


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Mu?nster, and 2CVderm – German Center for Health Services Research in Dermatology, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, Hamburg, Germany. E-mail: sonja.staender@uni-muenster.de
Accepted Dec 8, 2016: Epub ahead of print Dec 8, 2016
Chronic pruritus (CP) is a frequent symptom in the general population and in many skin and systemic diseases (1, 2). A population-based cohort study found the 12-month cumulative-incidence of CP to be 7% and lifetime prevalence 25.5% (3). Determinants of prevalent CP, based on cross-sectional multivariate analysis, were: liver disease (prevalence ratio 2.1), asthma (1.8), eczema (2.7), increased body mass index (1.0), higher anxiety scores (1.1) and dry skin (1.9) (3).
Dry skin is characterized by a disrupted barrier, resulting in roughness, desquamation, lack of brightness of the skin surface and development of pruritus (4). Therefore, the European Guideline on chronic pruritus recommends emollients as first-line therapy to restore the skin barrier and to induce relief of pruritus (5). Topical N-palmitoylethanolamine (PEA) has been described as having emollient and antipruritic characteristics (6–8). The aim of this study was to compare the effects of twice-daily application for 2 weeks of a derma-membrane system (DMS)-based dermatocosmetic lotion containing PEA with the vehicle in subjects with CP due to dry skin, with regard to symptom improvement, quality of life and cosmetic acceptance.
A total of 100 subjects were included and randomized either to the vehicle lotion (group 1, n = 51: 27 women, 24 men; age range 18–83 years, mean age 54.9 ± 16.7, median age 54.0 years) or to the PEA-containing lotion (group 2, n = 49: 29 women, 20 men; age range 24–83 years, mean age 59.5 ± 15.2, median age 61.0 years) (Fig. S1).
At baseline all subjects had pruritic dry skin with no further skin symptoms. Additional scratch lesions were observed in one-third of subjects in both groups.
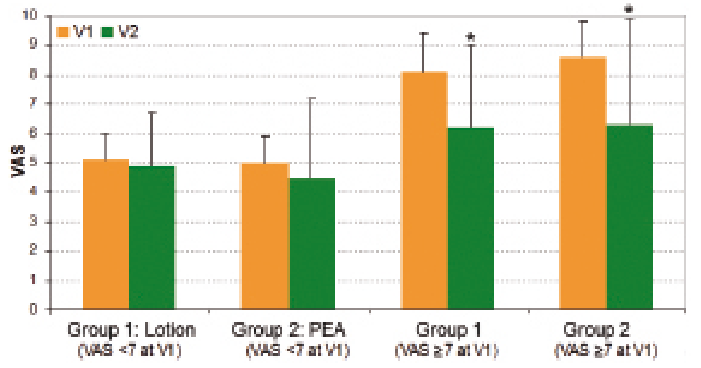
Pruritus intensity, as assessed by visual analogue scale (VAS), decreased significantly from baseline and treatment onset (V1) to 2 weeks (V2) (p < 0.001) and considering pruritus intensity at study onset, only those subjects with severe pruritus (VAS >7) at onset showed significant itch reduction from V1 to V2 (p < 0.001, per protocol (PP)) (Fig. 1). Differences between the 2 groups were not significant for either variable.
Fig. 1. Pruritus intensity at study visits as measured by visual analogue scale (VAS). In each group (group 1: derma-membrane system (DMS)-based lotion, no N-palmitoylethanolamine (PEA); group 2: DMS-based lotion with PEA), patients were divided into those with baseline <7 vs. those with baseline ≥7 (per protocol analysis, visit 1 (V1) to visit 2 (V2)). *p < 0.001.
Pruritus, as assessed by verbal rating scale (VRS), decreased from V1 to V2 (p = 0.223, PP) and from V1 to the follow-up visit 2 weeks after the end of treatment (V3) (p = 0.003, PP) across both groups. The decrease was significant only in the per-protocol analysis between V1 and V3.
Based on the percentage score, pruritus improved, on average, at V2 (group 1: 24.2 ± 29.3%, n = 40; group 2: 30.1 ± 29.8%, n = 41; p = 0.378) and V3 (group 1: 22.4 ± 30.5%, n = 30; group 2: 28.6 ± 35.9%, n = 22; p = 0.505) across both groups without significant group differences. Descriptively the improvement was rated higher in group 2. Stinging sensations increased non-significantly in group 1 from V1 to V2, and remained stable in group 2. This time-by-group effect was significant only in the PP analysis (p = 0.024).
