


1Centre for Prevention of Infectious and Transmissible Diseases, 2Infectious Diseases Department, 3Bacteriology Department, and 4Dermatology Department, Nantes University Hospital, FR-44093 cedex 1 Nantes, France. E-mail: lefebvremaeva@gmail.com
Mycoplasma genitalium is a sexually transmitted non-Gram stainable bacterium. It is considered as an emerging agent of sexually transmitted infection (STI), but its testing is generally not recommended in population-based screening or symptom-based testing (1, 2). The lack of susceptibility of M. genitalium to antibiotics is an increasing concern, as illustrated for instance by the recent update of the Centre for Disease Control and Prevention (CDC), and European guidelines about non-gonococcal urethritis (NGU) (1, 2).
In recent years, several M. genitalium prevalence studies in diverse populations have been published, but such studies are rare in France, and there are few large cohorts on therapeutic strategies. In France, PCR for M. genitalium is performed only by a few centres, in cases of treatment failure for NGU.
The aim of this study was to evaluate the prevalence and pathogenic role of M. genitalium, through a systematic screening approach, in a male and female population attending a sexual health centre.
This cross-sectional study was conducted prospectively during a 4-month period (1 December 2013 to 31 March 2014) at Nantes STI Reference Centre, France. The population consisted of all male and female patients attending either the free and anonymous STI testing and counselling clinic, or the sexually transmitted diseases clinic in the centre. Patients were systemically asked about STI-related symptoms and risk factors: having new sexual contact or more than one partner in the last year, being a man having sex with men, being diagnosed with other STI, or being sexual contact of persons with an STI. After consent was obtained, this test was proposed in the same way as for Chlamydia trachomatis (CT), according to French guidelines: for women and men under 25 and 30 years of age, respectively, regardless of symptoms, and for people with STI risk factors or symptoms, regardless of age. Sampling was achieved via first-void urine in men, self-collected vagina swab in women, and in case of symptoms, by rectal, pharyngeal and/or endocervical swabs, if appropriate.
M. genitalium and T. vaginalis were detected using the Diagenode S-DiaMGTVTM, (Diagenode SA, Liège, Belgium), a commercial duplex real-time PCR targeting MgPa gene/Mg219 gene of M. genitalium and a 2-kb repeated sequence of T. vaginalis. Samples were tested following the guidelines from the manufacturer. CT and N. gonorrhoeae (NG) were detected by approved commercial PCR CobasTM 4800 CT/NG test. In case of symptoms, culture was also used for NG identification and susceptibility testing.
Patients’ demographic, behavioural, clinical, and microbiological data were entered in an anonymous database and analysed using STATA IC12 (StataCorp, College Station, Texas, USA). Results were expressed as means and standard deviations or frequencies, as appropriate. Prevalences were expressed with 95% confidence interval (95% CI). Comparison of groups used a χ2 or Fisher’s exact test for dichotomous variables, and Student’s t-test or the Wilcoxon rank-sum test for continuous variables. Univariate and multivariate logistic regression analyses were conducted to determine factors associated with symptoms (odds ratio (OR) and 95% CI), selecting variables with p ≤ 0.4 for the multivariate analysis.
All consecutive patients corresponding to the selection criteria gave their consent to participate in the study.
The study included 651 patients; 357 men (55%) and 294 women. Mean age was 23 ± 5.7 years for females and 28 ± 5.8 years for males. Eighty-two patients (12.6%) were born abroad, 49 (59.8%) of them in Sub-Saharan Africa. Among men, 92 (25.8%) reported having sex with men. Overall, 448 patients (68.9%) reported inconsistent condom use for genital or anal sex and no concurrent partner testing. Of the 651 patients, 52 (8%) were symptomatic. Twenty-three men presented with urethritis according to clinical criteria (purulent or clear discharge, burning or painful urination, dysuria). Other symptoms were testicular pain, ulceration, and inguinal lymphadenopathy. Among women, 21 reported symptoms, mostly vaginal discharge (n = 10), followed by dyspareunia and pelvic pain. Twenty-six patients (4%) presented as sexual contacts of patients diagnosed with STI.
Overall, the prevalence of CT and M. genitalium infection was 7.8% (95% CI: 5.7–9.9) and 2.4% (95% CI: 1.3–3.6), with similar rates in women and men (Table I). The prevalence of NG and T. vaginalis infection was the same: 0.92% (95% CI: 0.55–1.3). Considering asymptomatic and symptomatic subjects, the prevalence of M. genitalium infection was 1.8%, and 9.6%, respectively. Symptoms were more frequent in cases of M. genitalium infection (5/16: 31%) than in CT (8/51: 16%), the difference being non-significant (p = 0.27). Co-infection of CT and M. genitalium was seen in 6 patients (11.8% of CT infected subjects), whereas no cases of other co-infections were seen.
