


Departments of 1Dermatology, 4Clinical Biochemistry, 6Hepatology and Gastroenterology and 7Paediatrics, Aarhus University Hospital, Aarhus, Departments of 2Dermatology and Allergy and 5Hepatology and Gastroenterology, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark, 3National Advisory Unit on Pregnancy and Rheumatic Diseases, Department of Rheumatology, Trondheim University Hospital, Trondheim, Norway, 8Department of Dermatology and Allergy Centre, Odense University Hospital, Institute of Clinical Research, University of Southern Denmark, Odense, 9Department of Dermatology, Copenhagen University Hospital, Roskilde, 10Dermatology Clinic, Hudlaegecenter Nord, Aalborg, 11Dermatology Clinic, Copenhagen, and 12Dermatology Clinic, Odense, Denmark
Methotrexate (MTX) has been used in the treatment of psoriasis and other dermatological diseases for more than 50 years. However, there is limited evidence regarding its effect, dose and monitoring, and a lack of consensus regarding how the drug should be used in daily practice. Although the use of MTX is governed by guidelines, such as the European S3-Guidelines and the National Institute for Health and Care Excellence (NICE) guideline, it is important to discuss and adjust these guidelines to national standards. An expert meeting was held in Denmark at the end of 2014, in order to reach consensus regarding the use of MTX in dermatological practice in Denmark. Participants included dermatologists, hepatologists, paediatricians, clinical biochemists and a rheumatologist. Topics discussed were: liver disease monitoring, teratogenic effects of MTX, risk of cancer, and use of MTX in children. We report here the conclusions of this expert meeting regarding use of MTX in dermatological practice.
Key words: psoriasis; skin diseases; methotrexate.
Accepted Dec 12, 2016; Epub ahead of print Dec 13, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Claus Zachariae, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, Denmark. E-mail: claus.zachariae@regionh.dk; and Lars Iversen, Department of Dermatology, Aarhus University Hospital, DK-8000 Aarhus, Denmark. E-mail: lars.iversen@clin.au.dk
Methotrexate (MTX) is a folic acid antagonist that was first used in the treatment of acute leukaemia in the early 1950s and subsequently for the treatment of solid tumours. Low-dose MTX has also been used successfully for the treatment of rheumatoid arthritis and psoriasis; and over the past 25 years, MTX has become the standard of care in the treatment of these 2 diseases (1–3). The effect of MTX was originally described as anti-proliferative, as the drug induces inhibition of purine, methionine and thymidylate synthesis, and thereby inhibits DNA synthesis. MTX is transported into the cells by either a folate carrier or by passive diffusion, and is polyglutamated once inside the cells (4). Whereas MTX has a half-life of 5–8 h, the MTX polyglutamates are retained in cells and tissues for several weeks or months (5). It was suggested that low-dose MTX treat-ment, e.g. the doses used in psoriasis, may also have anti-inflammatory effects, including increased adenosine levels, and MTX has been shown to modulate immune cells and to decrease the level of tumour necrosis factor alpha (TNFα), among other effects (3, 6).
MTX has been used in the treatment of moderate-to-severe psoriasis for many years; yet, the first randomized controlled trials were not performed until 2003. These studies compared MTX with cyclosporine (7, 8). MTX was later compared with different biologics in other randomized controlled trials (9–11). Even so, evidence for its effect remains limited. Yet, MTX is used for the treatment of a wide range of dermatological disorders, including pityriasis rubra pilaris, atopic dermatitis, chronic urticaria, pityriasis lichenoides, blistering disorders, cutaneous lupus erythematosus, localized scleroderma, vasculitis, cutaneous sarcoidosis, dermatomyositis and granuloma annulare (6). This report focuses on experience with MTX in the treatment of psoriasis.
For dermatological indications, MTX is used in low doses compared with those used in oncology. No studies have established the best starting or maintaining dose for dermatological indications (12), although a few studies have compared different doses of MTX in the treatment of psoriasis (13, 14). The general recommendation in psoriasis is to start at 5–15 mg once weekly, with dose escalation up to 25–30 mg weekly, depending on the clinical response (15, 16). The doses of MTX used for other dermatological diseases are similar to those used in psoriasis (6). Caution is recommended when treating elderly patients and patients with impaired kidney function (15).
