


Department of Dermatology, Faculty of Medicine, University of Tokyo, Tokyo, Japan
Angiogenesis is regarded as an essential step in supporting tumour growth and metastasis. In haematological malignancies, including cutaneous T-cell lymphoma (CTCL), angiogenesis is increased and serum levels of some pro-angiogenic markers are elevated. The aim of this study was to investigate expression levels of placental growth factor (PlGF) and vascular endothelial growth factor (VEGF)-A in lesional skin and sera in patients with CTCL, and to assess the association of these factors with development of CTCL. A further aim was to investigate the effect of PlGF on lymphoma cell growth in vivo using a tumour inoculation model. Expression of PlGF and VEGF-A were significantly elevated in CTCL skin. Tumour cells expressed PlGF in some cases. Serum PlGF levels were increased in patients with advanced CTCL and correlated with disease markers. Moreover, PlGF enhanced lymphoma cell growth in vivo through increasing tumour vasculature. These findings suggest that angiogenesis plays a role in the progression of CTCL and raises the possibility of using inhibitors of PlGF in CTCL therapy.
Key words: placental growth factor; cutaneous T-cell lymphoma; angiogenesis; disease marker.
Accepted Jan 24, 2017; Epub ahead of print xx
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Tomomitsu Miyagaki, Department of Dermatology, Faculty of Medicine, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan. E-mail: asahikari1979@gmail.com
Mycosis fungoides (MF) and Sézary syndrome (SS) are the most common types of cutaneous T-cell lymphoma (CTCL). MF is characterized by the malignant proliferation of neoplastic CD4+ CD45RO+ T cells, which preferentially traffic to the skin, and has a classically prolonged clinical course. A small proportion of cases progress over years through patch, plaque, and tumour stages, followed by lymph node and visceral involvement (1). SS is characterized by fever, erythroderma, lymphadenopathy, and leukaemic involvement, and usually has a rapid clinical course (2). Although the pathogenesis of CTCL is unknown, a variety of cytokines/chemokines are reported to be involved in development of the disease (3–5).
Angiogenesis, the growth of new blood vessels from pre-existing ones, is regarded as an important step to support primary and metastatic tumour growth (6). Angiogenesis is also thought to be important for the progression of haematological malignancies. Some clinical observations have indicated that tumour microvessel density, measured by CD34, CD31, or von Willebrand factor expression, is increased in various lymphoproliferative disorders (7). Increased serum levels of pro-angiogenic markers are also reported in some haematological malignancies (7). Similarly, in CTCL, angiogenesis, assessed either by microvessel density or by microvessel number in lesional skin, is increased, suggesting that interaction between tumour cells and their microvasculature is likely to occur during the progression of CTCL (8, 9). Consistent with those reports, increased expression of angiogenin, one of the angiogenic factors, in the sera and lesional skin was reported in patients with erythrodermic CTCL (10). Serum levels of angiopoietin-2 (Ang-2), which has the capacity to promote both angiogenesis and lymphangio-genesis, are also elevated in patients with SS and are correlated with disease severity markers (11).
Among pro-angiogenic and pro-lymphangiogenic factors, vascular endothelial growth factor (VEGF) family is generally regarded as the key player in both physiological and pathological skin angiogenesis and lymphangiogenesis. VEGF family comprises VEGF-A, VEGF-B, VEGF-C, VEGF-D, and placental growth factor (PlGF). VEGF-A activates VEGF receptor (VEGFR)-1 and VEGFR-2 on vascular endothelial cells and promotes angiogenesis. VEGF-B and PlGF bind to VEGFR-1 and manifest angiogenic properties. VEGF-C and VEGF-D mainly modulate lymphangiogenesis through VEGFR-3, but may also induce angiogenesis through VEGFR-2. VEGF-A is secreted by tumour cells of MF and cell lines of MF/SS, while its receptors, VEGFR-1 and VEGFR-2, are not expressed on tumour cells (12–14). Thus, VEGF-A may contribute to MF/SS progression through angiogenesis. However, PlGF involvement in MF/SS has not been studied, whereas PlGF is known to have strong angiogenic properties in the skin, partially via enhancing VEGF-A action (15, 16).
