


1Department of Dermatology and Venereology, and 2Department of Pathology and Cytology, Malmö University Hospital, Jan Waldenströms gata 18, SE-21428, Malmö, Sweden. E-mail: gregtheodosiou@yahoo.com, Grigorios.Theodosiou@skane.se
Accepted Feb 20, 2017; Epub ahead of print Feb 20, 2017
Naevoid malignant melanoma (NMM) is a rare, but distinctive, variant of melanoma, which is, clinically and histologically, easily mistaken for a melanocytic naevus; this can have devastating consequences for the patient due to delay in appropriate treatment (1–3).
Epidemiologically NMM has a male predominance. Age at diagnosis is often the 6th decade of life (mean age: 51–57 years) (4–8). A case of a 4.5-year-old girl with metastatic naevoid melanoma has also been reported (9).
Clinically, NMM presents as a variously pigmented papillomatous or dome-shaped papule or nodule that is often >1 cm in diameter and is located on the trunk and the limbs. The verrucous appearance of the naevoid melanoma can deceptively evoke a benign diagnosis of dermal or compound naevus, seborrhoeic keratosis or papilloma (3, 8, 10–13).
Histologically, subtle clues that enable NMM to be differentiated from benign melanocytic lesions are the presence of multiple dermal mitoses, often deep and atypical, nucleolar prominence, subtle pleomorphism, slight asymmetry and impaired circumscription (5, 7, 14).
A healthy 49-year-old Caucasian man, with no relevant dermatological history, was referred to our department due to a lesion on the dorsal side of his left leg. There was no family history of skin cancer. The patient was certain that the lesion had appeared more than 10 years prior to referral. Five years prior to referral the patient had been seen by a dermatologist, who conducted a shave biopsy with curettage of part of the lesion. The histopathological examination was consistent with a benign naevus, and no follow-up was offered. The lesion, however, increased further in size over subsequent years and the patient was referred to our department for a second opinion.
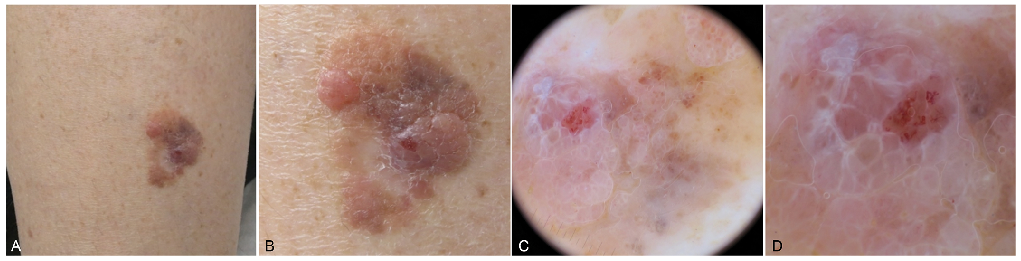
Clinical examination revealed a 2×2 cm, multicolour papillomatous lesion, which appeared to be comprised of distinct areas of pigmentation, and to exhibit a typical verrucous appearance (Fig. 1A, B).
Fig. 1. (A) A multicolour papillomatous plaque on the patient’s leg. (B) Close-up of the multicolour papillomatous lesion, which appears to be composed of distinct parts. A small ulceration and a whitish area after the previous shave biopsy are also observed. (C) Global dermatoscopic assessment: pattern of lines, of dots, of clods, structureless pattern. Multiple colours: white, brown, red, grey. (D) Clues to melanoma; white lines, polymorphous vessels, eccentric structureless zones, grey dots and clods.
Dermatoscopic evaluation of the lesion revealed the presence of multiple patterns (Fig. 1C, D). Differential diagnosis of the clinical image included seborrhoeic keratosis, compound naevus as well as malignant melanoma. Dermatoscopic findings, however, were not consistent with a benign diagnosis and the decision to surgically excise the entire lesion was made. Histopathological examination of the excised tissue revealed a nodular expansile tumour with polypoid architecture in the upper dermis (Fig. 2). A diagnosis of NMM, with a Breslow thickness of 2.1 mm and a mitotic rate 5/mm2, stage pT3a, Clark III was rendered. Wide local excision was performed, as well as sentinel lymph node biopsy, which was negative. The patient did not undergo further examinations. At follow-up, during the first year post-treatment there is no reported recurrent disease, locoregional or distant metastases.