Table I. Prevalence (% (95% confidence interval)) of sexually transmitted infection agents by specimen type, age and sex of subjects
Factors associated with presence of symptoms were positivity of NG, M. genitalium, CT, and unprotected intercourse in the univariate analysis, while in the multivariate analysis, only positivity of NG, M. genitalium, and unprotected intercourse were independently associated with symptoms (Table II).
Table II. Factors associated with symptoms in the study population (n = 651)
Although the value of our results are limited by the possible underestimation of symptoms and risk factors, the very high participation rate, with no refusal, and the size of the whole study population make the study results representative. A second limitation of this study is the age difference in enrolment, according to sex and symptoms, which does not allow generalizing our prevalence findings to the potential exposed population. This potential sampling bias may also impact on the study of factors associated with symptoms. Finally, a limitation is the way the diagnosis of urethritis and cervicitis was made: without smear microscopy, as recommended in France.
The prevalence of 1.8% for M. genitalium in asymptomatic subjects was in the low range of that reported in other studies in Europe and Israel (2.1–6.1%) (3–5). Prevalence was 9.6% in symptomatic patients of our study, in accordance with that observed in symptomatic men attending an STI clinic in Israel: 11.9% (6).
Among CT infected subjects, 11.8% had concurrent M. genitalium infection, a rate similar to recent studies (7, 8), which constitutes a reason of failure to single dose of azithromycin, one of the first-line recommended treatments for CT infection (1, 2).
Although CT was associated with symptoms in the univariate model, it was not in the multiple logistic model. This negative result may be the consequence of an underpowered multivariate analysis, or missing unknown confusion factors. In contrast, the multivariate analysis shows an association between M. genitalium and symptoms, adding to available evidence that this bacterium should be considered as an agent of NGU and cervicitis (9–11). These results suggest that patients with signs of urethritis or cervicitis tested positive for CT might be more prone to have concomitant M. genitalium infection, and therefore be handled differently from a therapeutic standpoint. Indeed, the median cure rate with the 7-day doxycycline regimen is only 31%, and resistance mutations in 23S RNA emerge rapidly after azithromycin 1 g, yielding to declining cure rates over the years: 67% vs. 85.3% according to the studies published after and before 2009, respectively (1, 12). Among alternative treatments of M. genitalium disease, prolonged dosing of azithromycin also yield to increasing rates of failure, and moxifloxacin for 7 days appears to be currently highly effective, but has a potential for serious side-effects and gastrointestinal microbiota perturbations (13). Moreover, moxifloxacin failures have been reported recently, along with GyrA and ParC mutations (14).
In conclusion, incorporation of M. genitalium PCR into first-line tests for STI screening and diagnostic should be considered. Additional prospective randomized studies are needed to evaluate therapeutic strategies.


 Click to show fullsize
Click to show fullsize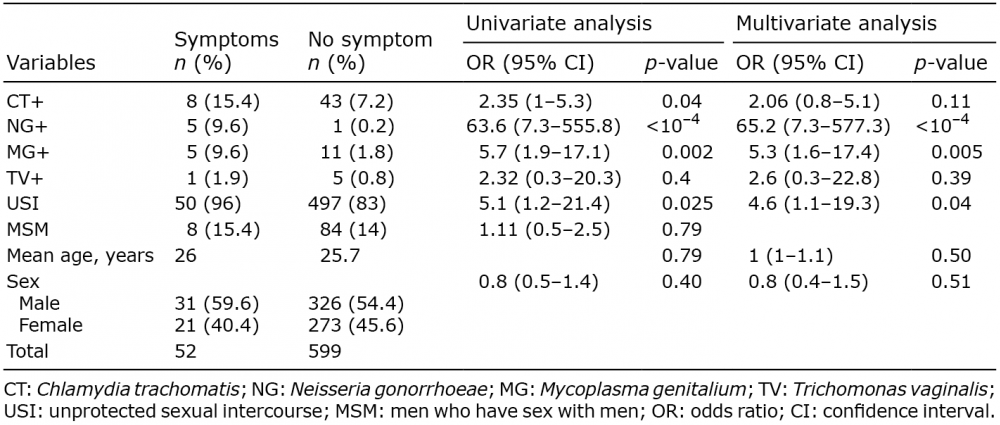 Click to show fullsize
Click to show fullsize