


Department of Dermatology, Hospital Clinic of Barcelona, Barcelona, Spain
Li-Fraumeni syndrome (LFS) is a rare autosomal dominant disorder caused by a mutation in the p53 gene. Melanoma is considered to be a rare, controversial component of LFS. The aim of this study is to describe the utility of systematic screening for melanoma in patients with LFS and atypical mole syndrome. Two 28-year-old identical twin sisters with LFS and atypical moles were monitored by physical examination, total-body digital photography and dermoscopy be-tween 2006 and 2014. A total of 117, predominantly dark-brown, reticular naevi were identified on case 1 and 105 on case 2. Excisions were performed during the evaluation period of 1 in-situ melanoma and 3 basal cell carcinomas in case 1, and 1 in-situ melanoma and 1 early invasive melanoma in case 2. The remaining melanocytic lesions in both patients were stable during follow-up. The 3 melanomas were new atypical lesions detected with total-body photography and dermoscopy. In conclusion, monitoring LFS patients with total-body photography and dermoscopy may be useful to detect early melanoma.
Key words: familial melanoma; Li-Fraumeni syndrome; atypical mole syndrome; digital total-body; photography; dermo-scopy; confocal microscopy.
Accepted Feb 20, 2017; Epub ahead of print Feb 20, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Priscila Giavedoni, Department of Dermatology, Hospital Clinic of Barcelona, ES-08012 Barcelona, Spain. E-mail: giavedonip@gmail.com
Li-Fraumeni syndrome (LFS) was initially described in 1969 (1). In 1990, the p53 tumour suppressor gene was discovered as the most common underlying genetic abnormality in LFS (2). LFS is an autosomal dominant syndrome in which members of the same family experience multiple cancers, beginning at a young age. Many malignancies have been associated with the p53 mutation; including soft tissue sarcomas, osteosarcoma, breast cancer, brain cancer, leukaemia, multiple myeloma and ovarian cancer (3). The association of melanoma with familial cancer syndromes was first reported in 1987 and, specifically, with LFS in 2011, when 5 melanomas were reported in a single patient with a heterozygous germline mutation for p53 (4, 5). The authors note that the association of melanoma with LFS has been sporadic and controversial (4). On review of the literature we found no guidelines or reports of systematic follow-up of pigmented skin tumours in patients with LFS.
We report here the systematic dermatological follow-up of identical twin sisters with LFS and melanoma.
Two identical twin sisters, 28 years old, both with a diagnosis of LFS and atypical moles were included in a follow-up protocol in the Melanoma Unit of the Hospital Clinic of Barcelona. They had been diagnosed with LFS according to clinical criteria (6, 7) and in patient 1 who accepted genetic testing, a p53 mutation was confirmed. Both sisters had wild-type CDKN2A genes. A dermatologist completed a standardized full-skin examination, excluding the genital area. This standardized skin examination with naevus count protocol has been validated previously and found to be reproducible (8, 9). Naevi were recorded by size in 3 categories (> 2 and < 5 mm, > 5 and < 10 mm and > 10 mm). Skin type was assessed according to the Fitzpatrick classification, as described previously (10). Hair and eye colour were also recorded. Physical examination, dermoscopy with a hand-held dermatoscope of all pigmented lesions, and digital photography, including total-body photography and photographic dermoscopy was completed every 3–6 months for the 2 patients, from 2006 to 2014, according to the previously reported 2-step method (11). A commercially available device for digital photography was used in these 2 cases (Molemax TM, Derma Instruments, Vienna, Austria). New lesions or changes in pigmented lesions were systematically recorded. New lesions with atypia, detected with total-body photography, or atypical changes in pre-existing lesions, detected with dermoscopy, were biopsied.
Case 1: Had a melanoma in situ of the right ankle diagnosed in 2004, and multiple cancers, including: breast, adrenal and osteosarcoma of the rib. She began digital photographic monitoring in 2006. The patient had had moderate sun exposure in her childhood/adolescence, and had sunburned at least 5 times with peeling, but no blistering. She had also used tanning beds approximately 10 times when she was approximately 19 years old. She reported adequate sun protection at the time of her first visit to our centre. Fitzpatrick skin type III, brown eyes and brown hair.
