


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Atopic dermatitis (AD) is the most common chronic dermatitis in children. The influence of AD on quality of life of parents of children with AD was studied using the Family Dermatology Life Quality Index (FDLQI). Fifty children with AD were included in the study (age range 2–24 months) together with their parents. Children’s AD was found to influence the quality of life of both parents; however, it had a more significant influence on quality of life of mothers than that of fathers (mean FDLQI: 17.1 ± 5.3 vs. 14.7 ± 5.8 points; p < 0.001). Due to the children’s AD, mothers spent more time caring for them and carried out more household duties. Childhood AD had a greater impact on quality of life of fathers through influence on their work or education. The influence of AD on the quality of life of family members is significant, and this should be taken into account in the therapeutic process.
Key words: atopic dermatitis, quality of life, parents’ quality of life.
Accepted Feb 15, 2017; Epub ahead of print Feb 16, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Jacek Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Ul. Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Atopic dermatitis (AD) is the most common chronic dermatitis in children. Due to the chronic nature of AD and the inconvenience of treatment methods, the condition has a significant influence on patients’ quality of life (QoL). AD often affects the youngest patients (1) and therefore also has an impact on the QoL of parents (2, 3).
Interest in patients’ QoL, including that of dermatological patients, has increased in recent years (4–6). Several tools, mostly self-reported questionnaires, are available to measure the QoL of dermatological patients (7, 8). Numerous studies have confirmed that there is a significant decrease in QoL of patients with AD with reference to both the healthy population and other dermatological or systemic diseases (7, 9). However, there is little research made showing the influence of a child’s disease on other family members. There are a limited number of studies concerning the QoL of families of patients with AD, which show that skin disease in children has a negative impact on the well-being of parents (3, 10, 11). If mothers and fathers perform different roles in families, the influence of AD on their QoL may differ, although previous studies are inconclusive on this point (12, 13). The aim of the current study was to investigate the impact of children with AD on the QoL of both parents, in order to enable a better focus on patients’ and parents’ needs.
The study included the parents of 50 children with AD who were hospitalized in the Department of Paediatrics, Allergology and Cardiology of Wroclaw Medical University, Poland. Patients were recruited consecutively. Inclusion criteria were: written consent of both parents (or of one parent if the second parent did not raise the child) to participate in the study; child’s age between 1 and 24 months; confirmed diagnosis of AD based on clinical manifestation and disease course; no other major skin or systemic diseases that might influence the results of the study; parents are native Polish speakers; and parents were able to understand the questionnaires. There were 36 boys (72%) and 14 girls (28%), age range 2–24 months (mean ± standard deviation (SD) 10.2 ± 6.5 months) included in the study. In the parents’ group there were 50 mothers and 46 fathers (4 patients’ fathers were not in contact with their family). Based on their medical histories it was established that the major caregivers in all children with AD were the mothers.
The Polish language version of the Family Dermatology Life Quality Index (FDLQI) was used to assess the impact of the children’s AD on the parents’ QoL (14, 15). The questionnaire comprises 10 questions concerning the influence of the children’s disease on different fields of life of their family members, such as emotional distress, physical well-being, relationships, other peoples’ reactions, social life, free time, time spent looking after the child, extra housework, work or education, and daily expenditure. Questions concern the influence of the disease on parents’ QoL in the last month. Each question can be answered by choosing 1 out of 4 answers scored 0–3. The maximum score is 30 points and minimum 0 points. The higher the score, the lower the parents’ QoL.
In addition, in order to evaluate the QoL of children with AD the following questionnaire was used: Infant’s Dermatitis Quality Life Index (IDQOL) in the Polish language version (16), in which the answers were given by parents. Both questionnaires were chosen for several reasons: they are validated, are available in Polish, have numerous language versions that enable comparison of the results with those of other authors, they can be applied in different skin conditions, and enable comparisons to be made between AD and other dermatoses. Both questionnaires (FDLQI and IDQOL) were completed separately by mothers and fathers. Whilst the questionnaires were being completed parents were not allowed to communicate with each other. The severity of AD was measured by one of the co-authors (J.M., a paediatrician, allergist) using the Severity Scoring of Atopic Dermatitis (SCORAD) and the Eczema Area and Severity Index (EASI) (17, 18).
