


Department of Dermatology, University Hospital Jena, Erfurter Str. 35, DE-07743 Jena, Germany. E-mail: judit.lukacs@med.uni-jena.de
Accepted Jan 25, 2017; Epub ahead of print Jan 27, 2017
Necrobiotic xanthogranuloma (NXG) most often occurs in patients with paraproteinemia secondary to a haematologic disease, including chronic lymphocytic leukemia, monoclonal gammopathy of unknown significance and multiple myeloma (1, 2).
The most common manifestations are painless, non-pruritic papules at the beginning, with later progression to indurated yellow-red nodules, or plaques with a predilection for the periorbital tissues (1). NXG mostly affects patients in their fifth to sixth decade of life (3).
The pathogenesis of NXG remains unclear. An autoimmune response to paraproteinemia and/or the deposition of monoclonal protein in tissues is suggested (2).
A 74-year-old woman patient was presented to our department for multiple hemorrhagic skin lesions with secondary ulceration on the lower extremities. Laboratory tests revealed positive antinuclear antibody (1:500; normal range < 100), positive antiphospholipid antibodies with a prolonged activated partial thromboplastin time (37.6 s, normal 22–34 s), and elevated plasma cryofibrinogen. A biopsy of the lesion showed vasculopathy without leukocytolysis. Direct immunofluorescence was negative for IgA, IgM, and IgG. Improvement in skin lesions occurred with topical clobetasol propionate.
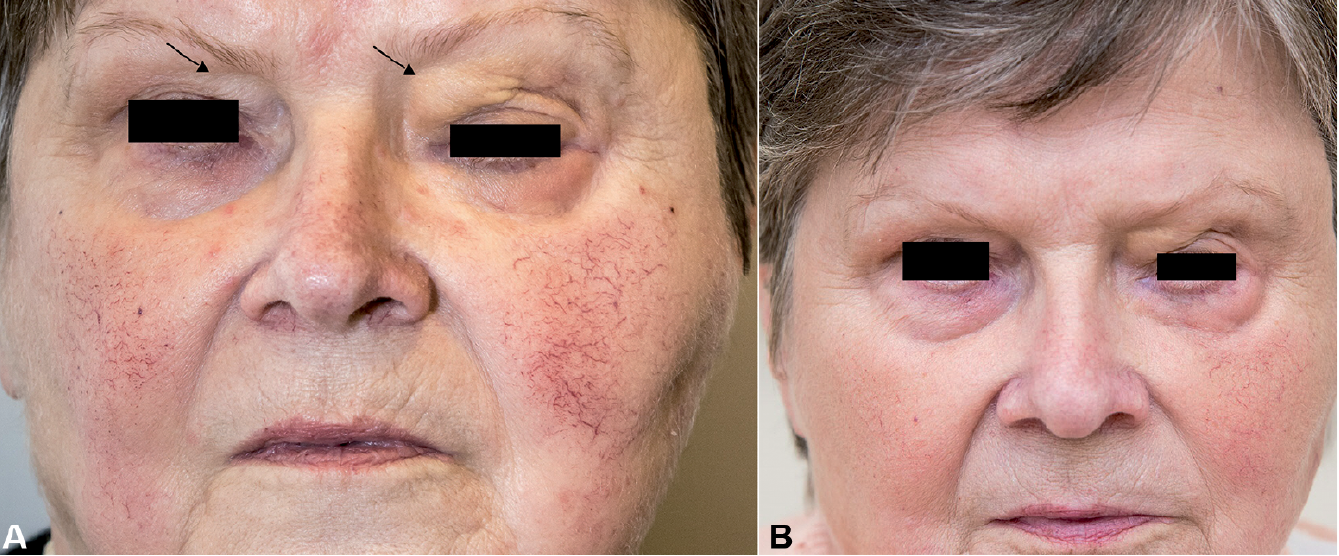
Three years later, physical examination revealed periorbital oedematous yellow plaques on both upper lids causing gravitational ptosis (Fig. 1A). Additionally, facial rosacea was diagnosed. There was no history of any other eye complaints or any significant haematologic disease. Medical history included hypertension, Factor XII deficiency and ischaemic heart disease.
Fig. 1. The clinical picture of necrobiotic xanthogranuloma (A) by the second presentation in the clinics: yellowish papules in the periorbital area (arrows) and (B) after 4 IVIG-cycles with beneficial response. A written permission from the patient is given to publish these photos.
The diagnosis of NXG was made on the basis of clinical and histopathological results. Histopathological examination showed several histiocytic giant cells resembling Touton giant cells with lymphocytes and few plasma cells.
Serum protein electrophoresis showed IgM kappa monoclonal gammopathy with an IgM level of 6.39 g/l (normal range 0.46–3.04 g/l) and an elevated alpha-2-globulin (12.7 g/l). The white blood cell count differential was within the standard range (neutrophil count 4.14 109/l (normal 1.8–7.7); lymphocyte count 2.51 109/l (normal 1.0–4.8); eosinophil count 0 109/l (normal < 0.5); basophil count 0.04 109/l (normal < 0.2); monocyte count 0.62 109/l (normal < 0.8)).
Quantitation of serum immune globulins demonstrated a normal IgA of 1.61 g/l and an elevated IgG (48.90 g/l; normal 7.51–15.60). Partial thromboplastin time was prolonged (37.6 s; normal range 22–34 s). Serum tests for cryofibrinogens were positive again. Other conditions like multiple myeloma were ruled out.
The patient was started on intravenous immunoglobulin (IVIG) infusions 0.5g/kg/day over 4 consecutive days every 4 weeks through 4 cycles. The therapy was well tolerated without any associated adverse events. Lesion improvement was noted after the second cycle. The treatment resulted in flattening of the periorbital lesions (Fig. 1B). The rosacea was treated with minocycline (50 mg twice daily) and topical metronidazole.
Due to the rarity of the condition, randomized controlled trials have not been performed, and there is limited evidence on treatment options. Therefore, case reports on successful treatment regiment remain to be important information (4).
While 80% of patients may not need any treatment or may only require topical agents or local procedures (3), various treatments including surgical excision, radiotherapy, plasmapheresis, systemic and intralesional corticosteroids have been reported in the literature (4, 5). Paraproteinemia has been successfully managed with plasmapheresis, leading to its rational use in treatment of NXG (4). Although plasmapheresis may be a good alternative therapy, a large number of adverse reactions were reported (e.g. myasthenia gravis, Guillain-Barre-Syndrome, Lyell’s syndrome, or thrombotic thromcytopenic purpura) (6, 7). Surgical excision carries a possible relapse rate (1). IVIGs (8) may induce long-lasting, at least partial remission, as observed in our patient, with negligible side effect. IVIG is an expensive therapy. High-dose IVIG treatment should be considered when other treatment modalities have failed (4, 9, 10).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize