


1Department of Dermatology and Allergy, 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 3The Danish Heart Foundation, and 4The National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark
Adult atopic dermatitis (AD) is associated with overweight, obesity and cardiovascular diseases (CVD) in Americans, similarly to psoriasis, but no increased risk of CVD has been shown in European patients with AD. This study investigated the prevalence and risk of gallstones in adults with AD and in those with psoriasis as a proxy for obesity using nationwide data for all Danish citizens ≥ 30 years of age. Outcome was a diagnosis of gallstones. Odds ratios (ORs) were calculated by logistic regression (cross-sectional study) and hazard ratios (HRs) were estimated by Cox regression (cohort study). The study comprised 6,742 patients with AD, 53,810 patients with psoriasis, and 3,534,164 general population subjects. The prevalence of gallstones was 3.8%, 3.5% and 5.0% in the general population, AD and psoriasis patients, respectively. Adjusted ORs were 0.81 (0.71–0.92) for AD and 1.18 (1.14–1.23) for psoriasis. During follow-up, adjusted HRs were 0.72 (0.56–0.90) for AD and 1.10 (1.02–1.18) for psoriasis. The findings highlight important differences in obesity and lifestyle factors among patients with AD and those with psoriasis.
Key words: psoriasis; atopic dermatitis; BMI; obesity; gallstones.
Accepted Jan 24, 2017; Epub ahead of print Jan 25, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Alexander Egeberg, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, Denmark. E-mail: alexander.egeberg@gmail.com
Atopic dermatitis (AD) is a chronic relapsing inflammatory skin disease that affects many adults, a large number of whom will have lived with their condition since childhood (1). Well-established co-morbidities include not only food allergies, asthma and rhinitis, but also psychiatric conditions, including anxiety, depression and attention deficit hyperactivity disorder (ADHD) (2–4). However, there is growing interest in possible cardiovascular co-morbidities, since chronic low-grade inflammation could potentially increase the risk of such conditions. For example, US cohorts of adult patients with AD and eczema have found increased risks of hypertension, angina, heart attack, and stroke, as well as pre-diabetes (5, 6). Similarly, a study from Taiwan showed a dose-dependent increased risk of stroke in patients with AD (7). However, we have not been able to replicate the increased risk of cardiovascular disease (CVD) in adult Danish patients with AD (8). We have speculated that the explanation could be a difference in risk factors between the populations. Indeed, a meta-analysis showed that obesity and overweight were significantly associated with AD in American and Asian populations, but not in Europeans (9). This is in line with our clinical impression that Danish patients with AD are rarely overweight or obese. Conversely, Danish patients with psoriasis have a higher prevalence of overweight and obesity (10). In fact, obesity is significantly and independently associated with the presence and severity of psoriasis (11), probably resulting from obesity-induced systemic low-grade inflammation (12, 13). While obese patients show decreased response to anti-psoriatic therapy (14), weight loss has been suggested as a potential therapeutic option for patients with psoriasis (15, 16). Hypertension, dyslipidaemia, and diabetes also frequently occur in patients with psoriasis, and there is a high prevalence of smoking and alcohol consumption among these patients (17, 18).
Gallstones (cholelithiasis) is one of the most common medical problems leading to surgical intervention in Western countries, resulting in approximately 500,000 cholecystectomies in the US each year (19). Gallstones affect approximately 10% of the adult population in the USA, whereas in Europe, prevalence rates from 6% in Italy to 22% in Norway have been found (20, 21). While certain subtypes exist (cholesterol, brown pigment, and black pigment gallstones, respectively), in general the risk factors predisposing to gallstone formation include obesity, diabetes, dyslipidaemia, oestrogen and pregnancy, haemolytic diseases, and cirrhosis (19, 22). Moreover, while gallstones may cause subsequent inflammation of the gallbladder, inflammation itself does not appear to be a significant contributor to the development of gallstones (19).
A fundamental limitation of many large-scale registries is the lack of data on body mass index (BMI). Since gallstones are significantly associated with overweight and obesity, these may serve as a useful proxy to examine potential differences in obesity between study groups. We therefore examined the prevalence and risk of gallstones in patients with adult AD and psoriasis, compared with the general Danish population, using cross-sectional and cohort study designs.
Study approval was obtained from the Danish Data Protection Agency (ref. 2007-58-0015, int. ref. GEH-2014-018, I-Suite 02736). Approval from an ethics committee is not required for registry studies in Denmark. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations (23).
