


1Faculty of Continuing Education, 2Institute of Anatomy and Anthropology, and 3Department of Infectology and Dermatology, R?ga Stradi?š University, Dzirciema Street 16, LV-1007 Riga, Latvia. E-mail: ieva.sauliite@gmail.com
Accepted Dec 15, 2016; Epub ahead of print Dec 16, 2016
Despite persistent exposure to microbial agents, the nail unit appears to be capable of ensuring efficient innate immune defence. In the human nail, antimicrobial peptides (AMPs), which are small molecules with a broad spectrum of innate defence properties, may play an important role (1, 2). Although the specific arrangement of the nail’s immune components is poorly understood, one could speculate that a well-developed immune defence may require the correct expression and localization of AMPs. Nevertheless, the exact contribution of AMPs both in homeostasis and disease has yet to be defined.
In psoriatic skin plaques, the levels of several AMPs are reported to be highly upregulated (3). Furthermore, AMPs of the cathelicidin and defensin groups are suggested to be decisive players in psoriasis pathogenesis (3, 4). Hence, based on data from plaque psoriasis studies, one could hypothesize AMP upregulations in nails with psoriasis and that AMP upregulation would result in decreased secondary infections. However, in nail psoriasis, an increased coincidence of onychomycosis has been reported (5, 6).
Because the exact consequences of psoriatic inflammation in the nail unit are unknown and might differ from the ones described in the skin (7), we evaluated the AMP profile in the human nail apparatus. Specifically, we determined the presence and distribution of AMPs of the cathelicidin (LL-37) and beta defensin (hβD-2, hβD-3 and hβD4) groups in psoriatic nail apparatus specimens and compared them to clinically normal nails.
The patient group with nail psoriasis included 20 patients (18 to 70 years of age). Nail unit tissue specimens (5 mm in diameter) were obtained from the nail bed using a punch biopsy technique. Inclusion criteria were: i) a clinical diagnosis of nail psoriasis with nail bed involvement (8, 9); ii) a pathohistological diagnosis of nail psoriasis (8).
For the control group, 26 necropsies from human cadaver nail units (nail bed and nail matrix) were obtained (within 12 h of the death) and included for further evaluation. Only nail apparatuses with normal clinical and pathohistological appearance were included in the study. Exclusion criteria for both groups included: i) the presence of any disease in the medical history that might affect nails (except psoriasis in the psoriatic nail group); ii) a positive Periodic acid-Schiff (PAS) reaction and/or fungal culture of the nail sample; iii) history of any local or systemic anti-bacterial, anti-fungal, anti-inflammatory, immunosuppressive, or immunomodulating treatment received within the last month.
Immunohistochemistry. Four µm sections of paraffin-embedded nail biopsy specimens were treated with antibodies for LL-37 (rabbit; 1:200; Biorbyt, UK), hβD-2 (goat; 1:100; Bio-Techne, UK), hβD-3 (rabbit; 1:1000; Novus Biologicals, USA) and hβD-4 (mouse; 1:100; Santa Cruz Biotechnology, USA) (10). Immunostaining was assessed semi-qantitatevly by grading the stained cells in the visual field (11). Non-parametric statistics using the Mann-Whitney U-test display the ranking differences between the control group and studied group.
