


1Department of Dermatology, and 2Division of Clinical Investigation, Shinshu Univerisity School of Medicine, 3-1-1 Asahi, Matsumoto, Nagano, 390-8621, Japan. E-mail: ykiniwa@shinshu-u.ac.jp
Accepted Feb 20, 2017; Epub ahead of print Feb 20, 2017
Mucin 1 (MUC1), a member of the mucin family, is a highly glycosylated transmembrane protein normally present on the luminal surface of secretory glands (1). Overexpression of MUC1 in tumour cells and elevated serum MUC1 level have been reported in patients with cutaneous T-cell lymphoma (CTCL) (2, 3). We report here a patient with increased serum MUC1 level and aberrant MUC1 expression in the tumour cells of mycosis fungoides (MF), the most common subtype of primary cutaneous T-cell lymphoma.
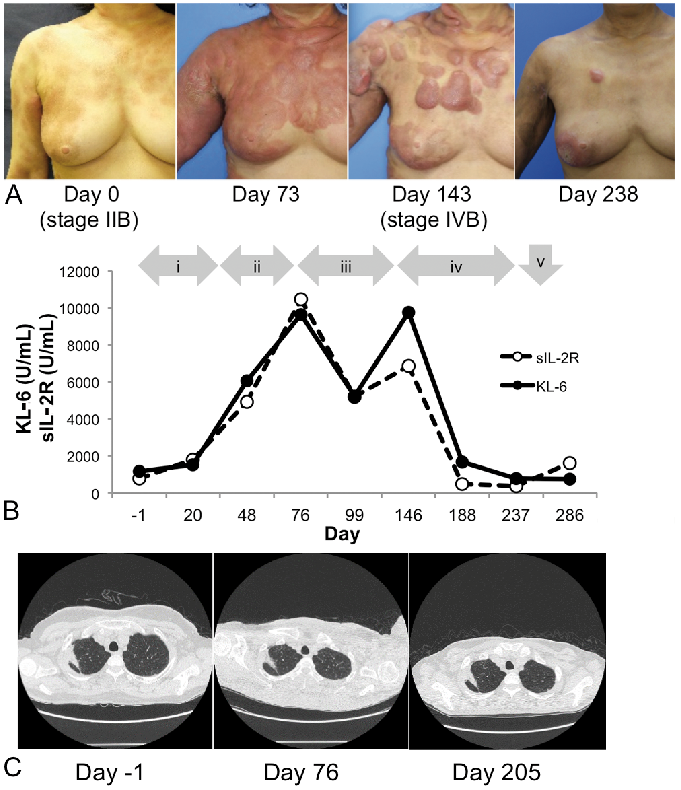
A 53-year-old woman with a 5-year history of MF visited our hospital. Her disease had progressed to tumour-stage (T3N0M0, stage IIB) despite multiple treatments, including psoralen plus ultraviolet-A phototherapy, local radiation, total-body electron-beam radiation, vorinostat and etoposide. Serum KL-6 (Krebs von den Lungen-6, a biomarker of interstitial pneumonia) was measured prior to administration of intravenous interferon (IFN)-γ, which occasionally leads to interstitial pneumonia. KL-6 is an epitope located in the N-terminal domain of MUC1. Her serum level was high, 1,171 U/ml (normal range 105–435 U/ml) (Fig. 1A, B); however, computed tomography (CT) showed no significant findings in her lungs, except radiation pneumonitis in the right lung (Fig. 1C). She was treated with IFN-γ (Day 0), followed by mogamulizumab and gemcitabine. Despite these treatments, new lesions appeared in the lymph nodes and spleen on day 143 (T3NXM1, stage IVB). Her serum KL-6 level increased to 9,650 U/ml as the disease progressed on day 146. After 5 courses of CHOP (a combination therapy of cyclophosphamide, doxorubicin, vincristine and prednisolone), serum levels of soluble interleukin-2 receptor (sIL-2R) and KL-6 decreased, together with clinical improvement in lymphoma lesions on day 238. Both KL-6 and sIL-2R reflected the patient’s clinical condition. Interstitial pneumonia did not occur during the course of treatment (Fig. 1C). She underwent allogeneic bone marrow transplantation. However, her skin lesions worsened 14 days after the transplantation.
