevus counts. Other than LTL, other drivers for this association remain to be established but as vitamin D serum levels are linked to so many other phenotypes associated with to “better health” we would only speculate about what these factors could be. Further work is needed to investigate the protective role of vitamin D in melanoma and other malignancies and whether it acts as a proxy for other phenotypes. Future vitamin D studies in melanoma should look at different subtypes of melanomas separately (superficial spreading versus nodular melanoma, high versus low naevus counts) and the effects of the host phenotype such as skin type and sun exposure need to be explored further. Evidence is lacking that recommending vitamin D supplementation is effective in reducing cancer risk and mortality, so potential genetics and environmental factors (apart from sun exposure) which drive higher vitamin D levels need to be better understood.
TwinsUK is funded by the Wellcome Trust, Medical Research Council, European Union, the National Institute for Health Re- search (NIHR)-funded BioResource, Clinical Research Facility and Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust in partnership with King’s College London.


 Click to show fullsize
Click to show fullsize