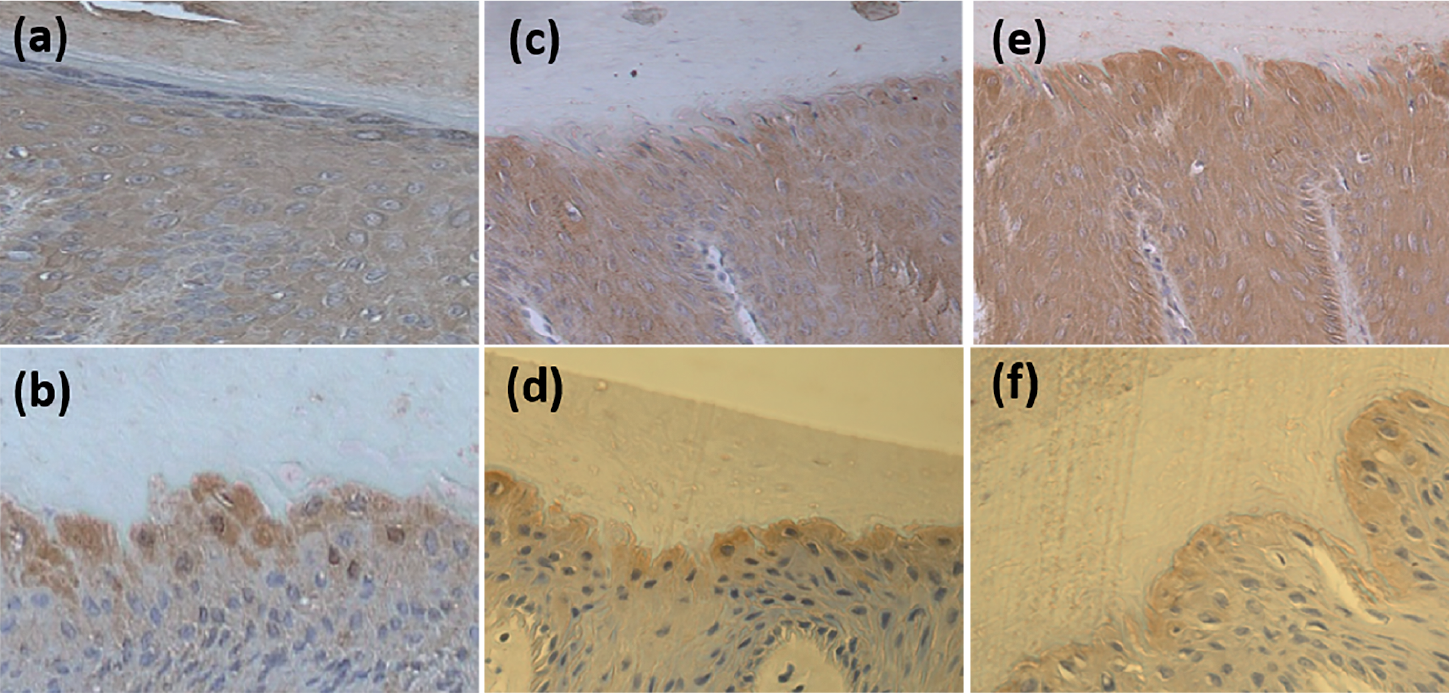
In both the psoriatic and control groups, we observed LL-37 positive cells; however, more positive cells were present in nail psoriasis samples. In psoriasis-affected nails, numerous (+++) positive cells were observed in the epithelial layer of the nail bed. Interestingly, in the control group, only moderate (++) numbers of LL-37 positive cells were present (Fig. 1 a and b; Table I). Further, in the control group samples, LL-37 immunoreactivity was evenly distributed throughout the nail unit, including proximal and distal nail matrixes.
Fig. 1. Detection of antimicrobial peptides by immunohisto-chemistry in psoriatic nail beds (a, c, e) compared to contrlos (b, d, f). (a) Abundance of LL-37-positive cells in the psoriatic nail bed and (b) a moderate number of LL-37 positive cells in the control nail bed; numerous and moderate numbers of hBD-2 positive cells were observed in psoriatic (c) and control nail beds (d); numerous hBD-3 positive cells were detected in psoriatic (e) and few in control nail beds (f) (original magnification: X250).
