


1Department of Dermatology, Venereology and Allergology, and 2Institute for Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany
Becker naevus syndrome is a rare epidermal naevus syndrome defined by the co-occurrence of a Becker naevus with various cutaneous, muscular and skeletal anomalies. In the majority of cases, abnormalities exclusively consist of ipsilateral hypoplasia of the breast, areola and/or nipple in addition to the naevus. Here, we report on a 42-year-old woman with an extensive Becker naevus reaching from the left buttock to the left calf verified on histological examination. In addition, there was marked hypoplasia of the fatty tissue of the left thigh confirmed by magnetic resonance imaging in contrast to hyperplasia of the fatty tissue of the left gluteal area. Underlying muscles and bones were not affected. There was no difference in leg lengths. In addition, we review and discuss the features of Becker naevus syndrome with emphasis on 10 reported cases with involvement of the lower body.
Key words: Becker naevus; Becker naevus syndrome; hypoplasia of fatty tissue; lower body.
Accepted Nov 23, 2016; Epub ahead of print Nov 24, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Henning Hamm, Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Josef-Schneider-Str. 2, DE-97080 Würzburg, Germany. E-mail: hamm_h@ukw.de
Becker naevus is a rather common, benign anomaly, which is clinically characterized by a light- to dark-brown patch or flat plaque with a mean size of 125 cm² and irregular borders (1). In most cases, Becker naevus is localized unilaterally on the upper trunk, mainly the shoulder, chest or scapular region (2). Due to androgen stimulation, it often presents with hypertrichosis and darker colouration in postpubertal males. Tymen et al. (1) reported a prevalence close to 0.52%, whereas De Almeida et al. (3) made the diagnosis in 4.19% of 18-year-old Brazilian males. It is probable that more pronounced visibility, and the resulting greater aesthetic nuisance, in adolescent and adult males led to the erroneous assumption of a substantial male predominance of up to 4.5:1 (4).
On histological examination, Becker naevus shows hyperpigmentation of the basal layer with or without only slightly increased number of melanocytes, variable acanthosis with mild papillomatosis and elongation of rete ridges featuring flat tips. Typically, hypertrophy of the musculi arrectores pilorum and bundles of smooth muscle fibres not related to hair follicles are found in the dermis (5, 6).
Quite a number of dermatoses and cutaneous tumours have been described in spatial conjunction with Becker naevus, such as acneiform lesions (7–11), dermatitis (12), lichen planus (13–15), pityriasis versicolor (16–18), granuloma annulare (19), hypohidrosis (20), overlying ichthyosis (21), Bowen’s disease (22), basal cell carcinoma (23), lymphomatoid papulosis (24), multiple leiomyoma cutis (25), osteoma cutis (26), and underlying desmoid tumour (27).
In rare cases, Becker naevus has also been observed in association with developmental anomalies. Thus, in 1997, Happle & Koopman (28) coined the term Becker naevus syndrome (BNS) for the simultaneous presence of Becker naevus with certain cutaneous and subcutaneous, muscular and skeletal defects. Based on rare reports of familial Becker naevus (29–32) and one familial occurrence of BNS (33), the authors proposed paradominant inheritance. However, the genetic basis and mode of transmission are unsolved to date.
In contrast to Becker naevi, the sex ratio in BNS shows a 1.5:1 female predominance of published cases (34). However, this ratio could be incorrect in favour of female cases, since the syndrome is more easily recognized in women. The reason is that the most frequent anomaly in BNS consists of ipsilateral hypoplasia of the breast, areola and/or nipple, which is much more evident in females, albeit not confined to them. Other associated features include supernumerary nipples, scoliosis, vertebral anomalies and shortening or other kind of asymmetry of the upper limbs due to hypoplastic soft tissue (34). While BNS is usually restricted to the upper part of the body, observations involving the lower body are rare. We report on a case of BNS involving one leg and buttock, and review 73 previously published cases of BNS with special regard to its occurrence on the lower body.
