


1Department of Dermatology, University of Montpellier and INSERM U1058, and 2Laboratory of Immunology, University of Montpellier, Montpellier, France
The aim of this 10-year monocentric prospective study was to determine a cut-off value of Fas/CD95 expression by peripheral blood CD4+ T lymphocytes in discriminating patients with mycosis fungoides from controls with cutaneous benign lymphocytic conditions. CD95 expression in peripheral blood CD4+ T lymphocytes was measured using flow cytometry in 330 patients referred for diagnosis: 104 with mycosis fungoides and 226 with eczema, psoriasis, drug reaction, etc. The sensitivity and specificity of different thresholds of CD95 expression were calculated regarding the final diagnosis of patients with mycosis fungoides or controls. CD95 expression higher than 30% reached a specificity of 91% in ruling out a diagnosis of mycosis fungoides, although overall CD95 expression was not significantly different from that of controls (p = 0.309) and sensitivity was very low (5%). Thus, peripheral CD95 expression higher than 30% could be used among the exclusion criteria in a multicomponent score for mycosis fungoides diagnosis.
Key words: mycosis fungoides; Fas/Fas ligand system; peri-pheral blood CD4+CD95+ rate; CD95 expression.
Accepted Feb 15, 2017; Epub ahead of print Feb 16, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Aurélie Du-Thanh, Department of Dermatology, University of Montpellier and INSERM U1058, Hôpital Saint-Eloi, 80 avenue Augustin Fliche, FR-34295 Montpellier cedex 5, France. E-mail: a-du_thanh@chu-montpellier.fr
The pathogenesis of mycosis fungoides (MF), the major subset of cutaneous T-cell lymphomas (CTCL), is largely unknown. Functional abnormalities of post-activation T-cell apoptosis have been suggested as initial pathomechanisms of MF. Specifically, an acquired impairment of the Fas/Fas ligand system could lead to a slow, but continuous, accumulation of non-proliferative, skin-addressed T cells (1). Fas, also called CD95, is a transmembrane protein belonging to the tumour necrosis factor superfamily, and is physiologically expressed on the surface of activated B- and T cells. Binding of Fas to Fas ligand activates the death-inducing signalling complex, which ultimately results in cell apoptosis through complex pathways mainly involving the activation of downstream caspases (2). In MF, inactivating mutations of the fas gene coding sequence, resulting in the production of an inefficient molecule or epigenetic changes with hypermethylation of the promoter region of this gene, leading to transcriptional down-regulation, have been reported (3–5).
Early diagnosis of MF, however, remains significantly challenging, due to the frequent lack of specific clinical and histological criteria at this stage resulting in delay in diagnosis and relevant care in many patients (6). The identification of T-cell clonal expansion in skin lesions, using molecular biology techniques, enabled a major improvement in early diagnosis; however, this approach does not always lead to a clear-cut conclusion. In an effort to circumvent this difficulty, the International Society for Cutaneous Lymphomas (ISCL) proposed a semi-quantitative score to help the early diagnosis of MF, based on clinical, histopathological, immunophenotyping and molecular criteria (7), although uncertain situations remain frequent. Thus, the search for additional, easy to implement diagnostic criteria that can also be used in difficult, ill-defined cutaneous T-cell infiltrates remains a relevant issue.
Previous studies, although limited in size, showed a significant reduction in the percentage of circulating CD4+ T-cell lymphocytes also expressing CD95 (CD4+CD95+/CD4+ ratio) in some patients with CTCL compared with cutaneous benign lymphocytic conditions (BLC) although the underlying mechanisms remain questionable; an attractive hypothesis would be the presence of a specific additional CD4+ CD95-population closely related to circulating clonal, neoplastic lymphocytes displaying fas gene abnormalities (either through mutations or epigenetic changes) resulting in a lack of expression of CD95 on the cell surface. This interpretation is consistent with the demonstration of the presence of the tumoural T-cell clone in peripheral blood in a significant number of early stages of MF. Moreover, immunochemistry studies showed that neoplastic T cells in CTCL skin lesions may also under-express CD95 (3, 8, 9).
Based on these previous, although limited, data, a prospective, large-scale study was designed to extend these preliminary results. The aims of this study were to investigate the possibly discriminating value of CD95 expression level by CD4+ circulating T lymphocytes between MF and BLC, and to assess the sensitivity and specificity of putative cut-off values of this CD4+CD95+/CD4+ ratio in the differential diagnosis of MF vs. BLC.