The aim of this study was to measure the expression of both PlGF and VEGF-A in lesional skin and PlGF expression in sera of patients with MF/SS. A further aim was to assess the effects of PlGF on lymphoma cell growth in vivo to clarify the involvement of PlGF in the development of MF/SS.
Messenger RNA (mRNA) was obtained from frozen biopsy materials of lesional skin of MF/SS (n = 26, patch 9, plaque 8, tumour 5, erythroderma 4; distribution of patients by stage: IA 7, IB 10, IIA 0, IIB 5, IIIA 1, IIIB 0, IVA1 3, IVA2 0, IVB 0) and normal skin adjacent to benign skin tumours (n = 5) using RNeasy Fibrous Tissue Mini Kit (QIAGEN, Valencia, CA, USA). Skin samples for immunohistochemistry were collected from patients with MF/SS (n = 28, patch 6, plaque 9, tumour 5, erythroderma 8; distribution of patients by stage: IA 6, IB 11, IIA 0, IIB 5, IIIA 1, IIIB 0, IVA1 3, IVA2 0, IVB 0) and patients with atopic dermatitis (AD) (n = 5). Serum samples were obtained from 42 patients with MF/SS (36 MF cases and 6 SS cases; mean ± standard deviation (SD) age: 59.4 ± 14.1 years; 27 males and 15 females; distribution of patients by stage: IA 10, IB 14, IIA 0, IIB 10, IIIA 2, IIIB 0, IVA1 6, IVA2 0, IVB 0) and 14 healthy control subjects (58.0±12.5 years, 7 males and 7 females). The healthy controls had no history of allergy, psoriasis, or CTCL. All samples were collected during daily clinical practice. The medical ethics committee of the University of Tokyo approved all described studies and the study was conducted according to the principles of the Declaration of Helsinki. Informed consent was obtained to use blood and skin samples from patients and healthy controls. All patients with MF/SS were given diagnoses according to WHO classification for cutaneous lymphomas.
Human MF cell line, MyLa, and human SS cell line, SeAx, were kindly provided by Dr Kazuyasu Fujii (Department of Dermatology, Okayama University, Japan). Human SS cell line, Hut-78, and mouse T-cell lymphoma cell line, EL-4, were kindly provided by Dr Sam T. Hwang (Medical College of Wisconsin, Milwaukee, WI, USA). A total of 4 × 105 MyLa, SeAx, and Hut-78 cells were cultured in 1 ml serum-free RPMI1640 (Millipore, Billerica, MA, USA) for 36 h and supernatants were harvested to investigate PlGF expression from those cell lines. EL-4 cells were grown in Eagle’s minimum essential medium (MEM; Sigma, St Louis, MO, USA) with 10% foetal bovine serum (FBS) and supplements.
C57BL/6 mice were purchased from SLC Japan (Hamamatsu, Japan). All experiments were performed using female mice between 8 and 14 weeks of age. All studies were approved by the animal ethics review board of the University of Tokyo and the Animal Committee of National Center for Global Health and Medicine.
cDNA was synthesized using TaqMan® Reverse Transcription Reagents (Applied Biosystems, Foster City, CA, USA). Quantitative RT-PCR was performed. Primers for human PlGF, VEGF-A, interleukin (IL)-4, and GAPDH were as follows: PlGF forward, 5’-GCG ATG AGA ATC TGC ACT CTG T-3’ and reverse, 5’-TCC CCA GAA CGG ATC TTT AGG-3’; VEGF-A forward, 5’-AGC CTT GCC TTG CTG CTC TAC-3’ and reverse, 5’-TCC TCC TTC TGC CAT GGG T-3’; IL-4 forward, 5’-CAC AGG CAC AAG CAG CTG AT-3’ and reverse, 5’-CTC TGG TTG GCT TCC TTC ACA-3’; GAPDH forward, 5’-ACC CAC TCC TCC ACC TTT GA-3’ and reverse, 5’-CAT ACC AGG AAA TGA GCT TGA CAA-3’. Primers for human CC chemokine ligand (CCL)27 were purchased from Applied Biosystems.