Case 2: Had a history of ductal carcinoma in-situ of the breast diagnosed in 2003. She had intermediate sun exposure in her childhood/adolescence, with sunburns at least 10 times with peeling, but no blistering. She had used tanning beds approximately 5 times when she was approximately 19 years old. She reported adequate sun protection at the time of her first visit to our centre. Fitzpatrick skin type III with green eyes and brown hair.
The sisters’ father had cancer of unknown primary with metastases to the liver, bone and lungs. They had a paternal uncle with a skin cancer of uncertain type, possibly melanoma, and another with an unknown cancer diagnosis. Their paternal aunt had ocular melanoma. Their paternal grandfather had a tumour in his vena cava and a paternal cousin had a tumour of the central nervous system.
Case 1. This patient had 103 naevi between 2 and 5 mm in size and 14 naevi between 5 and 10 mm in size. Many of these melanocytic lesions appeared clinically atypical. Most of these naevi were brown with a reticular dermoscopic pattern. The patient’s skin was noted to have some solar lentigines and mild solar elastosis. In April 2007 a small, pigmented lesion was detected on the back and dermoscopy showed multiple blue-grey globules, large grey-blue ovoid nests and spoke-wheel areas. In this lesion, confocal microscopy examination with Vivascope 1500 (Caliber, Rochester, NY) clearly showed hypo-reflective round tumour islands, palisading, peripheral clefting and melanophages. A biopsy showed a pigmented nodular basal cell carcinoma (BCC).
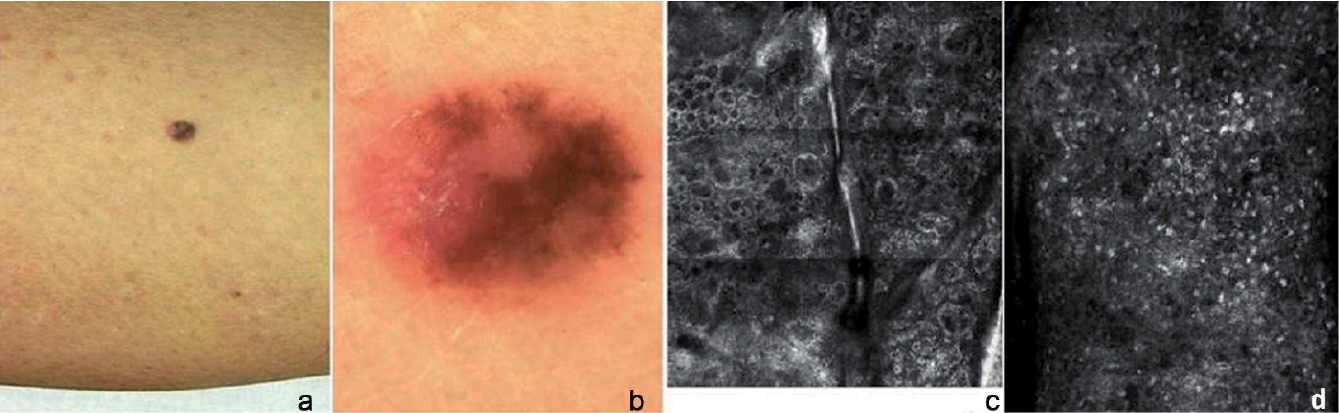
In February 2011 dermoscopy revealed 2 new lesions on the right pectoral and right infraclavicular chest, with multiple blue-grey globules and arborizing telangiectasias. A biopsy showed superficial BCC in both lesions. A new 3-mm diameter lesion was detected with total-body photography on the left lower leg in April 2013 (Fig. 1a).
Fig. 1. Case 1. (a) Clinical photograph left lower leg, April 2013. (b) Dermoscopy of left lower leg lesion. Confocal microscopy of left lower leg lesion. (c) Atypical cells in the dermal-epidermal junction, without nests and plump cells in the dermal papillae suggestive of a thin melanoma (mosaic covering 1.250 × 1.5 mm). (d) Atypical honeycomb pattern, pagetoid cells, atypical cobblestone (single image 500 × 500 micras).
