


1Department of Dermatology and Allergology, University of Szeged, Szeged, Hungary, 2National Center for Dual Diagnosis, Innlandet Hospital Trust, Brumunddal, Norway, 3Department of Dermatology, Universite Libre de Bruxelles Erasme Hospital, Brussels, Belgium, 4Department of Dermatology, Justus Liebig University, Giessen, Germany, 5Department of Psychology, University of Zaragoza, Aragon Health Sciences Institute, Zaragoza, Spain, 6Institute of Medical Psychology, Justus Liebig University, Giessen, Germany, 7Department of Dermatology, Zealand University Hospital, Roskilde, Denmark, 8Department of Dermatology, University Hospital of Brest, Brest, France, 9Oslo Center for Biostatistics and Epidemiology, University of Oslo, Oslo, Norway, 10Clinical Epidemiology Unit, Istituto Dermopatico dell’Immacolata (IDI)-IRCSS FLMM, Rome, Italy, 11Health, Medical and Neuropsychology unit, Faculty of Social and Behavioural Sciences, Leiden University, Leiden, The Netherlands, 12Department of Dermatology, Oslo University Hospital, 13Institute of Clinical Medicine, University of Oslo, Oslo, Norway, 14Department of Dermatology, Stavanger University Hospital, Stavanger, Norway, 15Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, 16Department of Psychiatry and Psychosomatics, I. M. Sechenov First Moscow State Medical University, Moscow, Russia, 17Department of Dermatology, Alcaniz Hospital, Alcaniz, Spain, 18Department of Dermatology and Venereology, Sisli Hamidiye Etfal Teaching and Research Hospital, Health Sciences University, ?i?li-Istanbul, Turkey, 19Department of Dermatology, Cardiff University School of Medicine, Heath Park, Cardiff, UK, 20Department of Pharmacy, Pharmacology and Postgraduate Medicine, The School of Life and Medical Sciences, University of Hertfordshire, Hatfield, UK, and 21Department of Dermatology and Venereology, Skåne University Hospital, Lund University, Malmö, Sweden
Attachment styles of dermatological outpatients and satisfaction with their dermatologists were investigated within the framework of a multicentre study conducted in 13 European countries, organized by the European Society for Dermatology and Psychiatry. Attachment style was assessed with the Adult Attachment Scale. Patient satisfaction with the dermatologist was assessed with an 11-degree scale. A total of 3,635 adult outpatients and 1,359 controls participated in the study. Dermatological outpatients were less able to depend on others, were less comfortable with closeness and intimacy, and experienced similar rates of anxiety in relationships as did the controls. Participants who had secure attachment styles reported stressful life events during the last 6 months significantly less often than those who had insecure attachment styles. Patients with secure attachment styles tended to be more satisfied with their dermatologist than did insecure patients. These results suggest that secure attachment of dermatological outpatients may be a protective factor in the management of stress.
Key words: psychodermatology; attachment styles; satisfaction.
Accepted Jan 24, 2017; Epub ahead of print Jan 25, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Csanád Szabó, Department of Dermatology and Allergology, University of Szeged, Korányi fasor 6, HU-6720 Szeged, Hungary. E-mail: szabo.csanad@med.u-szeged.hu
Attachment can be defined as an emotional bond that develops within the context of the early interactions between infants and their primary caregivers (1). Attachment towards caregivers has an effect on later interpersonal expectations, emotions, and behaviours towards significant others (2). Attachment style relates to the way people behave in close relationships, which, in turn, is linked to well-being, due to a positive association between social support and health (3–5).
Three different attachment styles were categorized by Ainsworth et al. (6); secure attachment, and 2 types of insecure attachment: anxious-ambivalent, and avoidant. These different attachment styles can be defined by attributes of 3 dimensions of attachment: comfort with closeness (closeness), capacity to depend on others (dependency), and fear of being abandoned (anxiety in relationships) (7). Securely attached people find it relatively easy to get close to others and are comfortable depending on them; they do not often worry about being abandoned. Individuals with avoidant attachment style are somewhat uncomfortable being close to others; they find it difficult to allow themselves to depend on others, and they are nervous when anyone gets too close to them. People who have an anxious-ambivalent attachment style find that others are reluctant to get as close as they would like, and they often worry that their partner “does not really love them” or does not want to stay with them (2). In a large representative sample of American adults the distribution of adult attachment styles was 59% secure, 25% avoidant, and 11% anxious (8).