According to the National Institute for Health and Care Excellence (NICE) guideline, the maximum treatment response is usually seen 16–24 weeks after treatment initiation, although maximal effect will occasionally be reached within 8–12 weeks of treatment with 15 mg weekly doses (16). Both the PASI75, which is equal to a 75% reduction in the skin manifestation of psoriasis, and patients’ quality of life improve significantly after treatment with MTX (17). In a randomized controlled trial, 62% of patients reached a PASI50 after 16 weeks of treatment, whereas 36% reached a PASI75. However, due to a low MTX starting dose (7.5 mg), these numbers are likely to be underestimated (9). This is supported by retrospective studies in which 40% and 62% of the patients achieved a PASI75 after 12 and 24 weeks of MTX treatment, respectively (18). In Denmark, it is usually recommended to evaluate the effect after 12 weeks of psoriasis treatment with the maximum tolerated dose of MTX (17).
In dermatology, MTX is administered orally or as a subcutaneous injection. In general, the oral administration route is the first choice owing to its simplicity and lower price. However, if there is lack of efficacy or unacceptable side-effects, it is recommended to change the administration route to subcutaneous injection, which can increase the efficacy and tolerability (19, 20).
Some of the most common side-effects of low-dose MTX, such as nausea, anorexia, fatigue and malaise, are very inconvenient for the patient, although not dangerous. These side-effects are dose-dependent and usually occur at initiation of therapy (6), and they may be reduced by folic acid supplementation (21). MTX can cause haematopoietic suppression, and haematopoietic biochemical monitoring is therefore recommended during treatment. MTX can also lead to pancytopaenia; however, this is a rare side-effect at the low-level doses used in dermatological diseases (22). The ability of MTX to induce liver toxicity is an important side-effect discussed in detail below.
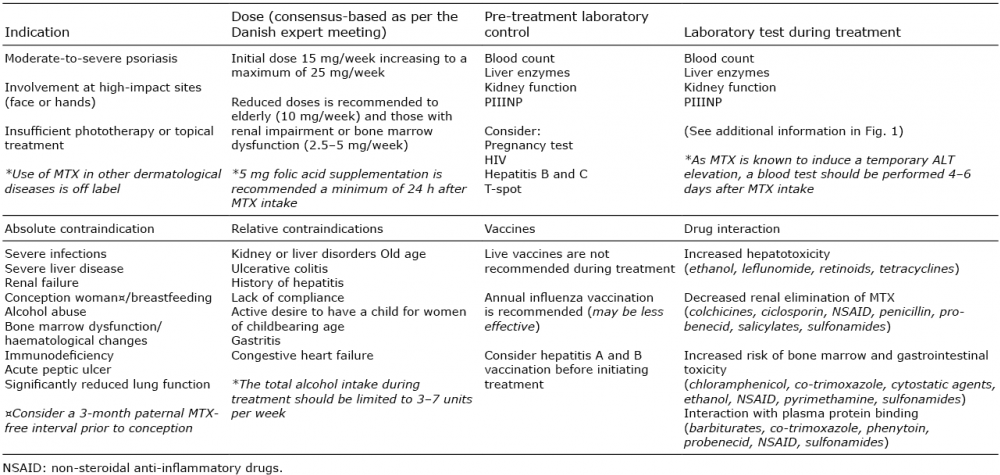
Even though the efficacy of MTX is lower than the biological therapies used in psoriasis, MTX is the first-line systemic treatment for psoriasis in Denmark owing to its cost-effectiveness and the extensive experience in the use of this drug accrued over many years (23, 24). MTX is therefore used very frequently in dermatological settings; however, national guidelines on how to monitor MTX treatment are lacking. The aim of this paper is to provide recommendations regarding the use of MTX in a dermatological setting. Recommendations regarding the indication, dose and laboratory tests are summarized in Table I (15).