Immunohistochemical staining was performed for PlGF and VEGF-A within lesional skin of MF/SS and AD. Normal skin adjacent to benign skin tumours served as controls (n = 6). Immunohistochemical staining was also performed for CD34 within mouse tumour tissues to identify vessels in and around the tumour. Briefly, 5-mm thick tissue sections from formaldehyde-fixed and paraffin-embedded samples were dewaxed and rehydrated. These sections were then stained with goat anti-human PlGF polyclonal antibody (Santa Cruz, Dallas, TX, USA), goat anti-human VEGF-A polyclonal antibody (R & D Systems, Minneapolis, MN, USA), or anti-CD34 monoclonal antibody (Nichirei Biosciences, Tokyo, Japan) followed by ABC staining (Vector Lab, Burlingame, CA, USA). Diaminobenzidine was used to visualize the staining, and counterstaining with Mayer haematoxylin was performed, according to the manufacturers’ instructions. The following grading system was used for keratinocytes and endothelial cells: – negative; +/– slight staining; + moderate staining; ++ strong staining. For tumour cells, the following grading system was used: – negative; +/– >0–25% of tumour cells stained; + >25–50% tumour cells stained; ++ >50% tumour cells stained.
Immunoreactive PlGF in sera and supernatant were quantified by human enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems). These assays employ the quantitative sandwich enzyme immunoassay technique. Optical densities were measured at 450 nm using a Bio-Rad Model 550 microplate reader (Bio-Rad Laboratories, Hercules, CA, USA). The concentrations were calculated from the standard curve generated by a curve-fitting program. Values from individual patients were plotted as dots.
EL-4 cells (5×106) in 100 ml of phosphate buffered saline (PBS) with 2.0 mg/ml PlGF (PlGF group) or without PlGF (PBS group) were injected subcutaneously into the shaved left flank of C57BL/6 mice. On days 4, 7 and 11, 2.0 mg/ml PlGF in 100 ml of PBS was injected into the lesion in the PlGF group, whereas PBS was injected in the PBS group. On days 4, 7, 11 and 14, 2 perpendicular diameters were measured and tumour size determined. On day 14, the tumour tissues were harvested for immunohistochemical investigation.
Statistical analysis between 2 groups was performed using the Mann–Whitney U test. For testing equality of population means among 3 or more groups, Kruskal–Wallis test was used. Correlation coefficients were determined by using the Spearman’s rank correlation test. Wilcoxon signed-rank test was used to investigate the difference between before and after treatment. p-values < 0.05 were considered statistically significant.
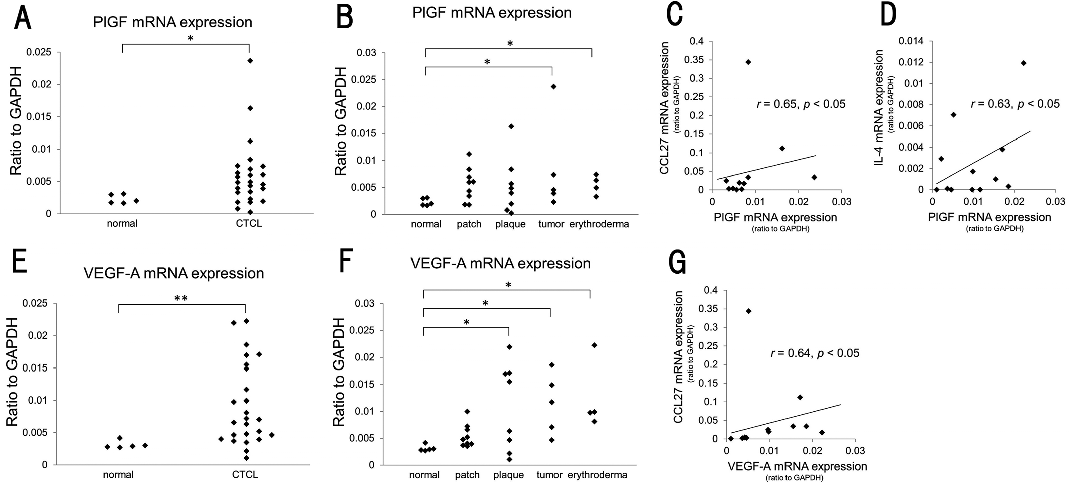