The study was designed as a prospective monocentre investigation. All adult patients diagnosed with either a definite MF identified through usual clinical, histopathological and immunological criteria or a BLC (mainly psoriasis, eczema, or cutaneous drug side-effect) between 2003 and 2013 in a unique third-line referral institution were consecutively enrolled in the study. In all patients, the percentage of peripheral blood CD4+ lymphocytes expressing CD95 (CD4+CD95+/CD4+ ratio) was evaluated by flow cytometry at initial diagnosis, before any specific treatment was introduced apart from topical treatment (mainly topical steroids) for a maximal time of 2 weeks regardless of the potency of the products. As peripheral lymphocytes immunophenotyping is currently used routinely in initial evaluation of cutaneous lymphocytic infiltrates, no specific informed consent was required from the patients.
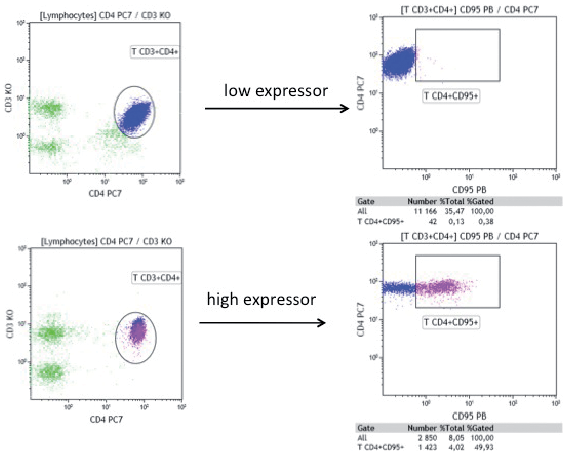
Immunophenotyping of peripheral blood lymphocytes was performed by routine flow cytometry using the following antibodies: CD3 Krome Orange (CD3 KO), CD4 Phycoerythrin-Cyanin 7 (CD4 PC7) (Beckman Coulter, Villepinte, France) and CD95 Pacific Blue (CD95 PB, clone DX2) (Bio-Legend, London, UK), as published previously (10) (Fig. 1). Whole blood was stained using the TQ.Prep workstation and IMMUNOPREP Reagent System (Beckman Coulter) according to manufacturer’s protocol. Cells were subsequently subjected to flow cytometry (Navios Flow Cytometer; Beckman Coulter) and the results were analysed by KALUZA Software (Beckman Coulter). The results are expressed as the percentage of CD95+ cells in the T CD3+CD4+ population.
Fig. 1. Flow cytometry showing a representative sample of low and high expressors of CD95 profiles in CD4+CD95+ circulating T cells.
Comparison of CD95 expression by CD4+ peripheral T lymphocytes (CD4+CD95+/CD4+ ratio) in patients with MF and BLC was performed using standard Student’s t-test. For each predefined threshold-value of the ratio, sensitivity and specificity regarding a definite diagnosis of MF or BLC were calculated, taking into account that: a true positive is a patient with definite MF and a ratio lower than the predefined threshold; a true negative is a patient with BLC and a ratio higher than the predefined threshold; a false positive is a patient with BLC and a ratio lower than the predefined threshold; and false negative is a patient with definite MF and a ratio higher than the predefined threshold. The overall aim of this work was to identify one or more threshold-value(s) of this ratio that might reach a specificity above 90% in adequately discriminating MF from BLC in patients with a well-established diagnosis, and, specifically, to assess whether a ratio above or below the cut-off value(s) under examination is associated with 1 of these 2 subsets of T-cell cutaneous infiltrate with a high specificity regardless of the level of sensitivity. In addition, receiver-operating characteristic (ROC) analysis was performed according to the threshold-values of CD95 expression, in a further attempt to determine the most valuable cut-off value discriminating MF from BLC or BLC from MF.
A total of 330 patients were prospectively included at initial diagnosis between January 2003 and March 2013. Of these, 104 were patients with MF, including 67 with classical, interfollicular MF, 36 with merely or partially folliculotropic MF, and 1 with unspecified MF, all of them staged IA–IB apart from 10 with histologically transformed MF (stage IIB). In the control group, 226 patients with various BLC were included. The patients’ clinical characteristics are summarized in Table I. After a follow-up of 3 years, diagnoses of MF or BLC were confirmed in all patients.
Table I. Patients’ characteristics
The mean raw CD4+CD95+/CD4+ ratio was 55% and 57% (standard deviation (SD) 0.165 and 0.187, respectively; range 0.18–1 and 0.01–0.97, respectively) in the MF group and the control group respectively (p = 0.309). The mean number of CD4+CD95+ circulating lymphocytes was 379/mm3 and 401/mm3 (SD 212 and 264.8/mm3, respectively) in MF and control group, respectively (p = 0.599).
Sensitivity and specificity were calculated for each threshold-value of the ratio, as described above, for MF vs. BLC. Interestingly, CD4+CD95+/CD4+ ratios of 30% and 40% reached a specificity of 91% and 80%, respectively, in identifying definite MF. Data regarding the specificity and sensitivity of various CD4+CD95+/CD4+ ratios in discriminating between MF and BLC are summarized in Table II.