Table I. Detection of LL-37, hβD-2, hβD-3, and hβD-4 in psoriasis-affected and control nail bed by immuno-histochemistry
In psoriatic nails, cells positive for hβD-2 and hβD-3 were observed in nail bed epithelia. The number of positive cells varied from numerous (+++) to abundant (++++) in the visual field (Fig. 1 c and e). Moderate (++) numbers of hβD-2 and hβD-3 positive cells were found in the control group’s nail bed (Fig. 1 d and f) and a patchy distribution of positive cells was observed near the nail plate. In contrast, in psoriatic nails, expression was evenly distributed throughout the nail bed. Notably, more hβD-2 and hβD-3 positive cells were observed per visual field of the psoriatic nail samples. Cells positive for hβD-4 staining were not observed in either psoriatic and control group nails (Table I).
In our study, all nail specimens affected by chronic psoriatic inflammation had significantly more LL-37, hβD-2 and anti-hβD- 3 positive cells when compared to the control group samples. These findings are consistent with previously described increases in AMPs in psoriatic skin lesions, particularly LL-37 and hβD-2, by other authors (2, 4). Moreover, the role for LL-37 as an autoantigen in psoriasis patients is supported by the presence of cytokine-producing LL-37-specific T cells found in plaque psoriasis (4, 12). However, to our knowledge, the expression and distribution of AMPs in nail units affected by psoriasis have not been previously described. Therefore, taking into account the observed increase in the number of LL-37 positive cells in psoriatic nails in our study, we suggest that LL-37 is characteristic for nail psoriasis. Furthermore, we speculate that LL-37 may be of particular importance not only for inducing the psoriasis-related inflammation but also for the persistence of psoriasis-related inflammation in nail unit due to either excessive and/or perpetual exposure of the nail apparatus to microbial and fungal agents.
We observed LL-37 positive cells throughout the healthy control group’s nail bed as well as both proximal and distal matrixes. Previously, LL-37 and hβD-2 have been reported in the healthy nail apparatus (1, 13). Further, we found that expression of hβD-2 and hβD-3 in control nails was predominantly found at sites directly exposed to fungal and microbial agents such as the nail plate. These findings suggest that, along with LL-37, AMPs of the defensin group are expressed in the healthy human nail unit. Importantly, we provide evidence that AMPs in the nail apparatus might contribute to the relative immune privilege of the nail matrix (14). AMPs expressed in the nail apparatus may help to promote an effective defence in the presence of continuous exposure to various microbiologic agents.
Additionally, we propose that the perceived coincidence of psoriasis and onychomycosis might be over-estimated. Despite the lack of cellular immune components in the nail plate, nail units may ensure defence against infections by upregulating the expression of AMPs. Furthermore, we suggest that the elevated numbers of hβD-2 and hβD-3 positive cells in the nail apparatus of people affected by psoriasis may also contribute to the specific expression pattern of AMPs. By determining the distinctive expression pattern of AMPs in human nails affected by psoriasis, we can enhance our understanding of psoriatic nail disease and rationally develop targeted treatment options to interfere with AMPs, while avoiding unnecessary immunosuppressive consequences.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize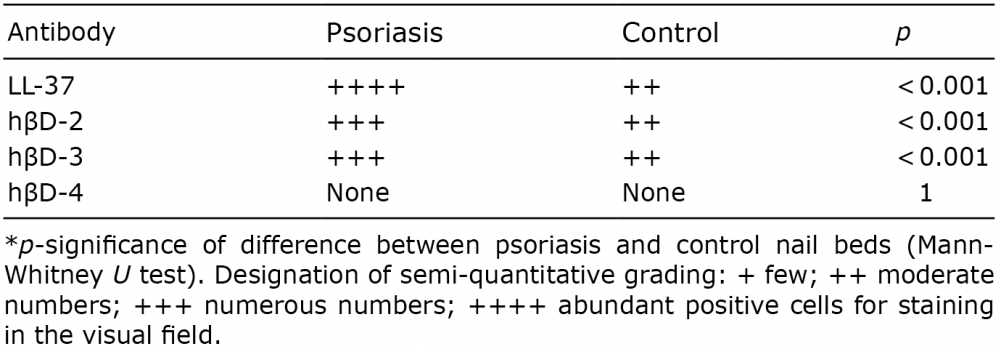 Click to show fullsize
Click to show fullsize