To investigate PlGF involvement in MF/SS, we first examined mRNA expression in lesional skin of MF/SS and normal skin. Expression levels of PlGF were significantly increased in MF/SS skin (p < 0.05; Fig. 1A). When classified according to the types of skin lesions, patients with tumour or erythroderma showed increased PlGF mRNA expression in lesional skin (p < 0.05, and p < 0.05, respectively; Fig. 1B). When classified according to staging, PlGF mRNA expression was significantly elevated in lesional skin of patients with stage IIB and IVA1 (p < 0.05, and p < 0.05, respectively; Fig. S1A). Next, we evaluated correlations of expression levels of PlGF with disease severity markers in MF/SS lesional skin. PlGF mRNA expression levels were significantly correlated with those of CCL27 (Fig. 1C). CCL27 expression in lesional skin was previously reported to be a potential marker of disease activity, as it is correlated with tumour cell density and correlated inversely with dendritic cell and CD8+ lymphocyte density (17). Moreover, PlGF expression levels significantly correlated with IL-4 expression levels (Fig. 1D), which are also associated with disease activity (18). We next examined VEGF-A mRNA expression in lesional skin of MF/SS and normal skin, because PlGF is known to promote angiogenesis partially via enhancing VEGF-A (15, 16). Expression levels of VEGF-A were significantly elevated in MF/SS skin (p < 0.01; Fig. 1E). When classified according to the types of skin lesions, patients with plaque, tumour or erythroderma showed increased VEGF-A mRNA expression in lesional skin (p < 0.05, p < 0.05, and p < 0.05, respectively; Fig. 1F). When classified according to staging, VEGF-A mRNA expression was significantly elevated in lesional skin of patients with stage IB, IIB and IVA1 (p < 0.05, p < 0.05, and p < 0.05, respectively; Fig. S1B). Similar to PlGF mRNA expression, VEGF-A mRNA expression was also correlated with CCL27 mRNA expression (Fig. 1G), whereas VEGF-A mRNA expression was not correlated with PlGF mRNA expression. Thus, both PlGF and VEGF-A mRNA expression levels are increased in MF/SS skin and correlated with disease activity.
Fig. 1. Quantitative real-time PCR (RT-PCR) results. (A) Placental growth factor (PlGF) mRNA expression in lesional skin of cutaneous T-cell lymphoma (CTCL) and normal skin. (B) PlGF mRNA expression in lesional skin of CTCL classified with types of skin lesions and normal skin. Values from individual patients were plotted as dots. *p < 0.05. (C) Correlations between PlGF mRNA expression and CC chemokine ligand 27 (CCL27) mRNA expression in lesional skin of CTCL. (D) Correlations between PlGF mRNA expression and IL-4 mRNA expression in lesional skin of CTCL. (E) Vascular endothelial growth factor (VEGF)-A mRNA expression in lesional skin of CTCL and normal skin. (F) VEGF-A mRNA expression in lesional skin of CTCL classified with types of skin lesions and normal skin. Values from individual patients were plotted as dots. **p < 0.01, *p < 0.05. (G) Correlations between VEGF-A mRNA expression and CCL27 mRNA expression in lesional skin of CTCL.