Table II. Sensitivity and specificity for each value of the ratio of CD4+CD95+/CD4+ circulating T-cells
As shown by the receiver operating characteristic (ROC) in Fig. 2, the mean percentage of CD4+CD95+ cells among circulating CD4+ T-cells is not a valuable criterion to discriminate MF versus controls.
Fig. 2. Receiver-operating characteristic (ROC), according to the value of the threshold of CD95 expression. The raw mean values of CD95+ expression in CD4+ T-cells are similar in the MF group and the control group, as shown by an area under the curve (AUC) of 0.5.
The mean CD4+CD95+/CD4+ ratio was statistically lower in folliculotropic mycosis fungoides (fMF) vs. classical MF (p = 0.045), but significantly higher in transformed vs. non-transformed MF (p = 0.017) (Table III).
Table III. Comparison of the ratio of the CD4+CD95+/CD4+ circulating T cells in folliculotropic mycosis fungoides (fMF) vs. classical MF and in transformed MF (TransMF) vs. non-TransMF, using a Student’s t-test
The results of this large-scale study to define a potential new tool to improve diagnosis of MF showed that the CD4+CD95+/CD4+ ratio in peripheral blood T lymphocytes higher than 30% reached a specificity of 91% in identifying definite BLC vs. MF, although overall CD95 expression was not significantly different between the 2 subsets of cutaneous T-cell infiltrates. However, the sensitivity of this threshold-value is very low (5%), suggesting that this blood marker is inefficient in properly identifying most MF patients, but rather favours BLC diagnosis when evaluating a cutaneous T-cell infiltrate where MF might be an eligible option. Thus, the level of CD95 expression by peripheral CD4+ lymphocytes might be added to a multicomponent score of early MF diagnosis, but as a negative factor when exceeding this cut-off of 30%.
In order to further investigate the specific value of this parameter in daily clinical practice, prospective studies are required, addressing initially unspecified lymphocytic T-cell skin infiltrates until a final diagnosis of MF or BLC is reached, and not, as in this pilot study, patients with a definite and predefined diagnosis. Moreover, raw mean values appear to be quite similar in the 2 groups, whereas overall ROC displays an AUC value of 0.5. The lack of overall significant difference between the 2 subsets of patients contrasts with previous studies and this discrepancy is likely to be related to a significantly larger number of patients included in the present study combined with the low sensitivity of the parameter. It must be pointed out that only scarce reports of physiological values of CD95 expression by circulating CD4+ T cells in healthy donors are available in the literature, which largely precludes an interpretation of possible variations in our study compared with normal values, especially regarding a putative relationship with pathomechanisms of the underlying disease. The ratio of CD4+CD95+/CD4+ T cells ranged from 31.9 (SD 10.2) to 52.9 (SD 10.3) in 23 adult blood donors (11).
The expression rate of CD95 appears to be higher in transformed MF vs. non-transformed MF, but this may be related to the re-activation of T cells in this aggressive subset of MF and the possible subsequent expression of CD95 as a marker of activated T cells whether genuinely neoplastic or reactive. Thus, it would be interesting to include a periodic evaluation of CD4+CD95+/CD4+ ratio in the follow-up of patients with MF with an initial low expression of CD95 in circulating T cells, since an increase might reflect, and perhaps portend, an unfavourable outcome.
