


1Department of Dermatology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Sugitani 2630, Toyama 930-0194, 2Department of Dermatology, Ishikawa Prefectural Central Hospital, Ishikawa, and 3Department of Dermatology, National Hospital Organization Kanazawa Medical Center, Kanazawa, Japan. E-mail: tmakino@med.u-toyama.ac.jp
Accepted Dec 15, 2016; Epub ahead of print Dec 16, 2016
Dermatitis herpetiformis (DH) is a pruritic papulovesicular disease that is symmetrically distributed over the shoulders, elbows, back and knees. Immunofluorescence has revealed granular IgA deposition in the papillary dermis. IgA antibodies to both epidermal transglutaminase (eTG) and tissue transglutaminase (tTG) are usually detected in patients with DH. DH is commonly thought to be a cutaneous manifestation of gluten-sensitive enteropathy (GSE) (1, 2). We refer to this condition as “granular-type DH”. Although DH is a relatively common disease in Caucasian populations, it is rare in Japan. Most Japanese patients with DH show unique features, including a high frequency of fibrillar IgA deposition in the papillary dermis, rare occurrence of GSE, absence of the HLA-DQ2/DQ8 haplotype and rare associations with autoimmune disease and lymphoma, although the histological findings appear to be similar to those of granular-type DH (3, 4). Furthermore, as reported previously, these patients appear to have IgA antibodies to eTG, but not tTG (5). We refer to this condition as “fibrillar-type DH”. The clinical and histological findings of typical fibrillar-type DH are shown in Fig. S1. Fibrillar-type DH appears to be rare in Caucasian populations (6). While the pathogenesis of DH is unclear, previous studies have suggested that the expression of interleukin (IL)-8, granulocyte-macrophage colony-stimulating factor (GM-CSF) and Th2-type cytokines could be important in the tissue infiltration process of eosinophils and neutrophils in granular-type DH (7, 8). The present study investigated the levels of serum cytokines and chemokines in order to clarify their presence and activity in the pathogenesis of fibrillar-type DH.
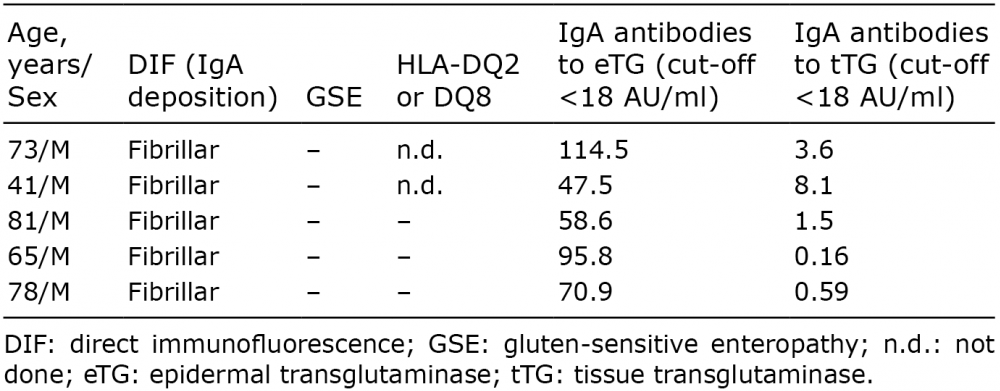
The study population included 5 patients with fibrillar-type DH (mean age 67.4 years; age range 41–81 years) in the active stage of the disease, who had not received any treatment and in whom the development of new lesions had been observed (Table I). The levels of IgA antibodies against eTG were markedly increased in all patients. However, no IgA antibodies against tTG were detected in any of the patients. None of the patient’s intestinal tissue specimens showed villous atrophy or lymphocytic cell infiltration.
Table I. Characteristics of study patients with fibrillar-type dermatitis herpetiformis
The serum level of interferon (IFN)-γ, a Th1-like cytokine, was increased slightly in the patients with DH (mean 0.414 ± 0.23; range 0.21–0.80 pg/ml) in comparison with the control subjects; however, the difference was not statistically significant. IL-12, another Th1-like cytokine, was not detected in either the patients with DH or the control subjects (Fig. S2a).
The patients’ serum levels of Th2-like cytokines IL-4 (mean14.55 ± 5.3 pg/ml; range 6.84-21.71 pg/ml, p < 0.005), IL-5 (mean 6.09 ± 0.99 pg/ml; range 4.84–7.49 pg/ml, p < 0.001) and IL-13 (mean 1.14 ± 0.20 pg/ml; range 0.85–1.36 pg/ml, p < 0.005) were significantly increased in comparison with the normal subjects: IL-4: mean 0.04 ± 0.09 pg/ml; range 0-0.21 pg/ml, IL-5: mean 0.55 ± 0.14 pg/ml; range 0.37–0.72 pg/ml, IL-13: mean 0.21 ± 0.09 pg/ml; range 0.08–0.29 pg/ml, respectively (Fig. 1 and Fig. S2b).
Fig. 1. Increased serum levels of cytokines IL-4 and IL-5 in patients with fibrillar-type DH. Values are shown as mean ± standard deviation. *p < 0.005; **p < 0.001.
