


1Department of Dermato-Allergology, and 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: peter.jensen@regionh.dk
Accepted Dec 15, 2016; Epub ahead of print Dec 16, 2016
Psoriasis is a prevalent, chronic systemic inflammatory skin disease, affecting approximately 2–3% of the general population; more than 125 million people worldwide (1). While 6–40% of patients with psoriasis develop psoriasis arthritis (PsA), psoriasis has also been associated with a host of autoimmune diseases, including vitiligo, multiple sclerosis, rheumatoid arthritis and inflammatory bowel disease; partly explained by shared genetic risk variants (2–4). Recently, we conducted a nationwide cohort study in Denmark, and showed that the incidence rate ratio for autoimmune hepatitis was increased 2–3-fold in persons with psoriasis (5). In 2012, Wu et al. (4), conducted a retrospective cohort study including 25,341 individuals with psoriasis and/or PsA and showed that patients with psoriasis were more likely to have at least 2 other autoimmune diseases compared with healthy controls. Given the associations between psoriatic disease and a number of autoimmune conditions, an increased prevalence of psoriatic disease among members of the Danish National Addison’s Disease Advocacy group (unpublished observation), and the limited available data on the association between primary adrenal insufficiency (PAI) and psoriasis, we conducted a nationwide case-control study to examine a potential association between these conditions.
Study approval was obtained from the Danish Data Protection Agency (ref. 2007-58-0015, int. ref. GEH-2014-018, I-Suite 02736). Review by an ethics committee is not required for register studies in Denmark. Conduct of this study was in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology recommendations (6).
The Danish National Health Service provides universal tax-supported healthcare, guaranteeing unrestricted access to general practitioners and hospitals and partial reimbursement for prescribed medications. Information on date of birth, sex, and date of death are available from the Civil Personal Register (7). The Danish National Patient Register contains data on admission and discharge dates and discharge diagnoses from all non-psychiatric hospitals since 1977 and on emergency room and outpatient clinic visits since 1995 (8). The International Classification of Diseases (ICD)-8 codes were used until the end of 1993. From 1994, the Danish adaptation of ICD-10 was implemented, whereas ICD-9 was never used in Denmark. Statistics Denmark records information on tax-reported household income (9).
All Danish patients with a first-time hospital diagnosis of primary adrenal insufficiency (ICD-10 codes E27.1A and E27.2) between 1 January 1997 and 31 December 2012 were identified. Each case was matched on age, sex, and date of diagnosis with 5 healthy controls. That is, control subjects had to be alive, resident in the source population, and at risk for first hospital admission for PAI at the time the corresponding case was diagnosed. We defined the index date of control subjects as the date of first PAI diagnosis for the corresponding case. Using this risk set sampling design, the case-control odds ratio (OR) provides an unbiased estimate of the corresponding incidence rate ratio. We identified all patients in this cohort with psoriasis and PsA. Patients were classified with severe disease when they received systemic anti-psoriatic therapy consistent with severe disease (biological drugs, cyclosporine, psoralens, retinoids, or methotrexate). We have previously described and validated the method for identification of psoriasis, and classification of severity, with a sensitivity of 98% (10).
SAS version 9.4 (SAS Institute Inc. Cary, NC, USA) and STATA version 11.2 (StataCorp, College Station, TX, USA) were used to compute case-control ORs with 95% confidence intervals (95% CIs), based on conditional logistic regression (11). This model inherently adjusts for the matched factors, and we also adjusted the models for differences in socio-economic status and smoking history, respectively. Socio-economic status was calculated as an index between 0 and 4 based on the average gross annual income (standardized by age) during a 5-year period before the index date. A 2-tailed p-value < 0.05 was considered statistically significant.