Secure attachment probably results in beneficial psychological health attributes. Patients with insecure attachment styles tend to report a greater number of physical symptoms compared with secure individuals (9). A secure attachment style might be an important inner resource in emotional adaptation to chronic diseases (10). The prototype of secure attachment is characterized by a valuing of intimate friendships, the capacity to maintain close relationships without losing personal autonomy, and a coherence and thoughtfulness in discussing relationships and related issues (11). Insecure attachment has been linked to higher depressive and anxiety scores compared with secure individuals (12). Avoidant attachment was correlated with subjective depression and hopelessness point scores in a study by Grunebaum et al. (13). Kuscu et al. (14) reported a positive correlation between anxious-ambivalent attachment scores and the level of state anxiety. Attachment styles are related to point scores of somatization, hypochondria and coping skills (15).
A model with more insecure categories is in use by current researchers. The theory of Bartholomew & Horowitz (11) consists of 4 styles of adult attachment. According to their model attachment styles vary along 2 dimensions: a model of the self and a model of others, and both of these models can be positive or negative (11). Secure attachment style represents a sense of lovability and the expectation of others to generally be accepting and responsive. Preoccupied attachment style implies a sense of unlovability and a positive evaluation of others. Dismissing attachment style represents a sense of lovability with a negative disposition toward others. Fearful attachment style implies a sense of unlovability and a negative evaluation of others (16).
There are very few studies of attachment style in dermatology. One study, of patients with atopic dermatitis, showed that attachment insecurities were associated with greater detriment to dermatological life quality and greater symptom severity (17). Another study, of patients with chronic urticaria, showed that insecure attachment styles correlated positively with alexithymic trait scores and negatively with quality of life values (18). Attachment patterns play an important role in psychological intervention (17).
Attachment can be a protective factor in the management of stress. Psychosocial and psychiatric factors may be predisposing and maintaining factors of skin diseases, or may be a result of experiencing these conditions (19). One of these factors is psychosocial stress (everyday life stressors, stressful live events and psychological traumas). This makes the management of emotional stress an essential part of the treatment of dermatological diseases. Attachment insecurity is associated with distinctive physiological responses to stress; these include responses involving the hypothalamic-pituitary-adrenal (HPA), sympathetic-adrenal medullary (SAM) and immune systems (20). Secure attachment is related to greater reductions in state anxiety levels following exposure to stress (21). Individuals with secure attachment patterns feel competent in their ability to regulate affect in stressful situations with others, unlike people with insecure attachment styles (22). According to Hunter & Maunder (23) attachment theory provides a simple and pragmatically useful model for understanding the particular ways that individuals can feel and react when stressed by illness, and how the professional may help in the management of that distress. The internal working model of a securely attached individual includes an expectation that help will be sufficient, and that medical personnel can be trusted for support during the crisis (23).
Attachment style influences not only close relationships, but also the way in which patients relate to the clinical staff, which has an impact on their satisfaction with their care. In the establishment of outpatient satisfaction the interpersonal skills of dermatologists are important factors (24). Patient satisfaction is an important determinant of high-quality dermatological care (25, 26).
The main objective of this study was to explore the correlation of attachment style and stress in patients with skin diseases. A further aim was to explore how attachment style plays a role in patient’s satisfaction with the dermatologist.
A multi-centre observational cross-sectional study (27) was conducted in 13 European countries, organized by the European Society of Dermatology and Psychiatry. Materials and methods have been described in detail previously (27). Patients were recruited from dermatology outpatient clinics from November 2011 to February 2013. Complete data were collected on 3,635 dermatological outpatients and 1,359 healthy controls. On one or more random days at each dermatology outpatient clinic patients were invited to join the study until a total of 250 patients was reached. Inclusion criteria were: age 18 years or older, able to read and write the official language, and not having severe psychosis. Each participant completed a questionnaire which was then handed to the research assistant prior to the clinical examination by the dermatologist. The dermatologist recorded a primary diagnosis and, where applicable, a secondary diagnosis. In each centre, a control group of at least 125 subjects was recruited via advertisement from among hospital employees at the same institution. Employees with a skin condition were excluded. The employees were informed about the study and invited to answer the questionnaire after providing written consent. The subjects were not examined clinically. Information on treated co-morbidities was self-reported.