All data were analysed with Statistica® 12.0 software for Windows Software. Student’s t-test and Mann–Whitney U test were used, where appropriate. Possible correlations between parameters were measured with Pearson’s correlation test. The statistical significance level was set at 0.05. For multiple comparisons Bonferroni correction was used (in such cases p < 0.005 was considered significant). The post hoc power calculation for comparison of mothers vs. fathers was 56%.
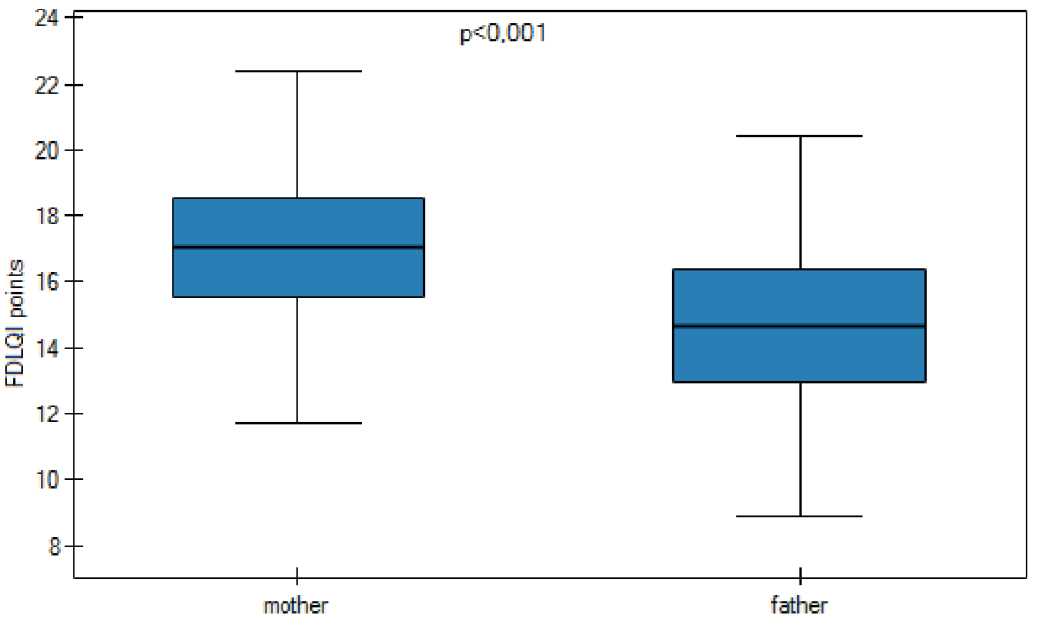
A significant difference was found between the FDLQI for mothers (17.1 ± 5.3 points; range 4.0–28.0 points) and fathers (14.7 ± 5.8 points; range 4.0–27.0 points) (p < 0.001) (Fig. 1). In addition, there was a statistically significant correlation between the mothers’ and fathers’ QoL, measured with FDLQI (r = 0.73, p < 0.001). Detailed results of the impact of children’s AD on mothers’ and fathers’ QoL are shown in Table I. Although categorization for FDLQI is missing, by analogy with the Dermatology Life Quality Index it could be suggested that children’s AD has a very large negative effect (scoring > 10 points) on parents’ QoL, for both mothers and fathers. Both parents reported that their children’s skin disease mostly had a significant impact on household expenditure, as well as a negative influence on their emotional and physical well-being.
Fig. 1. Family Dermatology Life Quality Index (FDLQI) scoring of parents of children with atopic dermatitis (AD) indicating significantly higher impact of AD on quality of life of mothers (n=46) compared to fathers (n=46) (results demonstrated as mean ± standard errors of means and standard deviations).
Table I. Impact of children’s atopic dermatitis on the quality of life of mothers and fathers indicating generally higher impairment of various aspects of quality of life in mothers compared to fathers (for details see the text)
Due to their child’s AD mothers spent more time taking care of the children by nursing or giving medical treatment and carrying out more household duties (Table I). There was a trend towards greater impact of the disease on various aspects of the mothers’ well-being (tiredness, exhaustion, triggering of health problems, sleep disorders, relaxation) than the fathers’ well-being. Mothers had slightly more emotional anguish and experienced more inconvenience connected with other people’s reaction to the children’s disease than did fathers, but the difference was not statistically significant (Table I). It was noted that children’s AD had a slightly greater impact on the QoL of fathers with regard to the influence of their work or education (need for a day off, inability to work, decrease in the number of hours worked, problems with people at work). The children’s AD had a similar influence on the social life, spare time and daily expenditure of both parents.