To examine PlGF and VEGF-A protein expression in lesional skin, we immunolabelled MF/SS lesional skin and normal skin for PlGF and VEGF-A. We also immunolabelled lesional skin of AD, as AD is a representative inflammatory skin disease, which is regarded as a Th2-type disease similar to MF/SS. In normal skin, epidermal keratinocytes and vascular endothelial cells expressed PlGF (Fig. 2A). In lesional skin of AD, PlGF expression on epidermal keratinocytes and vascular endothelial cells was slightly up-regulated (Fig. 2B). On the other hand, in lesional skin of MF/SS, expression levels of PlGF were obviously higher than those in normal skin (Fig. 2C). In addition, in contrast to AD skin, which barely contains PlGF-expressing dermal infiltrating cells, lesional skin in some MF/SS cases contained PlGF-expressing epidermotropic lymphocytes and dermal lymphocytes with atypical nuclei, which were considered to be tumour cells (Fig. 2D, E). To confirm PlGF expression on tumour cells, we measured expression of PlGF by MF/SS cell lines by ELISA. Among 3 MF/SS cell limes, SeAx, MyLa, and Hut-78 cells, only SeAx cells expressed PlGF (Fig. S2). This result was compatible with the immunohistochemistry results, showing that tumour cells in some cases expressed PlGF. In addition, normal skin barely contained VEGF-A-expressing cells (Fig. 2F). In lesional skin of AD, VEGF-A was expressed on epidermal keratinocytes and vascular endothelial cells (Fig. 2G). In lesional skin of MF/SS, epidermal keratinocytes were scarcely positive for VEGF-A, whereas vascular endothelial cells expressed VEGF-A to the same extent as those in AD skin (Fig. 2H). In contrast to AD skin, which barely contains VEGF-A-expressing dermal infiltrating cells, lesional skin of most MF/SS cases contained many VEGF-A-expressing cells in the dermis (Fig. 2H). In some cases of MF/SS, there were abundant VEGF-A-expressing cells, which had atypical nuclei, in the dermis (Fig. 2I). Thus, tumour cells of MF/SS expressed VEGF-A, consistent with previous reports (12, 13). We summarized the results of immunohistochemistry of 28 patients with MF/SS (patch 6, plaque 9, tumour 5, and erythroderma 8) in Table SI. Thus, epidermal keratinocytes expressed PlGF, while vascular endothelial cells expressed both PlGF and VEGF-A in MF/SS skin. Furthermore, tumour cells expressed PlGF in some cases and VEGF-A in most cases.
Fig. 2. Immunohistochemistry results. Immunohistochemistry of placental growth factor (PlGF) in: (A) normal skin and (B) lesional skin of patients with atopic dermatitis, and (C) cutaneous T-cell lymphoma (CTCL). (D) Immunohistochemistry of PlGF in CTCL lesional skin in which tumour cells were partially positive for PlGF. (E) A higher magnification of (D). The arrows indicate representative PlGF positive tumour cells. The arrowheads indicate representative PlGF positive endothelial cells. Immunohistochemistry of vascular endothelial growth factor (VEGF)-A in (F) normal skin and lesional skin of patients with (G) atopic dermatitis and (H) CTCL. (I) Immunohistochemistry of VEGF-A in CTCL lesional skin in which most tumour cells were positive for VEGF-A.
We next measured serum PlGF levels in MF/SS patients and healthy controls. Serum PlGF levels of patients with MF/SS (20.9 ± 6.0 pg/ml) were similar to those of healthy controls (17.8 ± 1.9 pg/ml; data not shown). When classified according to types of skin lesions, patients with tumour or erythroderma showed higher levels of serum PlGF (22.5 ± 5.4 and 23.3 ± 6.1 pg/ml, respectively) than normal controls (p < 0.05 and p < 0.05, respectively; Fig. 3A). When classified according to staging, patients with stage IIB showed significantly higher PlGF levels in sera than normal controls (p < 0.05; Fig. S3). We also measured serum PlGF levels in 6 MF/SS cases before and after treatment, which included topical and oral corticosteroids, ultraviolet (UV) phototherapy, oral etretinate, oral vorinostat, and/or systemic chemotherapy. Serum PlGF levels after treatment were significantly lower than those before treatment (p < 0.05; Fig. 3B). We next compared serum PlGF levels in MF/SS patients with other clinical markers for disease severity. Serum PlGF levels correlated significantly with serum CCL17, Ang-2, and IL-10 levels (r = 0.39, p < 0.05, r = 0.40, p < 0.05, and r = 0.74, p < 0.05; Fig. 3C–E), all of which were associated with disease severity and progression (11, 18–20). Thus, in patients with advanced MF/SS, serum PlGF levels are elevated and associated with disease severity and activity.