The first part of the questionnaire recorded socio-demographic variables.
Attachment style was measured with the Adult Attachment Scale (AAS) (7), distinguishing secure and insecure attachment styles. In addition to describing the styles, point scores (ranging from 6 to 30) for 3 attachment dimensions can be calculated using the AAS: Closeness (comfort with closeness), Dependency (capacity to depend on others) and Anxiety in relationships (fear of being abandoned). Stress was assessed with the item ‘’Have you had any stressful life events during the last 6 months?’’ (yes/no). Patient satisfaction with the dermatologist was assessed on an 11-degree scale (0=not satisfied at all; 10=extremely satisfied).
Other variables assessed in the multi-centre study have been described previously (27).
Descriptive statistics, independent samples t-tests, χ2 tests, Pearson correlation coefficients, one-way analysis of variance (ANOVA), Kruskal–Wallis test and Mann–Whitney U test were performed with SPSS 22.0 software.
A total of 4,994 participants were included in the study; 3,635 adult outpatients and 1,359 controls. Their sociodemographic characteristics have been described recently (27). The most frequent skin diseases were: psoriasis (17.4%), non-melanoma skin cancer (10.9%), skin infections (6.8%), eczema (6.4%), acne (5.9%), naevi (4.9%), atopic eczema (4.5%), benign skin tumours (4.2%), hand eczema (4%), and leg ulcers (3.4%) (27).
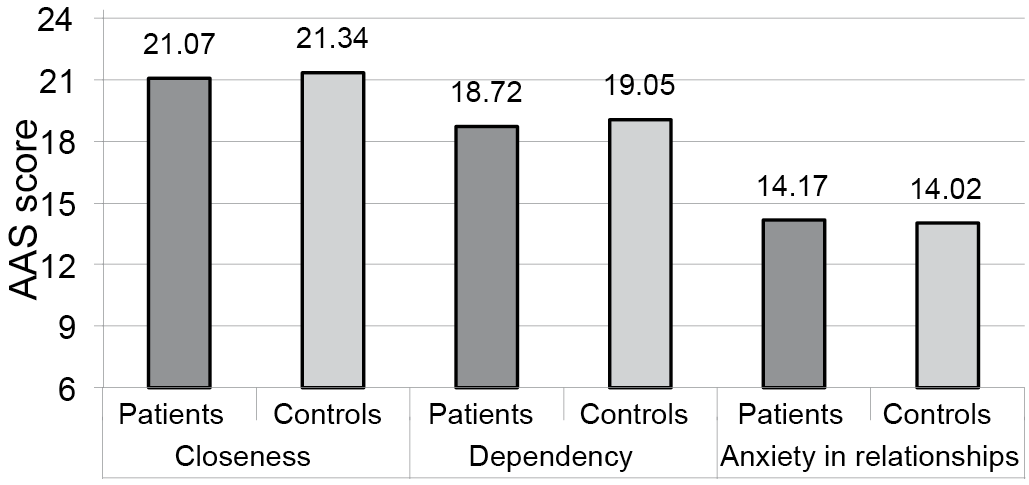
The AAS was used to assess patients and controls along 3 dimensions of attachment, and to identify each participant’s attachment style. Attachment dimension results are shown in Fig. 1. Unanswered items on the questionnaires reduced the number of participants whose attachment scores could be calculated (n = 4,320) (missing data (MD) = 674 (patients = 560; controls = 114)). The attachment scores of controls (19.05 ± 3.57) were significantly higher (t = –2.815, p < 0.01) than those of patients’ (18.72 ± 3.46) for the Dependency dimension.
Fig. 1. Means of the 3 attachment dimension scores of the Adult Attachment Scale (AAS) (scores range 6–30) (n = 4,320) (missing data = 674).
Patients’ results (21.07 ± 3.52) were significantly lower (t = –2.382, p < 0.05) than healthy volunteers’ (21.34 ± 3.3) for the Closeness dimension. Patients’ (14.17 ± 4.14) and controls’ (14.02 ± 3.93) scores did not differ significantly for the Anxiety in relationships dimension. It was possible that participants whose attachment results were missing might have different attachment patterns from those who have completed the AAS. Comparing the 2 samples we found that: there was no significant difference (χ2 = 0.886, p = 0.346) in the male/female ratio, but that the age of participants (54.51 ± 17.73) with missing attachment data was higher (t = –13.951, p < 0.01) than whose (44.13 ± 16.52) attachment data was evaluable. Age did not correlate significantly with any of the 3 AAS subscale scores.