Correlations between mothers’ and fathers’ FDLQI and the severity of the children’s AD and QoL are shown in Table II. A statistically significant correlation was found between the mothers’ QoL assessed with FDLQI and the QoL of the children with AD evaluated with IDQOL (r = 0.79; p < 0.001). Similarly, a statistically significant correlation was found between the fathers’ FDLQI scoring and IDQOL (r = 0.67; p < 0.001). Regarding disease activity and parents’ QoL statistically significant positive correlations were found between disease severity and FDLQI scoring for both mothers (SCORAD: r = 0.48; p < 0.001; and EASI: r = 0.34; p = 0.02) and fathers (SCORAD: r = 0.44; p = 0.002; and EASI: r = 0.33; p = 0.03).
Table II. Correlations between childrens’ parameter and Family Dermatology Life Quality Index (FDLQI) of mothers and fathers and the studied parameters
This study evaluated the impact of children’s AD on parent’s QoL using the FDLQI. Children’s AD influenced mothers’ QoL most by increasing daily expenditure. It had a less significant impact on the mothers’ work or education. The children’s AD also influenced the fathers’ QoL most by increasing daily household expenditure; least significant for fathers was other people’s reaction to the children’s AD. A meaningful relationship was observed between mothers’ and fathers’ FDLQI. The reduction in mother’s QoL correlated significantly with the reduction in father’s QoL. However, the children’s AD had a greater impact on the mothers’ QoL than on the fathers QoL.
Children’s AD had a comparable influence on both parents in terms of their social life, spare time, and daily expenditure. This may be connected with current lifestyles, in which sharing duties is more equal than in the past. Spending time together is essential, especially due to the fast pace of life. Moreover, planning expenses together is a prerequisite for good family relations. Mothers tend to spend more time taking care of ill children, through nursing or providing medical treatment. Furthermore, due to their children’s AD they carried out more household duties. In addition, AD had a greater influence on the mothers’ relationships with other people compared with the fathers’ relationships with other people. It should be noted that in Polish culture and tradition there is deeply embedded model of mothers taking care of the home and children. This division of roles is followed in many families, despite changing lifestyles and a move away from traditional family models of mothers sacrificing their career or education to bringing up children. Thus, the mother is still the parent most affected by their child’s AD. In many Western European countries the family model might differ significantly from the Polish one; thus, further research is needed into the influence of children’s AD on the QoL of parents in other countries.
Regarding fathers, the children’s AD had a greater impact on QoL only through influencing their work or education (e.g. needing time off work, being unable to work, decreased hours worked, problems with people at work). In Polish tradition the father is perceived as the main earner. Despite changing trends, Polish men earn more than women and have a greater input to family budget.
A study by Chernyshov (13) into a group of children with AD under 4 years old and their parents estimated family QoL using the Dermatitis Family Impact (DFI) measure. No statistically significant differences were found in family QoL with regard to the sex of the parents completing the questionnaire regarding influence on housework, food preparation and feeding, other family members’ sleep patterns, ways of spending free time, time for family shopping, costs connected with treatment, tiredness or exhaustion, emotional stress, inner family relationship, and the influence of help in child treatment on the carer. Differences between our results and the Chernyshov study (13) may reflect several aspects: the different and smaller population analysed in the Chernyshov study (i.e. the smaller power to detect significant differences), cultural differences between Polish and Ukrainian people, and different methodologies. Our results are more convergent with Holm et al. (12), who also showed that mothers usually scored higher than fathers while assessing their QoL related to skin disease of their children. Another study observed that mothers caring for children with AD lost a median of 39 min of sleep per night, while fathers lost 45 min sleep per night. This compared with a median of 0 min sleep lost by parents who had children with asthma (19).