Fig. 3. Placental growth factor (PlGF) expression in sera. (A) Serum levels of PlGF in patients with cutaneous T-cell lymphoma (CTCL) classified with types of skin lesions and normal skin. (B) Serum levels of PlGF in patients with CTCL before and after treatment. Values from individual patients were plotted as dots. *p < 0.05. (C–E) Correlations between serum PlGF levels and serum CC chemokine ligand 17 (CCL17) (C), angiopoietin-2 (D), and interleukin (IL)-10 (E) levels.
On the basis of the data above indicating strong association between PlGF and disease severity of MF/SS, we assessed the effects of PlGF on lymphoma cell growth in vivo. EL-4 cells, a mouse T-cell lymphoma cell line, were injected subcutaneously into the left flank of C57BL/6 mice, followed by repeated treatment with PlGF. Significantly larger tumours developed in the mice treated with PlGF compared with those treated with PBS (Fig. 4A). As PlGF did not affect EL-4 cell growth in vitro (data not shown), we decided to investigate angiogenesis in the tumours using CD34 staining. The number of CD34-positive vessels was higher in the tumours treated with PlGF than in those treated with PBS (Fig. 4B, C). Thus, PlGF administration increased vasculature and enhanced tumour growth of EL-4 cells in vivo.
Fig. 4. Placental growth factor (PlGF) enhances tumour growth of EL-4 cells in vivo. (A) EL-4 cells were injected into the shaved abdomen of C57/BL6 mice with phosphate-buffered saline (PBS) or recombinant PlGF (2.0 μg/ml). Each reagent was injected on days 4, 7, and 11. Tumour size was calculated as (long×short axis) on days 4, 7, 11 and 14. Values are means and standard error of the mean (SEM) (n = 8). *p < 0.05, **p < 0.01. (B) Numbers of CD34 positive vessels in mouse tutors on day 14 per high-power field. Values are means and SD (n = 8). *p < 0.05. (C) Immunohistochemistry of CD34 in mouse tumours on day 14. Arrows indicate CD34-positive vessels.
Angiogenesis is defined as the production of new blood vessels from an existing vascular network and is involved in the development and progression of pathogenic processes in a variety of disorders, including psoriasis, rheumatoid arthritis, diabetic retinopathy, cardiovascular diseases, and solid and haematological malignancies. Indeed, VEGF-A inhibitor, bevacizumab, is used for the treatment of several solid and haematological malignancies. Increased angiogenesis has also been reported in lesional skin of MF. Microvessel density, assessed by von Willebrand factor expression, is increased in lesional skin of plaque or tumour MF (8). In addition, the number of microvessels measured by CD34 staining is increased in lesional skin of advanced MF, stage III or IV (9). Although precise mechanisms of angiogenesis in CTCL remain unclear, it is known that T cells, mast cells, and macrophages are capable of producing angiogenic factors (21). Therefore, increased capillary formation may be induced by lymphoma cells themselves and/or by tumour-associated host cells (9). Dermal infiltrating T cells consistently express angiogenin, which is a member of the ribonuclease superfamily and is associated with the angiogenic process (22), in lesional skin of erythrodermic MF and SS (10). A previous study has shown that tumour cells of MF/SS express Ang-2 (11), which, alongside VEGF-A, facilitates angiogenesis.