A 42-year-old woman presented with a dark-brown hyperpigmentation of her left gluteal area and left thigh for cosmetic counselling. She was particularly disturbed by a skin fold of her left buttock drooping over the insertion of the thigh. She reported that the pigmentation had been present since birth and had become progressively darker since the beginning of puberty. Intensification of hyperpigmentation was accompanied by increasing irregularity of the skin surface and hair growth in this area. Moreover, the patient noticed a slow augmentation of the volume of her left gluteal area and a reduction in the circumference of her left thigh during the last 5 years. Her medical history was otherwise unremarkable. There were no similar cases in her family.
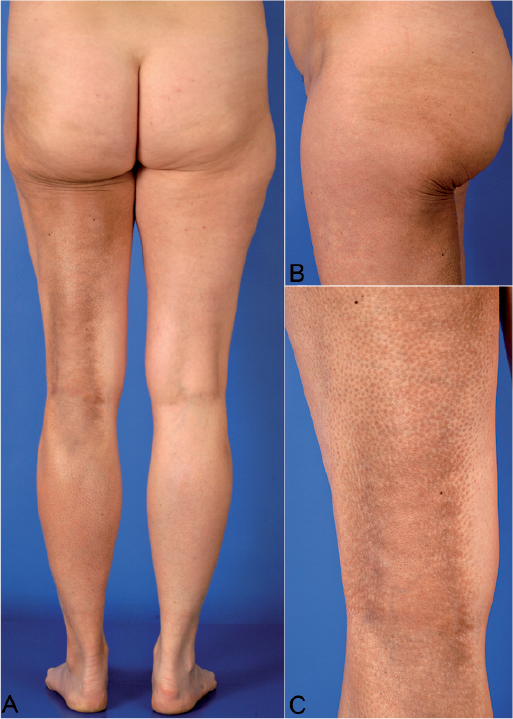
Physical examination revealed aggregated, follicular, slightly elevated, brownish papules, confluent to pigmented plaques at her left gluteal area, the dorsal aspect of the left thigh and the proximal calf (Fig. 1). Hypertrichosis was not evident, as her legs were clean-shaven. How-ever, dermoscopy revealed short-cut terminal hairs. The circumference of her left thigh was significantly reduced compared with the contralateral side (52.5 vs. 57.5 cm).
Fig. 1. Becker naevus syndrome involving the left buttock and leg. Note the hyperplasia of fatty tissue of the left gluteal area in contrast to hypoplasia of fatty tissue of the thigh. (A) General view. (B) Lateral view of left buttock and insertion of the thigh. (C) Detail of the lower part of the thigh and hollow of the knee.
Moreover, the adipose tissue of the left buttock was more bulky than on the right side (distance from spina iliaca to insertion of the thigh 41 vs. 39 cm). The legs were of equal length. A biopsy from the dorsal thigh showed epidermal acanthosis and hyperpigmentation of the basal layer without obvious increase in melanocytes, as well as hypertrophy of smooth muscle fibres, characteristic of Becker naevus (Fig. 2). A magnetic resonance imaging scan of her pelvis and legs confirmed hypoplasia of the fatty tissue of the left thigh and slight hyperplasia of the fatty tissue of the left gluteal area without involvement of the musculoskeletal system (Fig. 3).
Fig. 2. Histology from the left thigh showing slight papillomatosis, acanthosis and hyperpigmentation of the epidermal basal layer in conjunction with abnormal and separated bundles of smooth muscle in the reticular dermis (haematoxylin and eosin, original magnification ×100).
Fig. 3. Magnetic resonance tomography of the femora and left buttock. (A) Magnetic resonance tomography of the femora showing hypoplasia of the fatty tissue on the left thigh as well as a thickened and softly enhancing cutis corresponding to the clinical findings (T1 Turbo spin echo [TSE] fat saturated image after administration of i.v. Gd-DO3A-butrol contrast, axial view). Comment: Fatty tissue appears dark, contrast enhancing structures (vessels, cutis) appear bright. Muscles show intermediate signal intensity. (B) Magnetic resonance tomography showing prominent fatty tissue on the left buttock and hypoplasia of the fatty tissue on the dorsal aspect of the proximal left thigh, as compared to the ventral area (T1 TSE image before administration of i.v. contrast, sagittal view). Comment: Fatty tissue including bone marrow appears bright. Muscles show low to intermediate signal intensity.
Further total body examination showed no abnormalities. In particular, the breasts, axillary and pubic hair growth, as well as the musculoskeletal apparatus of the upper body, were unremarkable.