Dermoscopy revealed an asymmetrical multicomponent pattern and areas of regression (Fig. 1b). In this lesion confocal microscopy revealed an atypical honeycomb pattern, pagetoid cells, atypical cobblestone and atypical cells in the dermal-epidermal junction, without nests and plump cells in the dermal papillae suggestive of a thin melanoma (Fig. 1c, d). The pathological diagnosis was melanoma in-situ with regression.
Pancreatic cancer was detected in 2013, which progressed to the liver, resulting in the patient’s death in April 2014.
Case 2. This patient presented with 90 naevi between 2 and 5 mm and 15 naevi between 5 and 10 mm in size. Most of her naevi were dark brown with a reticular dermoscopic pattern. Like her sister, her skin showed signs of photodamage, with solar lentigines and mild solar elastosis in sun-exposed areas. In March 2009, 2 new small melanocytic lesions were detected on the right leg and right upper back. Both lesions exhibited atypical pigmented network and areas of hyperpigmentation on dermoscopy. With close follow-up, the 2 lesions had increased in size by May 2009. These 2 lesions were biopsied and diagnosed respectively as melanoma in-situ on the right leg (Fig. 2a, b) and early invasive melanoma of the right subscapular back with a Breslow depth of 0.6 mm (Fig. 2c, d).
Fig. 2. Case 2. (a, b) In-situ melanoma on the right leg (March 2009 and May 2009, respectively). (c, d). Early invasive melanoma on the right subscapular back (March 2009 and May 2009, respectively) (Size 300 dpi).
LFS is an autosomal dominant disorder caused by a mutation in the p53 tumour suppressor gene that is associated with several malignancies presenting at a young age. The diagnosis of “classic” LFS is based on the following criteria: patients present with a sarcoma before the age of 45 years and a first-degree relative with any cancer before the age of 45 years and another first or second degree relative with any cancer before the age of 45 years or a sarcoma at any age (6, 7). The age of onset of the first cancer is similar in male and female patients. In patients with the p53 mutation, the sex-ratio of tumours overall has been reported to be similar, with the exception of sex-specific cancers and a prevalence of adrenal cortical carcinomas in women (3.7:1) (6). The excess of tumours in women is due to their predisposition to breast cancer (6). The initial descriptive work by Li & Fraumeni (1) did not find an association of melanoma in LFS. To date, only a sporadic and controversial association has been reported between LFS and single cases of melanoma (4, 5, 12, 13). The risk of melanoma may be increased in LFS, but reports of skin cancer are not always included in many study cases, given the poor prognosis of other cancers in this population and the patient’s short life expectancy. These factors may explain an under-estimated prevalence of skin cancer in LFS. Table SI lists previously reported cases of LFS with melanoma where the clinical and pathological characteristics were reported. Two of the 7 reported melanomas in the table occurred in sites of prior radiation. It is possible that there is an increased susceptibility to ionizing radiation in patients with LFS.
Hartley et al. (5) described 7 cases of melanoma in the close relatives of 94 children with a total of 76 osteosarcomas, 10 chondrosarcomas and 9 adrenal cortical carcinomas. This study reported in 1987 lacks genetic data. Germline mutations of p53, and 2 different BRCA2 mutations, have been reported in 2 patients with melanoma and breast cancer (14). In a study of the prevalence of germline p53 mutations in children with adrenocortical tumours, choroid plexus tumours, and rhabdomyosarcoma, there were 2 observed cases of melanoma in the p53 positive or unknown group aged 0–49 years with an expected rate noted to be 0.2 in the general population (15). This was an increase in the standardized incidence ratio, at 8.7%, which was statistically significant (15).
Atypical mole syndrome (AMS) is characterized by the presence of multiple clinically atypical naevi; however, some authors consider a minimum number of 3 or 5 lesions and others do not clarify the number of lesions required to define this syndrome (16). The relative risk (RR) of melanoma increases in a patient with only one atypical naevus (RR=1.60; 95% confidence interval (95% CI): 1.38, 1.85), increasing to 10.49 (95% CI: 5.05, 21.76) for 5 atypical naevi (17). These high-risk patients are those who benefit with digital follow-up (16). The risk of melanoma in patients with LFS and AMS has not been described, but these patients may have a higher risk than those with LFS or AMS only.