Health-related QoL, as measured with the Dermatology Life Quality Index (DLQI), improved significantly from V1 to V2 across both groups (p < 0.001) without significant inter-group differences.
From V1 to V2, skin roughness increased slightly in group 1 and decreased in group 2. Differences between the groups were again not significant (p = 0.093).
Scaling decreased across both groups from V1 to V2 (p = 0.118, PP) and from V1 to V3 (p = 0.344, PP) without significance in the differences between the groups.
Chronic scratch lesions, such as prurigo, decreased in both groups from V1 to V2. The time effect was significant (p = 0.01), but the group differences were not (p = 0.833).
The 2 treatment groups had the same global patient-defined treatment benefit, with values ≥1 reflecting clinical benefit. Of the single treatment goals, the one best achieved was ‘’confidence in therapy’’, followed in group 1 by ‘’less out-of-pocket treatment costs’’ and ‘’less side-effects’’; and in group 2 by ‘’no more pain’’ and ‘’less burden in partnership’’. There were no significant differences between the 2 groups.
The majority of subjects in both groups rated a twice-daily application of lotion as sufficient and all cosmetic properties as good, except for the smell in group 2, which was rated as “bad” by 5.0% of subjects. There were no significant group differences.
At V2, and of the subjects having sleeping problems (group 1: n = 18; group 2: n = 14) due to dry skin, 27.8% (n = 5) in group 1 and 42.9% (n = 6) in group 2 reported an improvement in sleeping problems due to the treatments, without significance between the groups (p = 0.436).
Six subjects (13.3%) in each group reported adverse events related to worsening of skin symptoms, such as pruritus, stinging, scaling or reddening.
In the past, antipruritic effects of products containing PEA have been reported in case series of patients with atopic dermatitis and uraemic pruritus (6, 7), indicating a specific antipruritic mechanism associated with PEA (8). However, these case series did not compare the effect with a vehicle group. It was speculated, that PEA binds to the cannabinoid-2 receptor on skin cells and thereby ameliorates pruritus (8). In fact, PEA, together with N-acetylethanolamine, was demonstrated to reduce transepidermal water loss and increase skin barrier func-tion to a higher level than traditional emollients (9). Based on this, a higher response in the group applying the PEA-containing lotion was expected. In contrast to our hypothesis, in this study there was no significant difference between the lotion with and without PEA in terms of improvement in pruritus and quality of life. Differences between the groups in terms of pruritus improvement (ΔVAS; group 1: 0.6 points; group 2: 1.1 points) were present, but not significant. Based on the percentage score reduction, pruritus in the PEA group improved at V2 vs. V1 by more than 30%. Considering that in pain studies responders are defined as those with ≥30% reduction in pain intensity (10), this result in the PEA group is indicating a slight, although not significant, advantage of the PEA-containing lotion over its vehicle. It was also interesting that the significant superiority observed for PEA regarding reduction in stinging from V1 to V2 in the time-per-group effect of the PP analysis. This supports the observation made previously in case series, where the PEA-containing lotion showed anti-nociceptive effects in post-herpetic neuralgia (11). However, since no adjustment for multiple testing was performed in this study, further trials should test for differences in reduction in stinging between the 2 lotions, using this parameter as the main outcome criterion. A further limitation of the study was the absence of untreated control group. Thus, a possible placebo effect (12) or spontaneous remission cannot be excluded as possible reasons for the improvements seen.
It was also of relevance for the subjects in this study that the cosmetic properties of both treatments were perceived as good, thus facilitating the recommended twice-daily application. Clinical studies investigating antipruritic effects of emollients in chronic pruritus due to dry skin are rare. To our knowledge, this is the first study of a cohort of patients with chronic pruritus from a specialized itch clinic, to systematically investigate the comparative efficacy of 2 emollients, a PEA-containing lotion and its vehicle, on dry itchy skin. Despite its limitations, this study supports the recommendation for regular application of emollients on dry skin, even in subjects with long-standing pruritus, as it has been shown that this can lead to improvements in symptoms, especially with regard to quality of life and reduction in pruritus.
Conflicts of interest: The study was supported by Stiefel Laboratories, GlaxoSmithKline GmbH & Co. KG. CB, MA, and SS all received honoraria and travel expenses from Stiefel Laboratories.


 Click to show fullsize
Click to show fullsize