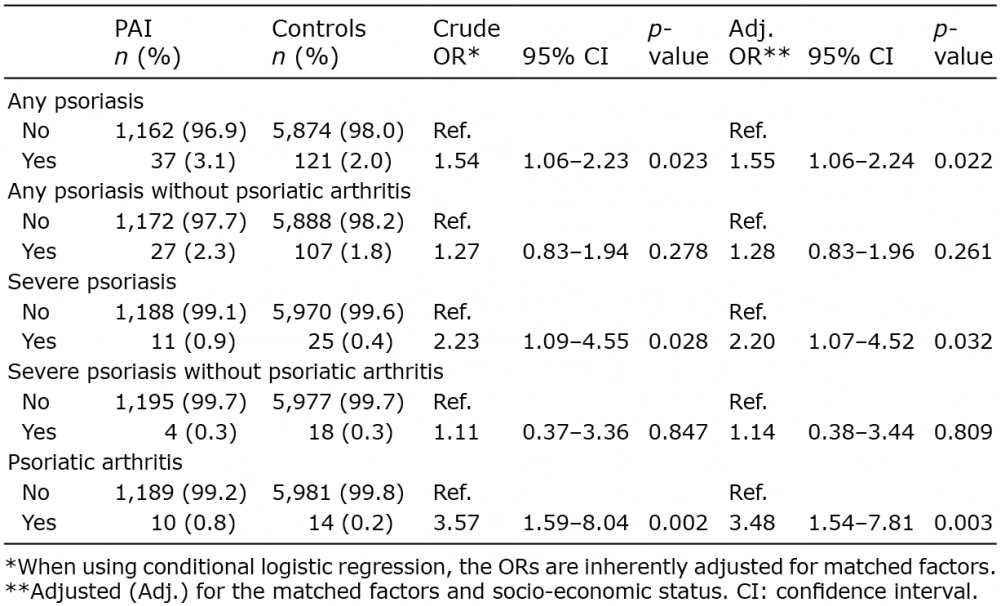
The study population included 1,199 individuals with PAI and 5,995 matched control subjects between 1 January 1997 and 31 December 2012 (65% women and mean age 52.8 years in both groups). Smoking was twice as common in PAI as in control subjects (15.4% vs. 7.8%, but the mean socioeconomic status was similar (1.9 vs. 2.0). In individuals with PAI, the adjusted ORs were 1.28 (0.83–1.96, p = 0.261) for any psoriasis (psoriasis regardless of severity) without PsA, 1.14 (0.38–3.44, p = 0.809) for severe psoriasis without PsA, 3.48 (1.54–7.81, p = 0.003) for PsA only, and 2.2 (1.07–4.52, p = 0.032) for severe psoriasis with or without PsA (Table I). When we examined the temporal relationship, i.e. whether psoriatic disease preceded PAI, or vice versa, fully adjusted ORs of pre-existing psoriasis were 1.64 (1.08–2.49, p = 0.021), whereas the OR of psoriasis onset after PAI was 1.22 (0.53–2.83, p = 0.636), as shown in Table II.
Table I. Odds ratios (ORs) associating primary adrenal insufficiency (PAI) with psoriasis or psoriatic arthritis
Table II. Odds ratios (ORs) of psoriasis and psoriatic arthritis before/after diagnosis of primary adrenal insufficiency (PAI)
In this population-based study, PAI was significantly associated with pre-existing PsA, but not psoriasis, when compared with matched controls. The explanation for the association is unclear, but a potential mechanistic link could be mediated by dysregulated tissue resident memory T cells (TRM), which reside long-term in peripheral tissues (2). TRM probably evolved to supply epithelial barriers throughout the body with protective T cells with the ability to react to pathogens most relevant in their respective tissues (12). TRM play a key role in the pathogenesis of psoriasis and other autoimmune conditions associated with psoriasis (12). Furthermore, autoimmune diseases share a large proportion of their genetic background and it has been shown that many diseases have more than 50% of their associated loci in common with another disease (2). This is further supported by the fact that the relative risk of developing an autoimmune disease is increased in children of patients with an autoimmune disease (13). Along this line, there are important genetic differences between psoriasis and PsA, which may explain the somewhat differing results observed in these two groups (14).