Table I. Recommendations regarding use of methotrexate (MTX)
MTX has been recognized as a hepatotoxic drug, which may limit its therapeutic use (25). Based on the literature and the discussion at our meeting, we suggest the approach summarized in Fig. 1 before and during treatment with MTX. Briefly, before treatment, liver enzymes and procollagen III aminopeptide (PIIINP) are tested; and if baseline values are elevated, fibroscan or change to another treatment is recommended. After treatment initiation, alanine aminotransferase (ALT) is measured after one week and then every second week for the first 2 months and then every 3 months. PIIINP is measured every 6 months and measurement is repeated within weeks if levels are elevated compared with baseline values. Further control is needed (Fig. 1) if ALT is increased by more than 1.5-fold or if PIIINP is elevated in 3 successive samples and cannot be explained by, for example, psoriatic arthritis.
Fig. 1. Algorithm for methotrexate (MTX) treatment and monitoring of liver toxicity and fibrosis. #Reference Limit (RL), method-specific. *Primary use of alanine aminotransferase (ALT) to monitor liver toxicity if procollagen III aminopeptide (PIIINP) is elevated due to, for example, psoriatic arthritis.
The pathogenesis of MTX hepatotoxicity includes hepatic folate depletion by MTX. Folate supplementation therefore results in a marked reduction in hepatotoxicity (26). In addition, polymorphisms in the gene encoding the MTHFR enzyme have been related to low-dose MTX-induced hepatotoxicity (27). The pathological changes in the liver following MTX are characterized by fat infiltration with subsequent inflammation and fibrosis and potentially development of cirrhosis. A number of risk factors associated with liver steatosis, inflammation and fibrosis may increase the risk of MTX-induced liver toxicity (Table II). These risk factors include obesity, dyslipidaemia and diabetes as part of the metabolic syndrome and are strongly associated with non-alcoholic fatty liver disease (NAFLD) including steatohepatitis (NASH) (28). Furthermore, excessive alcohol intake and other hepatotoxic drugs, e.g. non-steroidal anti-inflammatory drugs (NSAIDs), are important risk factors.
Table II. Risk factors for methotrexate (MTX)-induced liver toxicity
The incidence and prevalence of MTX toxicity is debated. However, there is little doubt that cumulative doses are associated with hepatotoxicity. In older studies, a worsening on Roenigk’s 5-grade histological classification scale was observed in 28% of patients; patients had a 7% risk of progressing at least one histological grade for each gram of MTX taken. The overall incidence of advanced pathological changes ascertained in liver biopsies (grades IIIB or IV) was 5% (29). In a recent meta-analysis of observational studies, a 22% increased risk of “any fibrosis” on biopsy was reported following MTX therapy. In this meta-analysis, the cumulative dose and duration of MTX therapy was not associated with biopsy-verified fibrosis or cirrhosis. Recent data also show that the risk of cirrhosis development with end-stage liver disease is quite limited, as determined by the very low number of patients listed for liver transplantation (30).
Liver biopsy is the gold standard for assessment of the severity of any liver disease, e.g. NASH or alcoholic liver disease with fibrosis, before MTX treatment is initiated, and may also be used during MTX treatment. However, performing a liver biopsy is associated with increased morbidity and mortality due to the risk of bleeding (31), and surrogate markers for liver disease are therefore often used. Most often, liver injury is assessed via the liver enzyme ALT, which is elevated in 7.5–26% of all patients treated with MTX depending on the cut-off level used (32). However, more specific methods are needed, in order to limit the number of liver biopsies and to evaluate the risk of liver fibrosis.
The PIIINP has been used in the assessment of liver fibrosis, as fibrogenesis results in the release of certain extracellular matrix proteins, including PIIINP, into the bloodstream. PIIINP is a molecule that derives from type III procollagen biosynthesis (33). Changes in PIIINP
levels are not specific to a particular disease, but reflect the involvement and altered metabolism of type III collagen depending on the activity and the extent of the tissue involved. Levels are high in children and adolescents as a result of physiological growth (34). In conditions where accumulation and/or degradation of connective tissue takes place, PIIINP levels are increased; and interpretation of the individual PIIINP values can be challenging because active joint involvement, smoking and other factors may lead to an increase in PIIINP levels that is unrelated to hepatic fibrosis (15). PIIINP is therefore less useful for monitoring of patients with psoriatic arthritis (35, 36), and therefore there is a need for further development of biomarkers.