There are only a few published studies using the FDLQI questionnaire to estimate the QoL of patients’ families for other dermatitis. Tadros et al. (20), in a study conducted in Greece on patients with psoriasis and their families, showed a reduction in family QoL according to the FDLQI questionnaire, which correlated positively with the reduction in patients’ QoL as assessed with the DLQI. In another study Bin Saif et al. (21) used FDLQI to estimate the QoL of patients with vitiligo in Saudi Arabia. They showed a significant impact of the disease on family QoL with the FDLQI questionnaire, and positive dependency on patients’ QoL according to the DLQI. The most highly influenced aspects of family members’ life were: emotional state, care, impact on physical state, other people reactions to disease, and impact on social life.
In the current study correlational analysis was performed between FDLQI and disease severity evaluated with SCORAD and EASI. It has been shown that increased disease severity was associated with a greater impairment in QoL in both mothers and fathers. A positive correlation between the severity of AD in children evaluated with SCORAD and parents’ QoL was found in previous studies using only the DFI (3, 22–25). The current study evaluated the correlation between both mothers’ and fathers’ QoL, assessed using the FDLQI, and the children’s QoL, assessed with the IDLQI. It was found that the more impaired was the QoL of the child with AD, the lower was the mothers’ and fathers’ QoL. Other studies have shown a positive correlation between the QoL of children with AD, as assessed with the IDLQI and parents’ QoL according to the DFI (15, 26–28).
This study has some limitations, and the results must be interpreted with caution. The study group is rather small; larger study populations are needed to confirm these observations. The study was performed in Poland, thus the results do not necessarily reflect the situation in other countries. Future research should also take into account culture and traditional family models. Finally, the mothers in the current study were the primary caregivers, which may have further influenced the results. Nevertheless, the impact of dermatitis, including AD, on the QoL of family members appears to be meaningful, and therefore more care needs to be taken treating AD as well as in further research on this matter.


 Click to show fullsize
Click to show fullsize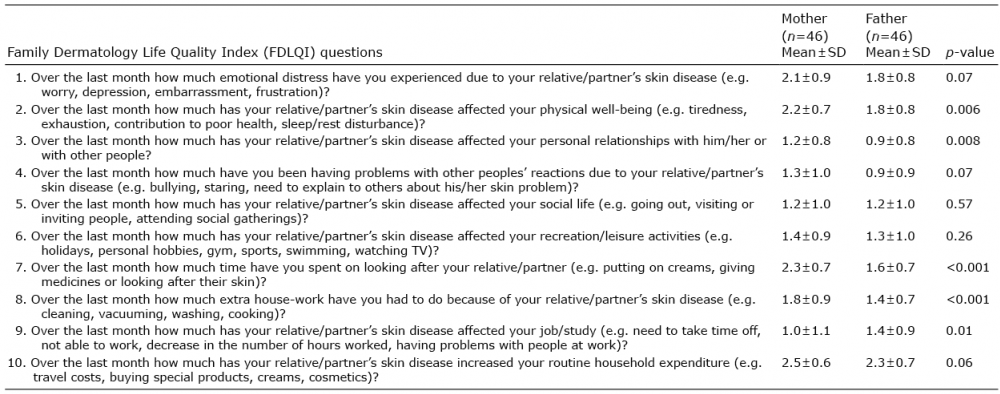 Click to show fullsize
Click to show fullsize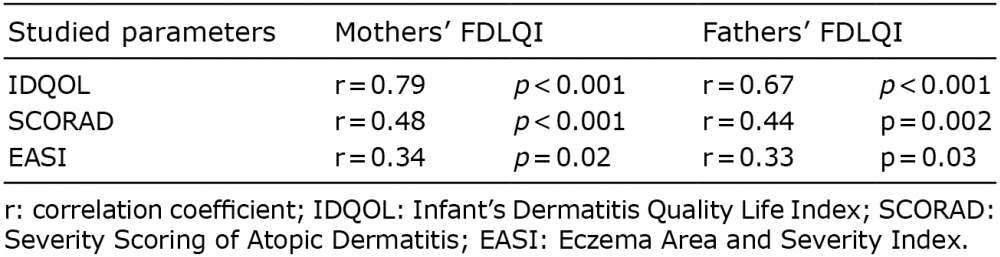 Click to show fullsize
Click to show fullsize