Concerning VEGF family expression in MF/SS, 2 different groups have reported that tumour cells, as well as dermal endothelial cells, express VEGF-A in lesional skin of MF/SS (12, 13). Similar to those 2 previous reports, we found that mRNA and protein expression levels of VEGF-A were elevated in lesional skin of MF/SS and that dermal endothelial cells and tumour cells mainly expressed VEGF-A (Fig. 1E, F, Fig. 2H, I). PlGF belongs to VEGF family and represents a key regulator of angiogenic events in development and pathological conditions (23). PlGF mRNA and protein expression were up-regulated in lesional skin of MF/SS (Fig. 1A, B, Fig. 2C–E). In addition, PlGF mRNA expression was correlated with CCL27 mRNA expression in lesional skin, a potential marker of disease activity (17), suggesting PlGF involvement in angiogenesis and progression in MF/SS lesional skin. Indeed, local administration of PlGF enhanced lymphoma cell growth in vivo through increasing tumour vasculature (Fig. 4), indicating PlGF capacity to contribute to MF/SS development. We also found that VEGF-A mRNA expression in lesional skin was correlated with CCL27 mRNA expression in the same way as PlGF mRNA expression. This result is consistent with the previous reports describing that PlGF and VEGF-A promote angiogenesis in a concerted manner (15, 16). By immunohistochemistry, we detected that epidermal keratinocytes and dermal endothelial cells expressed PlGF, consistent with previous reports (24, 25). More interestingly, we first found that tumour cells in some MF/SS cases expressed PlGF (Fig. 2D, Table SI). According to the previous results, PlGF is expressed in only a limited number of tumour-derived cell lines, which is different from VEGF-A (26, 27). Similarly, in contrast to previous reports describing that tumour cells of MF/SS expressed VEGF-A in almost all cases (12, 13), the number of MF/SS cases with PlGF-expressing tumour cells was limited in our study. Moreover, among 3 MF/SS cell lines, only SeAx cells expressed PlGF (Fig. S1). As angiogenin and Ang-2 are also expressed by tumour cells of MF/SS (10, 11), MF/SS tumour cells may have the strong ability to increase local vasculature by producing various pro-angiogenic factors. Furthermore, we found that PlGF mRNA expression was correlated with IL-4 mRNA expression in lesional skin of MF/SS (Fig. 1D). It is known that PlGF has the capacity to down-regulate Th1 immune response by modulating the function of dendritic cells other than angiogenesis (28). Considering that a Th2-dominant microenvironment assists MF/SS progression (5), PlGF might also be involved in MF/SS development through Th2-polarization.
Although PlGF expression levels in bone marrow are associated with prognosis of some haematological malignancies (29, 30), serum PlGF levels have not been investigated in haematological malignancies. In this report, we found that serum PlGF levels were increased in MF/SS patients with tumour or erythroderma (Fig. 3A). Serum PlGF levels decreased after treatment (Fig. 3B) and correlated with serum CCL17, Ang-2, and IL-10 levels (Fig. 4C–E), all of which are disease markers of MF/SS (11, 19, 20). Our results suggest that serum PlGF levels may be a disease marker not only for MF/SS, but also for other haematological malignancies.
In conclusion, this study reveals that expression of both PlGF and VEGF-A are increased in MF/SS lesional skin and that PlGF expression is elevated in the sera of patients with advanced MF/SS. MF/SS tumour cells have the capacity to produce PlGF and VEGF-A, suggesting involvement of those pro-angiogenic factors in angiogenesis during progression of MF/SS. In addition, considering the correlations of expression of PlGF with disease severity, inhibitors of PlGF or VEGFR inhibitors could be promising therapies in MF/SS.