A meta-analysis on assessments of liver toxicity in MTX-treated patients with psoriasis calculated that
PIIINP had a sensitivity of 77% and a specificity of 92%. Thus, PIIINP can be expected to have a good negative predictive value when the prevalence of severe fibrosis is expected to be low (37). In general, the risk of development of hepatic fibrosis is minimal if serial measurements of PIIINP are normal (35, 36).
The Enhanced Liver Fibrosis test (ELF™, Siemens Healthcare Diagnostic Inc., Tarrytown, NY, USA) was introduced recently as a non-invasive test of liver fibrosis. An ELF score is calculated using an algorithm based on analysis of PIIINP, hyaluronic acid and tissue inhibitor of matrix metalloproteinase-1 (TIMP-1). Studies indicate that the ELF test can be used to detect fibrosis in chronic liver diseases, such as primary biliary cirrhosis, NAFLD and chronic hepatitis C infection, and that the score has a higher diagnostic value than the individual tests alone (38–41). At present, only a single study has studied ELF as a non-invasive marker of MTX-induced hepatotoxicity (42). From this study it was concluded that ELF may be at least equivalent or possibly superior to PIIINP. The PIIINP assay that is part of the ELF test is different from the Orion Ercopharm PIIINP radioimmunoassay, which has been studied extensively. The Siemens PIIINP from the ELF test gives higher values due to a different standardization, but the values compare relatively well (43).
During the past decade other non-invasive tools, such as transient elastography and fibro test to monitor hepatotoxicity in MTX-treated patients with psoriasis, have been introduced, but large prospective studies are needed (44). Also fibroscan for liver fibrosis have become available and have proven effective in other fibrotic liver diseases (45). This has been evaluated in a few trials studying MTX-induced liver toxicity. In a study of patients with psoriasis only, the median fibroscan value was 6.4 kPa (range 3.3–18.4 kPa) and the fibroscan correctly identified 88% of the patients without significant liver fibrosis based on a liver biopsy (METAVIR score < F2, fibroscan ≤ 7.1 kPa) (46). However, fibroscan has yet to be validated for use in MTX-treated patients. Other scanning modalities are required and better biomarkers for liver disease severity and progression are needed.
MTX hepatotoxicity remains a clinical challenge in patients with psoriasis, and monitoring is important. The algorithm shown in Fig. 1 is recommended, and the importance of recognizing the increased risk of liver fibrosis in at-risk patient groups (Table II) is stressed. New imaging modalities and biomarkers for liver fibrosis provide the basis for non-invasive assessment of MTX liver toxicity.These tools will reduce the need for liver biopsies during follow-up of patients who receive MTX treatment.
MTX is embryotoxic in humans and animals (47). Different forms of embryopathies have been described after exposure during gestational weeks 5–8. The most severe malformation is “aminopterin syndrome” consisting of multiple central nervous system (CNS), skeletal and cardiac abnormalities. New prospective studies in patients with rheumatoid arthritis have shown no increase in spontaneous abortion or in congenital malformations when MTX was given 6–0 months before conception. However, when given at doses of 10–20 mg/week during the first trimester, a high rate of spontaneous abortion (20–40%) and a slight increase in congenital malformations with a variety of single and combined defects, as well as cardiac defects at high doses have been observed (48). Therefore, MTX must be discontinued in women 1–3 months before a planned pregnancy. Folic acid supplementation should be given to all patients of fertile age who are receiving MTX treatment, and supplementation should be continued during the first trimester even after withdrawal of MTX before a planned pregnancy.
In general, MTX at doses between 5 and 25 mg/week do not impair spermatogenesis. Several recent cohort studies investigating the outcome of pregnancies fathered by men who had taken MTX within 3 months before conception have failed to show any increase in congenital malformations in their children (49). A 3-month paternal MTX-free interval prior to conception does not appear to be necessary (50, 51). However, the drug information leaflet and the European S3-Guidelines still recommend a 3-month MTX-free interval before conception (15). The need for this interval should be considered on an individual basis.