BNS denotes a Becker naevus in combination with other cutaneous and extracutaneous abnormalities. Possible associations have been well documented in a comprehensive survey of 55 cases of BNS published until 2004 (34). In total, 73 cases have been reported to date. Table I provides a summary of all anomalies observed so far (1, 4, 6, 33, 35–79). Of note, facial Becker naevus is an inconstant feature of a maxillofacial syndrome involving bones, teeth, gums, and skin, which is known under the terms hemimaxillofacial dysplasia (80, 81), segmental odontomaxillary dysplasia (82–84), and HATS (hemimaxillary enlargement, asymmetry of the face, tooth abnormalities, and skin findings) syndrome (85, 86). On account of its unclear relation to BNS, cases of HATS syndrome were not considered in Table I.
Table I. Extracutaneous anomalies in Becker naevus syndrome, as compiled from the literature
Furthermore, a questionable case of BNS with suggested Becker naevus bilaterally involving the genitocrural area and the neck associated with exceptional neurological, endocrine, cardiac, and further abnormalities, was not included (87).
Apart from the skin, breast and adipose tissue, bones and muscles are predominantly involved in BNS. Characteristically, associated anomalies are found ipsilateral to the naevus. In only 2 cases the contralateral side of the body was involved (45, 62), and bilateral involvement was noted in just a single case (41). Except for 3 instances, all associated abnormalities were of hypoplastic nature primarily affecting the female breast. It is noteworthy that discrimination between fatty tissue and muscle hypoplasia has been made in only a minority of cases. Items of hyperplasia included soft tissue swelling of the ipsilateral hand (70), hyperplasia of the ipsilateral lower limb (72), and enlargement of the ipsilateral foot (71). In the case presented by us, hypertrophy of the subcutaneous fat of the gluteal area ipsilateral to the naevus was noted.
As in non-syndromic cases, the most common sites of Becker naevus in BNS were shoulder, anterior chest, and scapular region. Less often, the naevus was located at the lower part of the body. Lucky et al. were the first to describe a patient with BNS affecting the lower limbs in 1981 (71). Including our report, 10 cases of BNS affecting parts of the body below the waistline have been reported in English language publications so far (Table II). Seven patients were female and 3 of male sex with a mean and median presenting age of 30 and 34 years, respectively.
Table II. Published cases of Becker naevus syndrome involving the lower body
In addition to our case, 3 more BNS patients with lipoatrophy of the ipsilateral leg are on record (48, 73), and in another case hypertrophy of the ipsilateral lower limb was observed (72). In 2 cases the leg affected by the naevus was shortened (47, 69). Further abnormalities included bilateral internal tibial torsion (41), accessory perineal scrotum (76) and hypoplasia of the contralateral labium minus (45). In 4 patients with a Becker naevus at the lower extremity the associated anomaly was localized on the upper part of the body (59, 60, 63, 78).
Whether BNS actually involves the lower body significantly less often than the upper one or whether it is underdiagnosed in this region is a matter of speculation. Due to the preferential location of Becker naevus on the upper trunk, together with the spatial relationship to extracutaneous anomalies, it is tempting to assume a real difference in frequency of body area involvement. On the other hand, when confined to the lower body and lacking the hallmark of unilateral breast hypoplasia, diagnosis of BNS is more challenging. A number of BNS cases located at unusual sites may have been mistaken for other forms of melanosis or for congenital melanocytic naevi (CMN).