Denmark has high-quality nationwide administrative registries, in which all Danish residents can be linked at the individual level (24). The Danish National Patient Register (DNPR) (25) was established in 1978, and information on inpatient and outpatient (ambulatory) hospital consultations according to the International Classification of Diseases, 8th (ICD-8) and 10th revision (ICD-10). The validity of data from this register has been described elsewhere (26). The 9th revision was never used in Denmark. The Danish Registry of Medicinal Products Statistics (27), established in 1994, records information on all pharmacy-dispensed medications in Denmark, according to the international Anatomical Therapeutic Chemical (ATC) classification. Medication dispensed during hospitalization, or given directly from ambulatory clinics, is recorded in the DNPR. Information on tax-reported household income is recorded by Statistics Denmark (28).
The present study comprised all Danish adults ≥30 years and resident in Denmark on 1 January 2008 (i.e. the date of study start for all individuals in the cohort study). Subjects were followed from study start until 31 December 2012, death, migration, or the occurrence of an endpoint, whichever came first. Patients were classified as having adult AD if on or after their 18th birthday, but prior to the study start, they had received a diagnosis (inpatient or ambulatory) of AD by a dermatologist (ICD-8 691 and ICD-10 L20) recorded in the DNPR. Patients with psoriasis were identified by either a diagnosis of psoriasis (ICD-8 696.1 and ICD-10 L40) recorded in the DNPR, or if they had been given at least 2 prescriptions of topical vitamin D derivatives (ATC code D05AX), which is the preferred first-line treatment and used exclusively for psoriasis in Denmark. The accuracy of this method has been described elsewhere (29). At least 2 prescriptions were required to ensure persistent medical therapy. Patients were classified with severe disease if they received systemic therapy for AD (methotrexate, azathioprine, mycophenolate mofetil, systemic corticosteroids, psoralen plus ultraviolet A (PUVA), or cyclosporine) or psoriasis (methotrexate, PUVA, retinoids, cyclosporine, adalimumab, efalizumab, etanercept, infliximab, or ustekinumab) consistent with severe disease. Patients who did not receive such therapy were classified as mild. Collection of data on diabetes, hypertension, smoking history, and alcohol abuse has been described in detail elsewhere (30–32). From Statistics Denmark we used information on tax-reported household income to calculate an age-standardized index of socioeconomic status based on the mean gross annual income during a 5-year period before study start. Patients with gallstones were identified by ICD-8 574 and ICD-10 K80.
This study described baseline characteristics with means and standard deviations (SDs) for continuous variables and frequencies and percentages for categorical variables. The baseline prevalence of gallstones was determined as the percentage of individuals who had received a diagnosis of gallstones between 1 January 1978 (when the DNPR was established) and 1 January 2008. A cross-sectional design was applied using logistic regression models to assess the odds ratios (ORs) of gallstones on 1 January 2008. In a cohort study design patients were followed from 1 January 2008 and until death, migration, 31 December 2012, or a diagnosis of gallstones, whichever came first. Incidence rates per 1,000 person-years were estimated, and Cox regression models were used to obtain hazard ratios (HRs) for the risk of incident gallstones. Incidence of gallstones during follow-up was calculated for all individuals without a history of gallstones prior to study start. ORs and HRs for gallstones were calculated as age- and sex-adjusted, and fully adjusted (in which age, sex, socioeconomic status, and healthcare consumption (number of clinic visits) were considered). Sensitivity analyses were performed with additional adjustments for diabetes, alcohol abuse, and cholesterol-lowering drug use, as well as additional adjustment for inflammatory bowel disease (IBD). Two-tailed p-values < 0.05 were considered statistically significant and results were reported with 95% confidence intervals (95% CIs), where applicable. All analyses were performed with SAS statistical software version 9.4 (SAS Institute Inc. Cary, NC, USA) and STATA software version 13.0 (StataCorp, College Station, TX, USA)
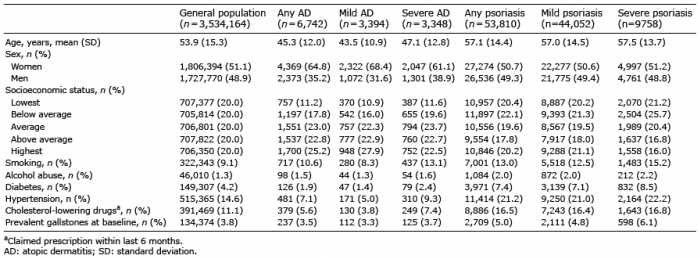
The study cohort comprised 3,534,164 subjects from the general population, 6,742 patients with adult AD, and 53,810 patients with psoriasis. A total of 3,394 patients had mild AD, and 3,348 had severe AD. Among patients with psoriasis, 44,052 had mild, and 9,758 had severe psoriasis, respectively. The mean ages at baseline ranged from 43.5 to 57.5 years across the groups, and there was an equal sex distribution, except among patients with adult AD, who were predominantly female (Table I). The prevalence of smoking and alcohol abuse was comparable between adult AD patients and the general population, but higher among patients with psoriasis. Notably, compared with the general population, diabetes, hypertension, and cholesterol-lowering drug use was significantly less frequent among adult AD patients, but occurred more often among patients with psoriasis.