Differences between the attachment dimensions for controls and the most frequent patient groups were examined. Among the Dependency dimension 3 patient groups had significantly lower (p < 0.05) (1-way ANOVA, post hoc least significant difference (LSD) test) point scores than controls (19.05 ± 3.57). These groups were: patients with leg ulcers (17.53 ± 3.17), benign skin tumours (18.41 ± 3.5), and psoriasis (18.56 ± 3.43). Among the Closeness dimension 2 patient groups had significantly lower (p < 0.05) (Kruskal–Wallis Test, Mann–Whitney U test) point scores than controls (21.34 ± 3.3). These groups were: patients with atopic eczema (20.59 ± 3.44) (U = 80072) and psoriasis (20.78 ± 3.55) (U = 310537). Among the Anxiety in relationships dimension none of the patient groups had point scores significantly different from controls.
Each participant’s own attachment style was identified based on the point scores they gave to items of the AAS. This method requires exclusion of individuals who do not clearly belong to any attachment style, which reduced the number of participants whose attachment style could be defined (n = 3,778) (MD = 1,216 (patients = 949; controls = 267)). There were no significant differences between patients and controls among frequencies of the 4 attachment styles (secure (68.7% vs. 69.8%), preoccupied (9% vs. 9.2%), dismissing (15.3% vs. 16.3%), fearful (6.9% vs. 4.7%)).
Participants can be divided into 2 groups, based on AAS point scores: those with secure attachment and those with insecure attachment styles. There were no significant differences between patients and controls among frequencies of the 2 attachment styles (secure (68.7% vs. 69.8%) and insecure (31.3% vs. 30.2%)).
The frequency of secure attachment style of skin patients with the most frequent diagnoses (n = 2,460) can be seen in Fig. 2. Controls had a secure attachment style more often than did patients with leg ulcers at a nearly significant level (χ2 = 3.459, p = 0.063). Controls had a secure attachment style significantly more often than did patients with psoriasis (χ2 = 3.840, p = 0.050).
Fig. 2. Percentage of patients with secure attachment style among the patients with most frequent diagnoses (n = 1,816) (missing data = 644) measured with the Adult Attachment Scale (AAS).
Patients’ mean satisfaction scores with the dermatologist were 7.58 ± 2.58. The frequency of the scores is shown in Fig. 3.
Fig. 3. Patients’ satisfaction with the dermatologist, assessed with a 11-degree scale (0 = not satisfied at all; 10 = extremely satisfied). Number of patients reporting each score (n = 3,052) (missing data=583).
Patients were classified into 4 groups according to quartiles (6, 8, 10) of their satisfaction scores: lowest satisfaction (n = 633), low satisfaction (n = 548), high satisfaction (n = 878) and highest satisfaction (n = 993) groups. Patients with secure attachment styles tended to be more satisfied with their dermatologist than did patients with insecure attachment, but the difference did not reach statistically significant levels (χ2=6.610, p = 0.085) (Table I).
Table I. Frequencies (%) of attachment styles among satisfaction categories of skin patients (n = 2,326) (missing data = 1,309) and among stressed and non-stressed patients (n = 2,661) (missing data = 974)
Patients reported stressful live events significantly more often (p < 0.01, χ2 = 10.836) than did controls (35% vs. 30%) (25). Stressed patients had insecure attachment styles (39.5%) significantly more often (p < 0.01, χ2 = 7.175) than secure styles (34.2%) (Table I). Thus, non-stressed patients had secure attachment styles (65.8%) significantly more often than insecure styles (60.5%).
A similar pattern was found in controls’ results. Stressed controls had insecure attachment styles (37.9%) significantly more often (p < 0.01, χ2 = 9.627) than secure styles (28.4%). Non-stressed controls had secure attachment styles (71.6%) significantly more often than insecure styles (62.1%).