Fig. 2. (a) Scanning magnification of the whole lesion, haematoxylin and eosin (H&E) ×2. (b) Expansile polypoid dermal tumour with thinning of epidermis, H&E ×4. (c) Patchy HMB45 positivity in the dermal melanocytes both in the superficial and deep aspects of the lesion, HMB 45 ×4. (d) High magnification shows nested melanocytes with slightly enlarged hyperchromatic and angulated nuclei with scattered prominent nucleoli and 1 mitotic figure, H&E ×40. (e) Double-staining with Melan A/PHH3 shows scattered melanocytic nuclei with genuine mitotic activity, ×10. (f) Double-staining with Melan A/Ki 67 shows 10% Ki 67 positivity in hot-spots, ×10.
Levene (1) first described in 1980 the existence of a rare variant of melanoma, namely “verrucous and pseudonaevoid melanoma”. Schmoeckel et al. (2) first coined the term “naevoid malignant melanoma” in 1985, describing 33 patients with malignant melanomas with histological features suggestive of benign melanocytic lesions followed for at least 5 years.
In a clinicopathological study of 20 cases conducted by Bleessing et al. (3), NMM occurred most often on the back and the limbs of male patients, who had a mean age of 57 years. Clinical diagnosis of benign lesions was made in over 50% of cases, while 10% of cases were initially diagnosed histologically as benign.
In a morphological study of 20 cases (4) with a follow-up of at least 3 years, 4 tumours recurred and 3 metastasized with fatal outcomes. The mean Breslow thickness was 2.5 mm in this study. No difference in terms of prognosis was found between NMM and ordinary malignant melanoma.
McNutt et al. (5) have emphasized that NMMs mimic ordinary compound or dermal naevi when the tumour cells are small, or Spitz naevi when the cells are large. The pattern of HMB45 staining was found to be strong in the dermal component of the naevoid melanomas, while in naevi, there is less intense staining in the base of the lesion (5, 6). Staining with a proliferation marker, such as cyclin (PCNA) or Ki-67 (with MIB-1 antibody) can further help in distinguishing a NMM from a Spitz’s naevus (NMMs strong nuclear staining throughout the lesion; Spitz’s naevi stronger staining at the top).
The term “small cell malignant melanoma” is often used to describe the small cell variant of NMM resembling a benign naevus without an intraepidermal component.
However, some authors use this term for cases which possess a lentiginous intraepidermal pattern. In one such study 80% of the lesions developed in individuals over the age of 50 years and there was a 2:1 male predominance, with the majority of the tumours in men (58%) occurring on the back (7).
A recent multicentre study of the International Dermo-scopy Society (8) assessed the clinical and dermatoscopic features of 27 cases of NMM, clinically presenting as nodules, plaques or papules. The lesions were identified as naevus-like tumours (48%), amelanotic tumours (30%), and tumours with multicomponent pattern (15%). Two cases (7%) could not be classified into any pattern. Male predominance and a mean age of 51.5 years were observed in this study.
The lesion reported here presented as a lightly pigmented papillomatous plaque. The history and clinical appearance evoked a differential diagnosis of seborrhoeic keratosis, warty melanocytic naevus and malignant melanoma. We had to decide whether to take an incisional or an excisional biopsy or just to follow-up the patient.
Dermatoscopic evaluation of the lesion revealed a “chaotic” picture with multiple patterns and colours arranged asymmetrically. Even clues to melanoma, according to the “revised pattern analysis” were found. The global dermatoscopic assessment was that of a malignant tumour. The discrepancy between the clinical and dermatoscopic picture raised the suspicion of malignant melanoma and led us to surgically remove the entire lesion.


 Click to show fullsize
Click to show fullsize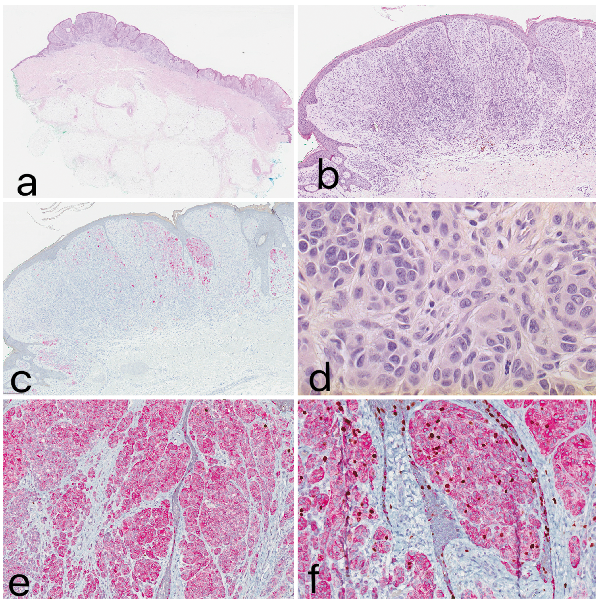 Click to show fullsize
Click to show fullsize