Low-dose MTX given for treatment of skin diseases can induce congenital malformations if administered during gestational weeks 5–8. MTX treatment during the first trimester may increase the rate of spontaneous abortion. MTX treatment must therefore be discontinued 3 months prior to planned pregnancy in females. There is no evidence to indicate that male fertility is impaired by standard doses of MTX; nor is there any evidence to support an increased rate of birth defects after paternal low-dose MTX intake around conception. However, the European S3-Guidelines still recommend a 3-month paternal MTX-free interval prior to conception, and it should therefore be considered on an individual basis.
The risk of cancer in patients with immune-mediated inflammatory diseases has been debated in recent years. Chronic inflammation may have a pro-tumourigenic effect and immunosuppressive treatment may increase the risk, but, at the same time, inflammatory cells and cytokines may have an anti-tumour effect.
Studies of patients with psoriasis have shown an increased risk of some solid cancers, especially cancers related to the respiratory tract, urinary tract and liver cancer (52). These are cancers that have been related to alcohol consumption and smoking habits, which are more common in patients with psoriasis (53). The risk of lymphomas has been shown to be slightly increased in patients with psoriasis (54). Patients with psoriasis also have an increased risk of non-melanoma skin cancer, especially squamous cell carcinomas (SCC) (55). The increase in non-melanoma skin cancer has been associated with previous use of ultraviolet (UV) treatment, especially psoralen plus ultraviolet A (PUVA), but immunosuppressive treatment, such as cyclosporine, may also increase the risk (56–58). Furthermore, MTX has been associated with an increased cancer risk in 1 study (56). Whether MTX treatment alone increases the risk of cancer in patients with psoriasis is debated. There have been some cases of lymphoproliferative diseases in patients treated with MTX; however, most of these patients had rheumatoid arthritis, and only a few cases have been reported in patients with psoriasis (59).
MTX is also used for treatment of many types of cancers and, in line with acitretin, MTX is recommended as treatment for moderate-to-severe psoriasis in patients with a history of previous cancer.
One study in patients with psoriasis who had previously been treated with PUVA and subsequently with MTX showed an increased risk of SCC (58). No studies have found an increased risk of non-melanoma skin cancer following a combination of UVB treatment and MTX. However, it is generally recommended to routinely screen the skin for skin cancer during treatment with immunosuppressive drugs, including MTX. This should be done at least once a year.
MTX clearly exhibits anti-tumourigenic effects, as demonstrated by its common use in treating different malignancies. However, based on the literature, it is not possible to conclude whether treatment with low-dose MTX in patients with psoriasis exhibits pro-tumourigenic effects. Owing to many years of experience with MTX treatment (compared with other treatments), we do not list previous cancer as a relative contraindication for MTX treatment in patients with psoriasis. However, patients with psoriasis have an increased risk of non-melanoma skin cancer, and annual screening of the skin for skin cancer is recommended when patients are being treated with all immunosuppressive drugs, including MTX.
The evidence for use of MTX in paediatric patients with psoriasis is limited to case reports and observational studies. Furthermore, MTX is not registered for paediatric psoriasis, and thus has to be used off-label. In general, a good clinical effect is demonstrated. One randomized controlled study comparing adalimumab with MTX has been conducted; however, the data have yet to be published (60). The MTX doses used in psoriasis are 0.2–0.4 mg/kg/week (~6–12 mg/m2/week), although higher doses can be used (maximum 20 mg/week) (61, 62).
Most evidence regarding the use of low-dose MTX in paediatric patients is found for rheumatic indications, especially juvenile idiopathic arthritis (JIA), juvenile dermato-myositis (JDM) and localized scleroderma (LS). The recommendations regarding the administration, monitoring, adverse events and long-term effect of low-dose MTX treatment in paediatric patients are based primarily on experiences from MTX treatment in JIA as no recommendations have yet been published in children with psoriasis. In JIA, the dosage of MTX is usually 10–15 mg/m2/week (60, 63–67).