Table I. Baseline characteristics of the study population
At baseline, the period prevalence (from 1978 until 2008) of gallstones was 3.8%, 3.5% and 5.0% for the general population, patients with AD, and patients with psoriasis, respectively. Stratified by disease severity, the prevalence was 3.3% and 3.7% in mild and severe AD, and 4.8% and 6.1% in mild and severe psoriasis (Fig. 1). Using a cross-sectional design, the OR of gallstones was significantly decreased among adult AD patients (adjusted OR 0.81; 0.71–0.92), but increased among psoriasis patients (adjusted OR 1.18; 1.14–1.23). Adjusted ORs for mild and severe AD were 0.78 (0.65–0.94) and 0.84 (0.70–1.01), respectively, and for psoriasis 1.15 (1.10–1.20) and 1.31 (1.20–1.42), respectively (Table II).
Fig. 1. Baseline prevalence of gallstones among the general population, patients with adult atopic dermatitis (AD), and patients with psoriasis, respectively. The baseline prevalence of gallstones was not significantly different (p = 0.218) between patients with adult AD and the general population, but significantly higher (p < 0.001) among patients with psoriasis (including mild and severe psoriasis) compared with the general population.
Table II. Odds ratios for association between adult atopic dermatitis and psoriasis, and gallstones at baseline (cross-sectional study design)
During follow-up in the cohort study, there were 44,353, 76 and 795 cases of incident (new-onset) gallstones among the general population, patients with AD, and patients with psoriasis, respectively, as shown in Table III. The adjusted HR of incident gallstones was 0.72 (0.56–0.90) for adult AD, and 1.10 (1.02–1.18) for psoriasis. Stratified by disease severity, the 5-year risk of incident gallstones was significantly decreased among patients with mild AD (adjusted HR 0.57; 0.40–0.81) and also showed a decreased risk, albeit not statistically significant, among patients with severe AD (adjusted HR 0.86; 0.64–1.16). For patients with mild psoriasis the risk of gallstones was not increased (adjusted HR 1.07; 0.98–1.16; p = 0.1145), but the risk was significantly increased among patients with severe psoriasis (adjusted HR 1.24; 1.07–1.44) (Table IV). In sensitivity analyses with additional adjustment for diabetes, alcohol abuse, and cholesterol-lowering drug use, as well as in analyses further adjusted for IBD, there were no significant changes in any of the reported ORs or HRs, compared with the primary analyses (data not shown).
Table III. Summary of number of new events, follow-up time, and incidence rates of incident gallstones/1000 person-years (PY)
Table IV. Hazard ratios (HR) for risk of incident gallstones
among patients with adult atopic dermatitis (AD) and psoriasis, compared with the general population (cohort study design)
This nationwide study of the adult Danish population found an increased prevalence and risk of gallstones in patients with psoriasis. However, the prevalence and risk were significantly lower among patients with AD compared with the general population. These findings support the notion that patients with psoriasis tend to be obese and overweight, while the same does not hold true for Danish adults with AD.
While 2 of 3 studies from the US have supported an association of AD with CVD (5, 6, 33), one Danish study could not confirm an association following adjustment for risk factors including tobacco smoking (8). One explanation could be that adult patients with AD in Denmark and the US have different risk profiles including overweight and obesity (9). Studies have shown that US paediatric and adult patients with AD have less physical activity than controls, whereas a study from Sweden showed no difference in 20–34-year-olds (34–36). While, to our knowledge, there are no published data on BMI in Danish adults with AD, we have previously performed a cohort study including 344 adults with AD and 2,999 general population controls in Denmark (37). In that cohort, the mean ± SD BMI was 25.9 ± 5.2 and 25.9 ± 4.6) kg/m2 in adults with AD and the general population, respectively (unpublished data).