Several cutaneous mosaic phenotypes other than Becker naevus may occur in combination with congenital hypo-plasia or, more rarely, hyperplasia of subcutaneous fat and deeper structures. A decrease in bulk of subcutaneous tissue is a well-known feature of large and giant CMN highlighted recently in a study on growth and hormone profiling issues (88). Lipomatous soft tissue masses in CMN with diffuse infiltration of the naevomelanocytes within fat lobules are also on record (89). Most of the large, giant and multiple CMN are caused by oncogenic mutations in codon 61 of the NRAS gene (88). Body asymmetry resulting from unilateral trunk and/or limb hypo- or hyperplasia is the most frequent extracutaneous anomaly associated with cutis marmorata telangiectatica congenita (90). Likewise, pronounced lipohypoplasia of the right buttock and thigh as well as hypoplasia of the breast has been observed in phacomatosis cesioflammea (91). This and other types of phakomatosis pigmentovascularis have been shown recently to belong to the group of mosaic heterotrimeric G-protein disorders by detection of activating mutations in GNA11 and GNAQ genes (92). Dysregulated adipose tissue including lipomas, lipohypoplasia, fatty overgrowth, and localized fat deposits is a frequent manifestation of Proteus syndrome caused by somatic activating mutations in the gene encoding the growth-promoting serine/threonine kinase AKT1 (93). Similarly, related overgrowth disorders with considerable clinical overlap between each other, such as fibroadipose overgrowth, hemihyperplasia multiple lipomatosis, congenital lipomatous overgrowth, vascular malformations, epidermal naevi, scoliosis/skeletal and spinal (CLOVES) syndrome, and megalencephaly-capillary malformation (MCM) syndrome, are caused by mutations in other signalling proteins of the RTK/PI3K/AKT/mTOR pathway and constantly present with adipose dysregulation, either lipomatous lesions or regional lipohypoplasia (94). Mosaicism of lethal autosomal mutations only compatible with life in a mosaic state has been proven at the molecular level for Proteus, CLOVES and MCM syndromes, as well as for large/giant CMN (95).