This study shows that, compared with controls, dermatological outpatients were less able to depend on others, were less comfortable with closeness and intimacy, but experienced similar rates of anxiety in relationships as controls. Among the Dependency dimension 3 patient groups had significantly lower point scores than did controls: patients with leg ulcers, benign skin tumours and psoriasis. Among the Closeness dimension patients with atopic eczema and psoriasis had significantly lower point scores than did controls. There were no significant differences between patients and controls among frequencies of secure and insecure attachment styles. Controls had secure attachment style significantly more often than did patients with psoriasis. Feelings of shame and stigmatization of patients with psoriasis could cause avoidance of social activity and intimacy (28). The conclusion of Lahousen et al’s study of and our results also suggests that “psychological interventions should be integrated in the treatment of psoriasis” (28). The following interventions can be beneficial in the management of psoriasis: managing social isolation/withdrawal and improving self-esteem (29), applying support and education to reduce the intensity of pruritus (30), using adjunctive cognitive behavioural therapy combined with biofeedback (31), applying concepts from the life course approach to better understand the impact of chronic skin disease over the life course (32). The work of a psychodermatology multidisciplinary team (which may also include a dermatologist, a psychiatrist, a psychologist and other health professionals) has been identified as a successful way to manage patients with psychocutaneous disease (33). There is a need in psoriasis care for a comprehensive psychological and psychosomatic assessment (34).
Participants (both patients and controls) in the current study who had secure attachment styles reported stressful life events significantly less often than those who had insecure attachment styles. To our knowledge those findings are novel. Psychological stress plays an important role in triggering or exacerbating chronic skin diseases (35). In a psychotherapy session patients who have the capacity to quickly develop a secure attachment to their therapist seem more willing than patients with insecure attachment to engage in deep exploration of their issues, form an interpersonal bond with their therapist, and collaborate on the goals and tasks of therapy (36). Knowledge of this phenomenon may be useful for dermatologists and other professionals who would like to explore psychosocial stressors in chronic skin patients. It is a central feature of the therapeutic relationship that if the patient perceives a secure attachment with the therapist it enables him or her to feel safe to explore their inner conflicts without feeling ashamed or humiliated and allows him or her to experience the therapist as responsive and understanding (37).
Patients with secure attachment styles tended to be more satisfied with their dermatologist than did patients with insecure attachment styles. This finding could be important in the perspective of the doctor-patient relationship. High satisfaction of dermatology patients is related to effective communication of their dermatologists and friendliness of the care staff (38).
A limitation of our study was that we used one item to measure stress of the participants and satisfaction with dermatologists. Future studies should consider the use of more excessive stress and satisfaction inventories. Participants whose attachment results were missing (due to unanswered items in the questionnaire) might have different attachment patterns from those who have completed the AAS. There was no significant difference between their male/female ratios, but the age of those participants with missing attachment data was higher than those whose attachment data was evaluable. It was also found that age did not correlate significantly with any of the 3 AAS subscales’ scores. Therefore we can assume that the age difference between participants with evaluable attachment data and those with missing attachment data might not have had a remarkable effect on the overall attachment score of our sample. A strength of this study was that our results can be considered to be naturalistic and representative of dermatological outpatients in general.
In conclusion, this study revealed that attachment styles of dermatological patients in Europe are stronger predictors of perceived stress than the patients’ level of satisfaction with the dermatologist. It is therefore possible that the attachment results for European skin patients in this study had an effect on their consultations with their dermatologists in relationship to secure or insecure attachments to their caregivers. Further research is needed to understand the connections between stress and attachment style. This study supports the argument that when patients are securely attached in a supporting relationship or network they seem to be more protected from stress.