The authors thank Tamami Kaga for technical assistance. This work was supported by grants from the Ministry of Education, Culture, Sports and Technology (Japan; 26893052 and 16K19709).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize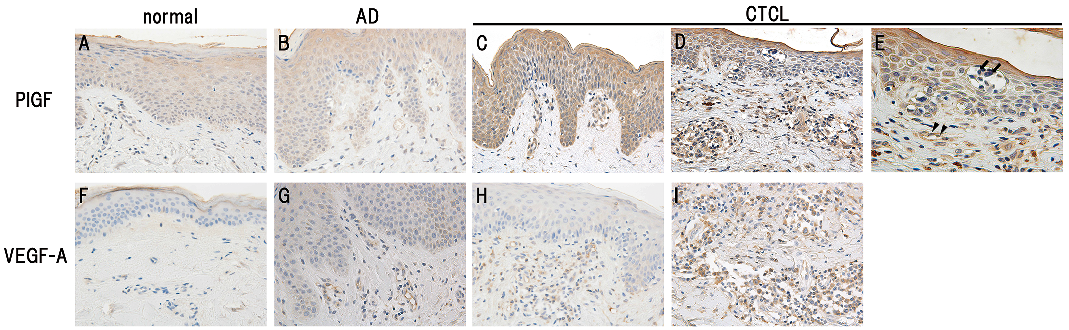 Click to show fullsize
Click to show fullsize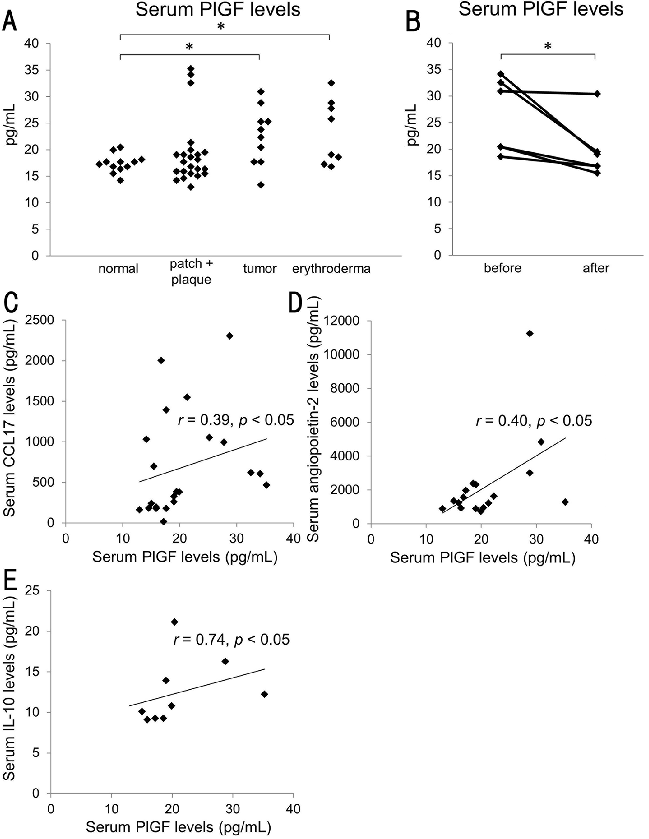 Click to show fullsize
Click to show fullsize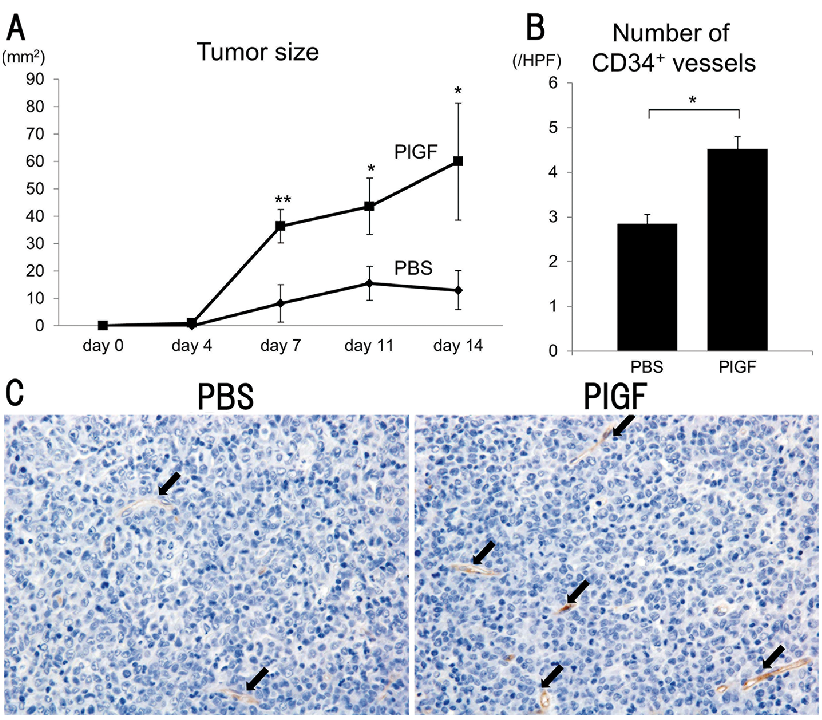 Click to show fullsize
Click to show fullsize