MTX in children may be administered orally or subcutaneously. Subcutaneous administration of MTX is more often preferred in children because it has fewer side-effects and allows administration of higher doses. Furthermore, the bioavailability is higher and more stable (68). In dermatology, it is common practice to monitor children via blood samples prior to initiation, weekly for 4 weeks after treatment start and then every other week up to week 8. When the paediatric patient is on a stable dose, laboratory tests should be similar to those recommended for adult patients (Table I) (69). However, use of PIIINP is difficult in paediatric patients because it increases during growth (70). Similar to adults, the adverse events most commonly associated with low-dose MTX treatment are nausea, vomiting and elevated liver enzymes (60). As in the treatment of adult patients, it is recommended to prescribe 5 mg folic acid (71).
In general, low-dose MTX is safe both in the short and the long term. It has not been found to affect growth nor fertility, nor has it been proven to be associated with malignancies (60, 72).
The evidence regarding the use and safety of low-dose MTX in paediatric patients is limited and based mostly on JIA studies. In general, doses of 0.2–0.4 mg/kg/week for the treatment of psoriasis and close monitoring are recommended in paediatric patients with psoriasis. Treat-ment with low-dose MTX is effective and seems not to affect growth or fertility or to be associated with an increased risk of malignancies.
This report was based on an expert meeting. It is hoped that it will provide further consensus regarding the use and monitoring of MTX treatment in patients with psoriasis in Denmark and other countries. In general, the recommendations given above are in line with the European S3-Guidelines.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize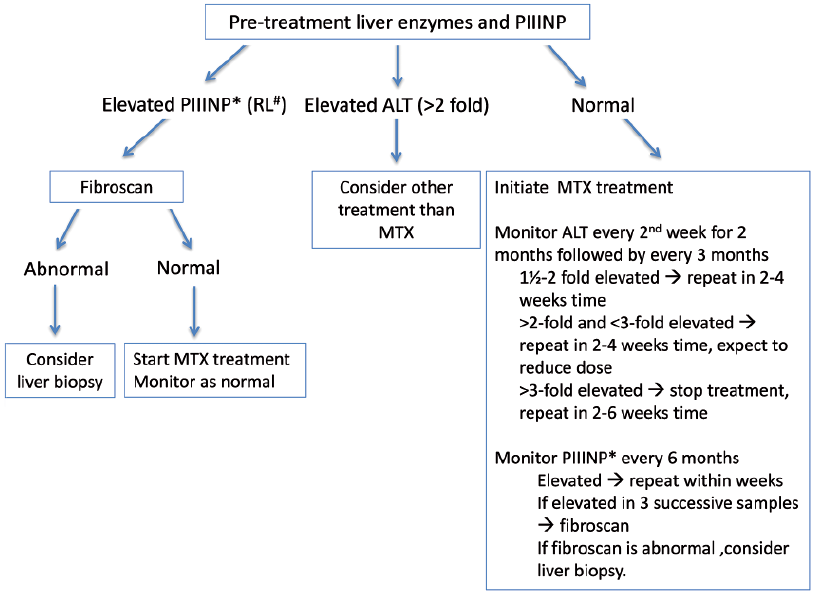 Click to show fullsize
Click to show fullsize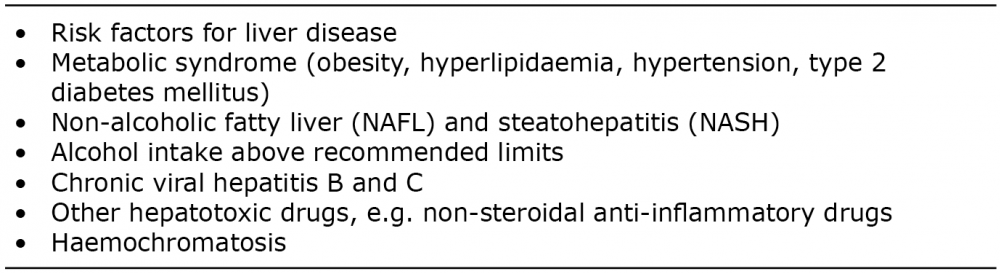 Click to show fullsize
Click to show fullsize