All participating centres declared that they accept the use of the whole data sample for the planned scientific research and publications in this ESDaP study. All participating centres have the right to use the European data following request to the core group. The numbers of complete data-sets provided by the participating European centres have been described in detail in a recent publication (27).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize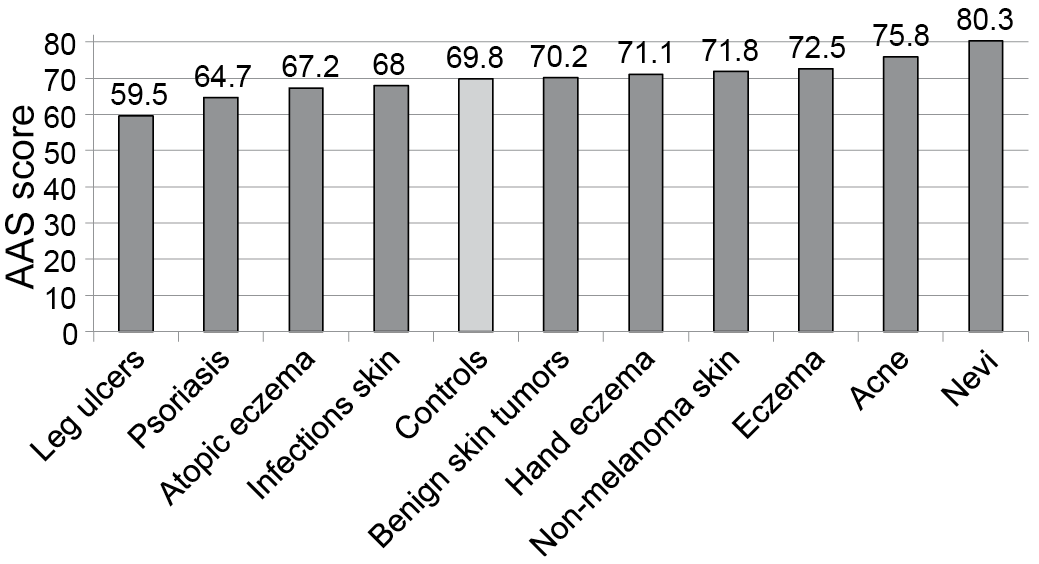 Click to show fullsize
Click to show fullsize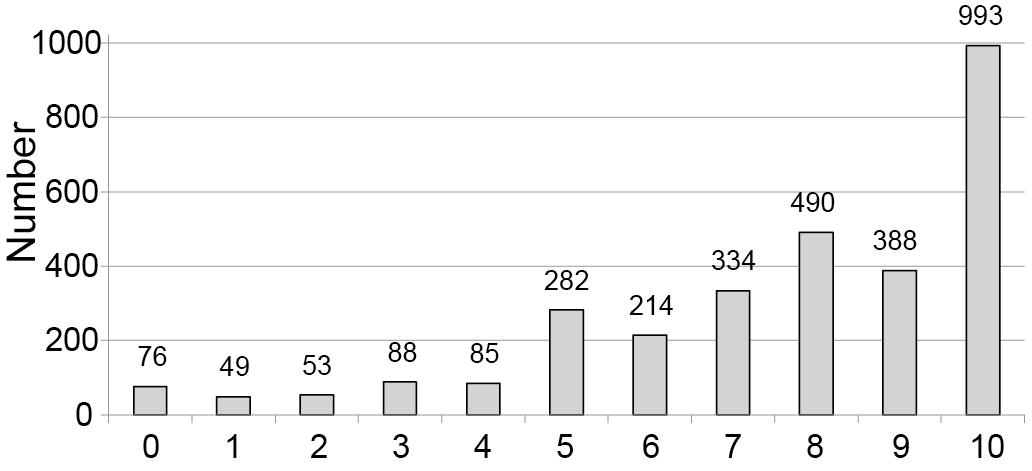 Click to show fullsize
Click to show fullsize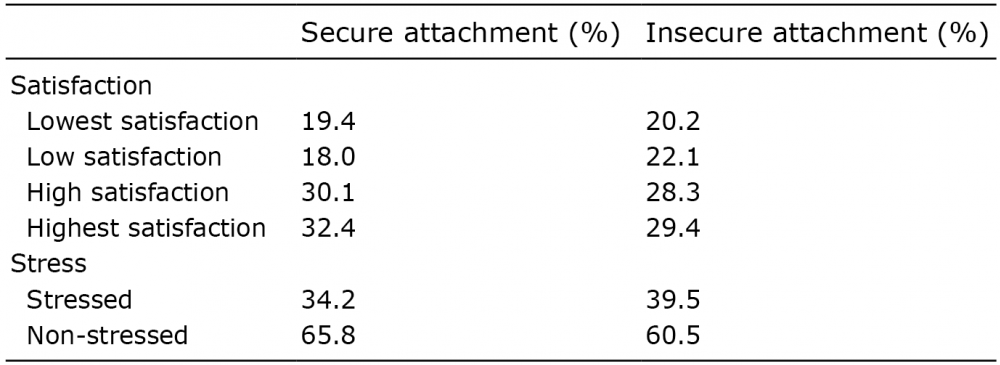 Click to show fullsize
Click to show fullsize