In contrast, the molecular basis of BNS is unknown. Based on the spectrum of extracutaneous anomalies, one may assume that the causative gene(s) is involved in the regulation of adipose tissue distribution. Since BNS is expressed in a segmental pattern, a lethal autosomal mutation only surviving as a mosaic seems to be the most likely genetic explanation.
Although patients may feel significantly disturbed due to the conspicuousness of a Becker naevus, therapeutic modalities are limited. Sequelae of surgical excision may be more visible than the original lesion. Pigment removal by Er:YAG laser ablation was found superior to Q-switched Nd:YAG laser treatment (96). Ablative fractional laser therapy was estimated as moderately effective, but the results were impaired by post-inflammatory hyperpigmentation (97). One case was treated successfully with topical flutamide (98). Spironolactone as an anti-androgen agent was tried in one female with breast hypoplasia and was reported to lead to its enlargement one month after initiation of therapy (55). In some cases breast hypoplasia and bone abnormalities, such as scoliosis, were corrected surgically.
In conclusion, Becker naevus is a rather common, benign anomaly, whereas its association with structural anomalies of soft tissue, muscles and bones is a rare event. Since its original description, 73 observations of BNS, excluding questionable facial cases, were published in the medical literature retrievable by PubMed/MEDLINE. Including our report, the lower body was involved in 10 BNS cases. Patients with a diagnosis of Becker naevus should undergo clinical evaluation for associated soft tissue, muscular and skeletal abnormalities. If BNS is suspected, magnetic resonance imaging is the imaging technique of choice, which can support the diagnosis and which is advisable prior to any surgical intervention. Treatment options are limited.
The authors are grateful for the excellent clinical photographs taken by Gerhard A. Krämer, Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Germany.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize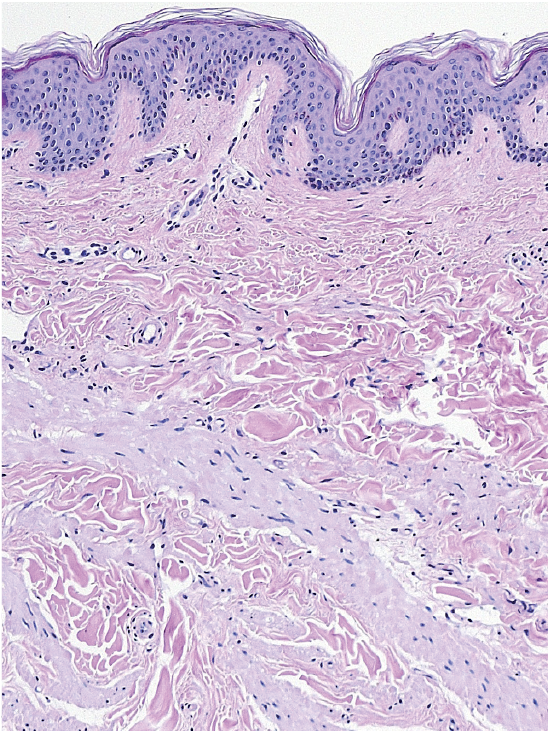 Click to show fullsize
Click to show fullsize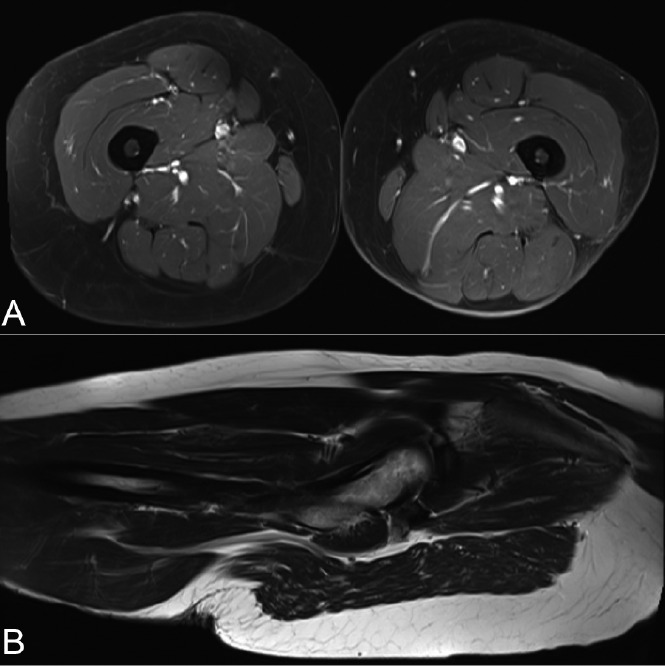 Click to show fullsize
Click to show fullsize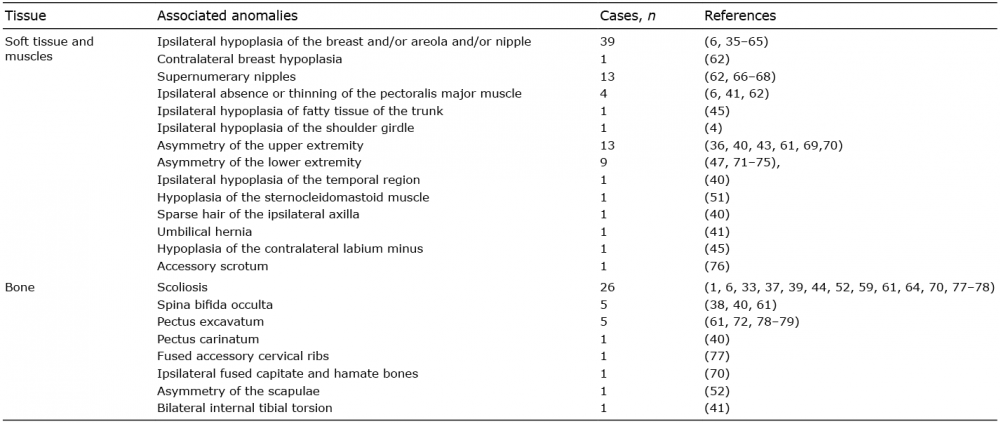 Click to show fullsize
Click to show fullsize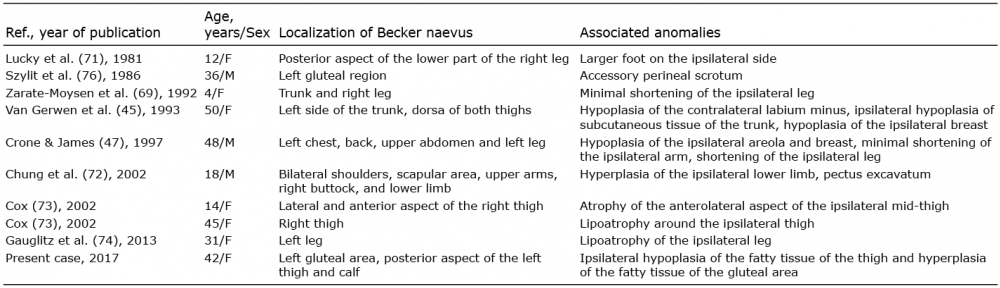 Click to show fullsize
Click to show fullsize