Conversely, the link between psoriasis and obesity is well-established (11, 38) and obese patients with psoriasis are less likely to achieve a satisfactory treatment response compared with lean individuals (15).
While a disease-severity-dependent risk of co-morbidities in patients with psoriasis is often attributed to systemic low-grade inflammation (39), formation of gallstones is generally considered to be non-inflammatory in nature (19). Thus, it is likely that the observed discrepancy in risk of gallstones between AD and psoriasis is due to body weight rather than to differences in their inflammatory pathways. In further support of such a hypothesis, it is interesting to note the markedly higher prevalence of diabetes and cholesterol-lowering drug use (suggestive of hyperlipidaemia) among patients with psoriasis in our study, as opposed to the very modest prevalence in patients with AD compared with the general population.
Certain limitations apply to the interpretation of the present results. Due to the observational nature of our study, we cannot claim a causal link. While differences in BMI would be a logical explanation, we cannot refute that other factors may also have played a role. It is well-recognized that gallstones are more common among women and that the risk increases with age (19). Thus, although we adjusted for such differences in our model, residual confounding from other risk factors could have affected our results. Also, while we sampled patients with psoriasis from the general population and hospital settings, data on adult AD were available only from patients seen in hospital (including ambulatory) clinics. Indeed, it is plausible that such patients may comprise the more severe cases of AD. However, this would arguably have biased the results towards the null, i.e. no difference, suggesting that the true difference may be even higher. Lastly, the Danish population is predominantly of Caucasian decent and the results should be interpreted accordingly.
In conclusion, this study found a significantly decreased risk of gallstones in patients with adult AD, but the risk was increased in patients with psoriasis. The findings may suggest important differences in obesity and modifiable lifestyle factors among patients with AD and those with psoriasis.
Conflicts of interest: AE has received research funding and/or consultancy honoraria from Pfizer and Eli Lilly. YMFA is supported by an unrestricted grant from the Lundbeck Foundation. LS has received consultancy and/or speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, Merck Sharp & Dohme, and Leo Pharma and is a member of the advisory boards of Abbvie, Pfizer, Janssen-Cilag, Merck Sharp & Dohme, Eli Lilly, Celgene and Novartis. GHG is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. JPT is supported by an unrestricted grant from the Lundbeck Foundation and has received speaker honoraria from Galderma and MEDA.


 Click to show fullsize
Click to show fullsize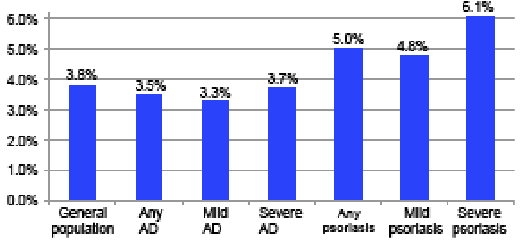 Click to show fullsize
Click to show fullsize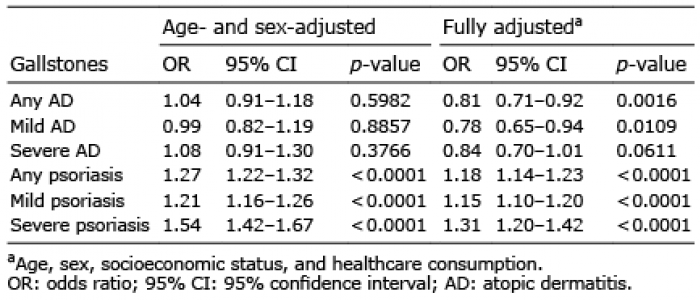 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize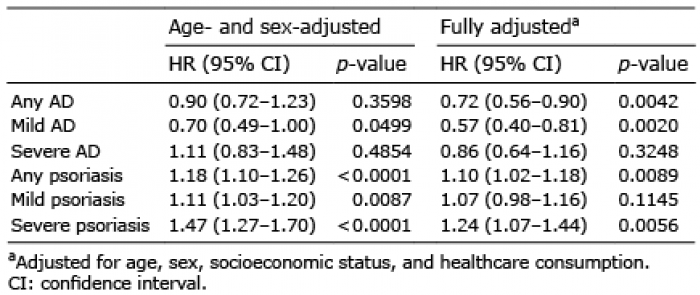 Click to show fullsize
Click to show fullsize