Several strengths and limitations apply when interpreting the results of our study. Limitations include the observational nature of the study and possible influence of unknown confounders. While PAI is a rare disease, the population-based setting employed here enables analysis of a large number of individuals with complete follow-up. Since pre-existing psoriasis was not associated with an increased risk of PAI, surveillance bias is unlikely to have markedly influenced our results, and the exclusion of secondary adrenal insufficiency limited bias, e.g. due to treatment with systemic glucocorticoids. Also, nationwide databases allow us to analyse a large number of patients with minimal selection bias. The complete registration, the prospective nature of prescription data, the ICD diagnostic codes, and the use of validated information on exposure and outcome measures ensure that recall bias and bias caused by non-response are minimized. Although, the mechanisms underlying the relationship between PsA and PAI, as well as the potential clinical implications, remain to be established, these findings add to the growing body of evidence of comorbidities associated with PsA.
Disclosures: LS has received consultancy and/or speaker honoraria from Abbott, Pfizer, Janssen-Cilag, MSD, and Leo Pharma. LS is a member of the advisory boards of MSD, Novartis, Eli Lilly and Co., Abbvie, Celgene, Amgen, and Janssen-Cilag. PJ has received speaker honoraria from Abbvie, Pfizer, and Janssen-Cilag. AE has received research funding and/or consultancy honoraria from Pfizer, Eli Lilly and Co.


 Click to show fullsize
Click to show fullsize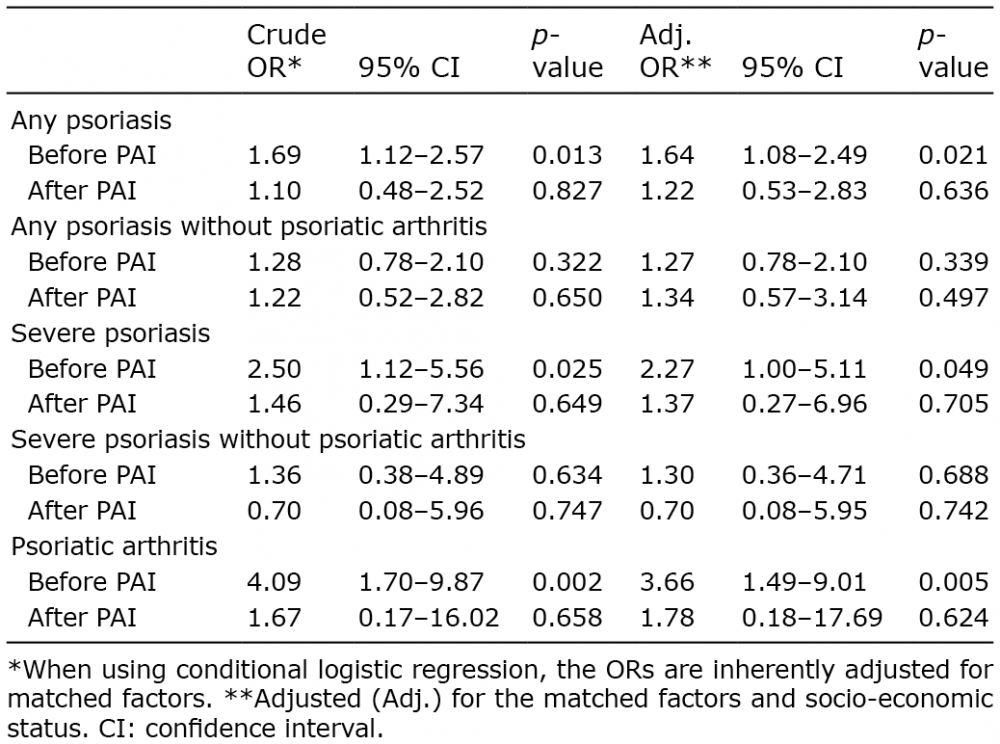 Click to show fullsize
Click to show fullsize