Fig. 1. Clinical characteristics and KL-6/sIL2R time course. (A) Clinical findings of skin lesions. Day 0: initiation date of intravenous interferon (IFN)-γ. (B) Krebs von den Lungen-6 (KL-6) and sIL-2R levels. The patient was treated with: (i) recombinant IFN-γ, followed by: (ii) mogamulizumab; (iii) gemcitabine; (iv) a combination of cyclophosphamide, doxorubicin, vincristine and prednisolone; and (v) bone marrow transplantation. (C) Computed tomography did not reveal any significant alterations, except for radiation pneumonitis in the right lung.
Skin biopsy showed CD4-positive lym-phoma cell infiltration in both the epidermis and dermis when the patient was Stage IIB. MUC1 positive cells were sparse in those lymphoma cells by immunohistochemical staining using a KL-6 antibody (Fig. 2A–C). The relapsed lesions exhibited a dense infiltrate of CD4-positive lymphoma cells in the dermis, most of which expressed MUC1 on the cell membranes (Fig. 2D–F). The ratio of MUC1-positive cells in CD4-positive cells was higher in the relapsed lesions (91.2% vs. 38.5%).
Fig. 2. Immunohistochemical findings in the present case. (A–C) Skin lesions biopsied 5 years before interferon (IFN)-γ therapy (stage IIB). (D–F) Skin lesions biopsied after bone marrow transplantation (stage IVB). (A, D) Haematoxylin and eosin staining. (B, E) Immunostaining of CD4. (C, F) Immunostaining for mucin 1 (MUC1). Original magnification: ×400.
MUC1 is associated with overexpression, aberrant intracellular localization and alteration of glycosylation patterns in epithelial carcinomas, including breast, lung and pancreatic cancers (1). MUC1 may contribute to cell proliferation, survival, drug resistance and immune escape (1). MUC1 is also aberrantly expressed in haematological malignancies, especially in myeloma (1). However, some reports have demonstrated involvement of MUC1 in T-cell lymphomas including adult T-cell leukaemia/lymphoma, anaplastic large T-cell lymphoma and CTCL (4–6). The current case report revealed MUC1 expression in tumour cells of MF. Interestingly, the ratio of MUC1-positive cells increased in the skin lesions with disease progression. Furthermore, a MUC1 epitope, KL-6, was increased in association with clinical condition and sIL-2R. In the current case it is likely that MUC1 flowed out from MF cells into the peripheral blood with disease progression. Therefore, MUC1 may be a useful biomarker for disease progression. These findings highlight novel malignant features of MF.
Anti-KL-6 antibody was kindly provided by Professor Hiroyoshi Ota, Department of Biomedical Laboratory Sciences, School of Health Sciences, Shinshu University School of Medicine.
This study was approved by the Institutional Review Board of Shinshu University School of Medicine.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize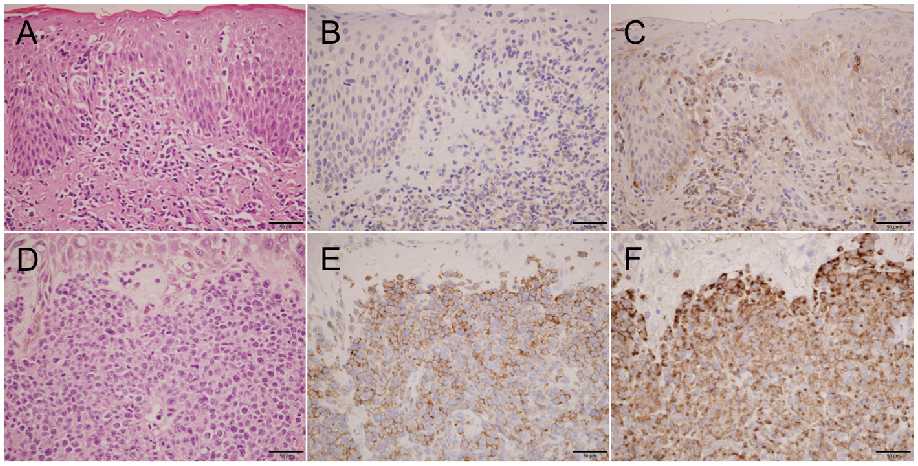 Click to show fullsize
Click to show fullsize