The 2 groups of patients were not strictly similar regarding age or sex ratio; however, age and sex did not seem to influence the expression of CD95 on CD4+ lymphocytes: Pearson correlation factor was 0.16 for age and the mean percentages of CD95+ were similar in men and women. Furthermore, we did not include an additional control group of healthy individuals because the aim of the study was to propose a potential additional criterion to further differentiate benign vs. malignant lymphocytic skin infiltrates along with other diagnostic items in identifying MF more accurately. Unfortunately, we were not technically able to select morphologically abnormal cells (i.e. suspected Sézary cells) to study a putative correlation between morphological anomalies and CD95 immunophenotyping. The significant differences in fMF vs. classical MF and in transformed vs. non-transformed MF regarding CD95 expression relied on very low number of patients. A further limitation of this study was that it was performed at a single centre.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize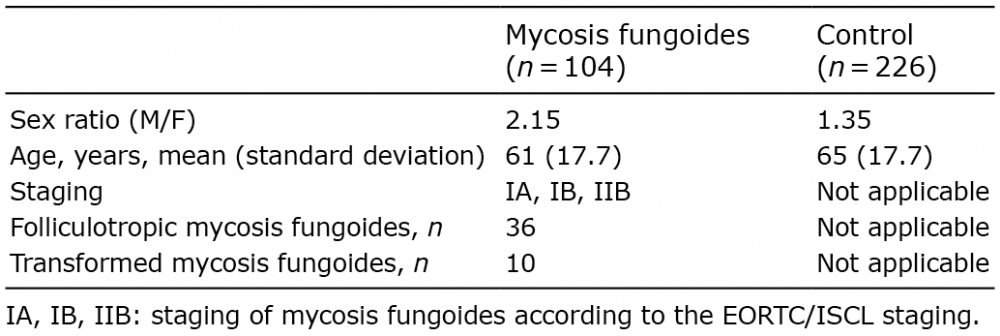 Click to show fullsize
Click to show fullsize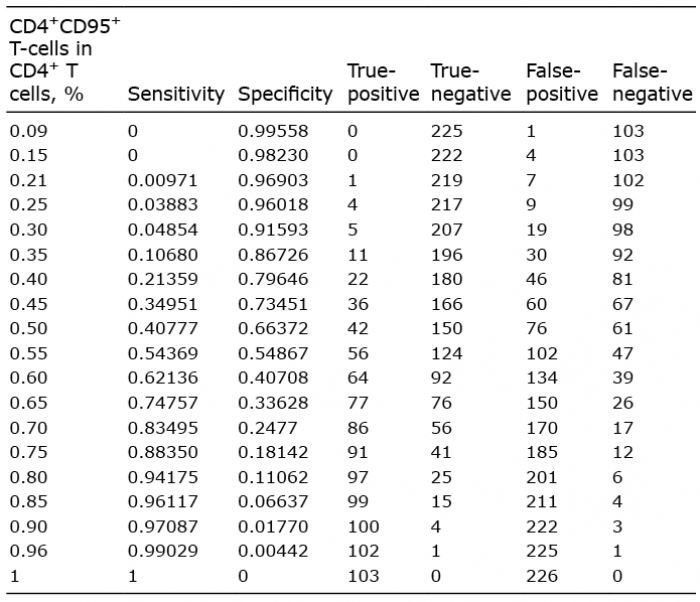 Click to show fullsize
Click to show fullsize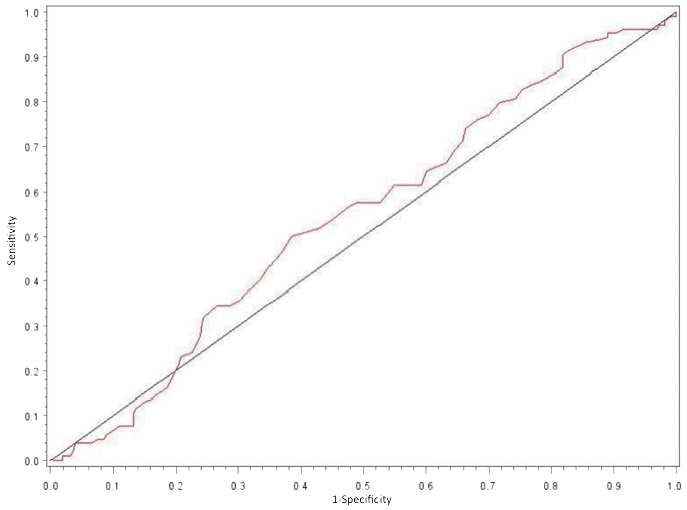 Click to show fullsize
Click to show fullsize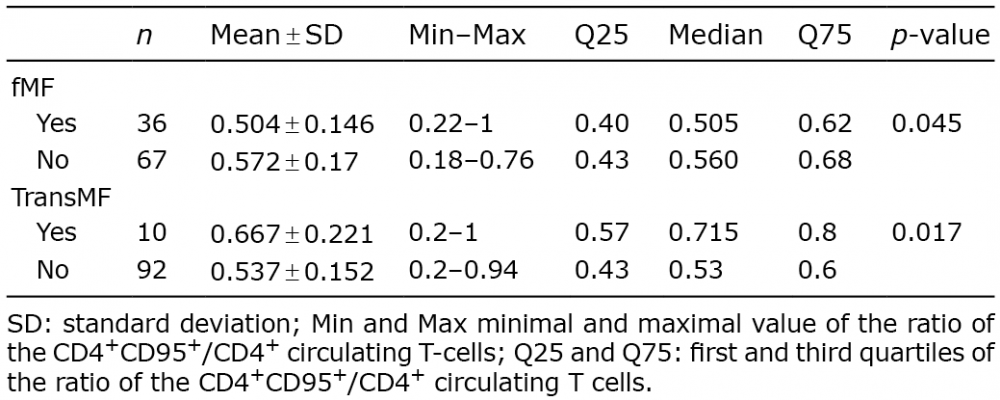 Click to show fullsize
Click to show fullsize