The serum IL-8 level in the patients with DH (mean 39.4 ± 43.5; range 1.1–93.81 pg/ml) tended to be increased in comparison with the control subjects (mean, 0.26 ± 0.59 pg/ml; range 0–0.32 pg/ml), although not statistically significant. The serum level of eotaxin in the patients with DH (mean 66.65 ± 31.3; range 35.3–114.0 pg/ml; p < 0.05) was significantly higher than that in the control subjects (mean 11.23 ± 2.70 pg/ml; range 7.76–13.81 pg/ml) (Fig. S2c).
Serum levels of Th2-type cytokines, including IL-4, IL-5 and IL-13, as well as eotaxin were found to be elevated in fibrillar-type DH. IL-4 plays a role in eosinophilic recruitment in the tissue by promoting eosinophilic transmigration from the vascular endothelium (9). IL-5 induces the apoptosis of eosinophils and the release of
eosinophil granules (10). Eotaxin is an eosinophil attractant that is increased under conditions associated with tissue eosinophilia (11). In addition, IL-4 and IL-13 mediate the production of eotaxin and modulate eosinophilic infiltration in immunological reactions (12). The T-cell-mediated immune response is thought to be associated with the pathogenesis of granular-type DH, because the CD4-positive T-cell infiltrated in the skin lesions of DH patients seems to act mainly through the production of Th2-type cytokines, such as IL-4, IL-5 and IL-13 (8). However, a significant increase in the serum levels of Th2-type cytokines was not observed in patients with granular-type DH (13). These findings further suggest that IL-4, IL-5, IL-13 and eotaxin may be important in the development of skin lesions, especially in the tissue infiltration process of eosinophils, in fibrillar-type DH.
Serum levels of IL-8, a chemokine that acts as a neutrophil chemoattractant and mediates the function of neutrophils, have been reported to be elevated in patients with granular-type DH (7). In this study, we observed increased serum levels of IL-8 in 3 out of the 5 patients with fibrillar-type DH; however, the difference was not statistically significant. The precise correlation between the IL-8 levels and fibrillar-type DH should be examined after the accumulation of more cases. In addition, the ability to control the inflammation associated with granular-type DH by strict adherence to a gluten-free diet suggests that the mucosal immune response plays a critical role in the pathogenesis of the skin lesions (14, 15). However, GSE is not normally observed in patients with fibrillar-type DH. Thus, further research will be needed to clarify the trigger for the creation of the Th2-type cytokine profile in circulating inflammatory cells. The number of patients included in the present study was low because of the rarity of fibrillar-type DH. The mechanism and pathogenesis of fibrillar-type DH should be elucidated with the accumulation of a greater number of cases.
This research was supported by a Grant-in-aid numbers 20591337 and 23591639 from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize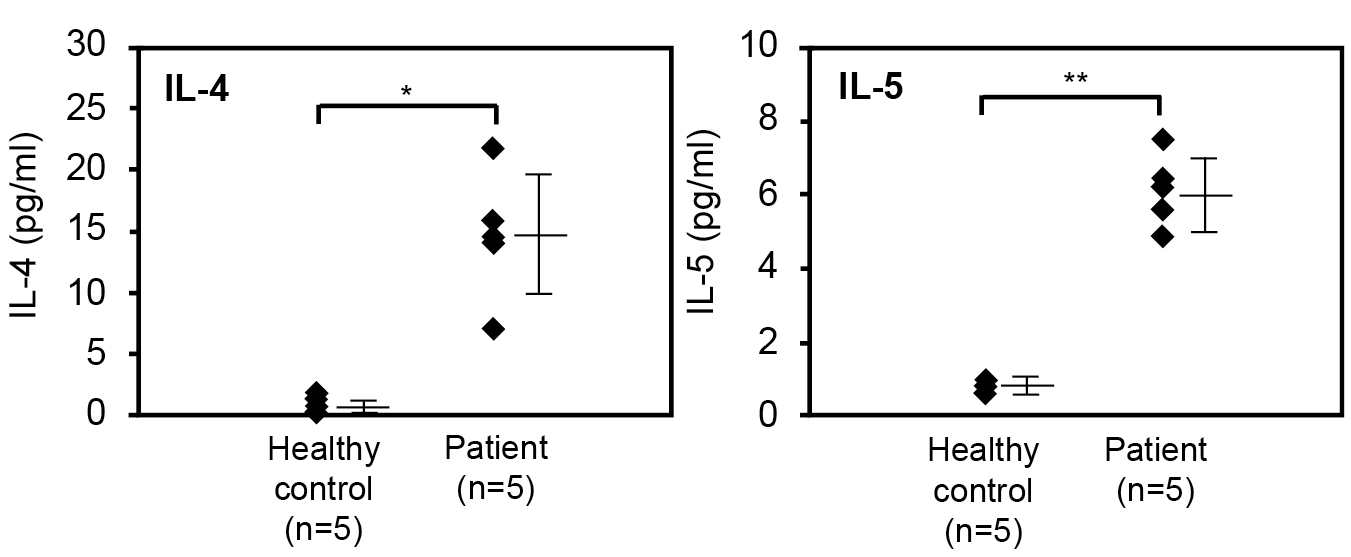 Click to show fullsize
Click to show fullsize