Although we can not quantify sun exposure of our patients, previous studies have described a higher risk for melanoma for intermittent sun exposure compared with chronic sun exposure (RR=1.46; 95% CI: 1.19, 1.79 and RR=1.09; 95% CI: 0.86, 1.37 for intermittent and chronic sun exposure, respectively) (17).
Cancer screening for patients with LFS is controversial, but it is supported based on the accuracy of the screening test regarding early detection of cancer, the risk or potential side-effects from the test and the associated cost. French guidelines include an annual physical examination, magnetic resonance imaging (MRI) of the breast annually after the age of 20 years of age, and avoidance of radiation, including X-rays and computed tomography scans. They also suggest having a discussion about prenatal/preimplantation genetic testing (7). A trial called the Lifscreen Project is planned to evaluate a whole body MRI, including brain and breast, physical examination, abdominal ultrasound and breast ultrasound in women with p53 mutations from the age of 20 years (7).
The United States National Comprehensive Cancer Network consensus guidelines for cancer screening in LFS include monthly breast self-examinations beginning at age 18 years, physician examination every 6 months after age 20 years or 5–10 years before the first breast malignancy found in the family, mammograms or MRI of the breast after the age of 20 years or earlier depending on the age at diagnosis of breast cancer in other family members. They suggest consideration of prophylactic mastectomy in selected cases after evaluating the risks and benefits. They also suggest annual physical examinations, including careful neurological and skin assessment, colonoscopy every 2–5 years, and other specific screening based on family history (7).
These results indicate that digital monitoring in patients with LFS and multiple naevi facilitates early diagnosis of melanoma. This method of screening is not suggested in current guidelines, as noted above. Three BCCs were diagnosed in these 2 patients in our clinic, all before the age of 35 years. In Spain the mean ± SD age at diagnosis of non-melanoma skin cancer is 67.3 ± 13.5 years (18). The association of LFS and BCC is more rarely reported than melanoma and is more controversial. Total-body skin examination with total-body photography and dermoscopy was useful for early diagnosis of BCC as well as melanoma in our patients. In patients with LFS, the frequency of atypical melanocytic lesions has not been reported. The combination of LFS and AMS may be a marker for increased risk of melanoma similar to other genodermatoses, such as xeroderma pigmentosum or familial melanoma syndrome. Dermoscopic examination of all skin lesions in patients with LFS by an experienced dermatologist is suggested, since this method has been shown to be effective in the diagnosis of melanoma as recommended by experts in evidence-based clinical international guidelines (19). Digital photographic dermoscopy monitoring has shown its utility for the early detection of melanomas in high-risk patients with AMS (16). This follow-up allows a significant reduction in excisions of benign lesions in patients with multiple atypical lesions (16), such as our patients. Regular digital follow-up with total-body photography and dermoscopy may help to detect subtle changes and facilitate the early diagnosis of melanoma in patients with LFS similar to high-risk patients with AMS (20).
The 2 patients reported in this study were monitored with a previously described protocol of total-body photography and digital dermoscopy. This method allows melanomas to be detected as new lesions by total-body photography or as changing lesions with digital dermoscopy, making serial digital dermatoscopic imaging a consideration in high-risk populations (11). Confocal microscopy is a non-invasive technique that may also be useful in the early diagnosis of melanoma, helping to reduce the morbidity of frequent biopsies of benign lesions in high-risk patients (21, 22). In 2 recently published studies, confocal microscopy added to dermoscopy improved diagnostic accuracy and was statistically significant at reducing the number needed to treat, calculated as the proportion of equivocal lesions excised for every melanoma (23, 24). One of the patients in our study had a pigmented lesion that was detected by total-body photography and dermoscopy, evaluated with reflectance confocal micro-scopy, which revealed clear signs in favour of malignancy.
We report here the results of systematic follow-up of 2 patients with LFS in our referral centre, which facilitated the early diagnosis of 3 melanomas. Methods of screening for patients with LFS with atypical moles should include an evaluation for melanoma. This could be completed effectively using digital total-body photography, dermoscopy and even confocal microscopy.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize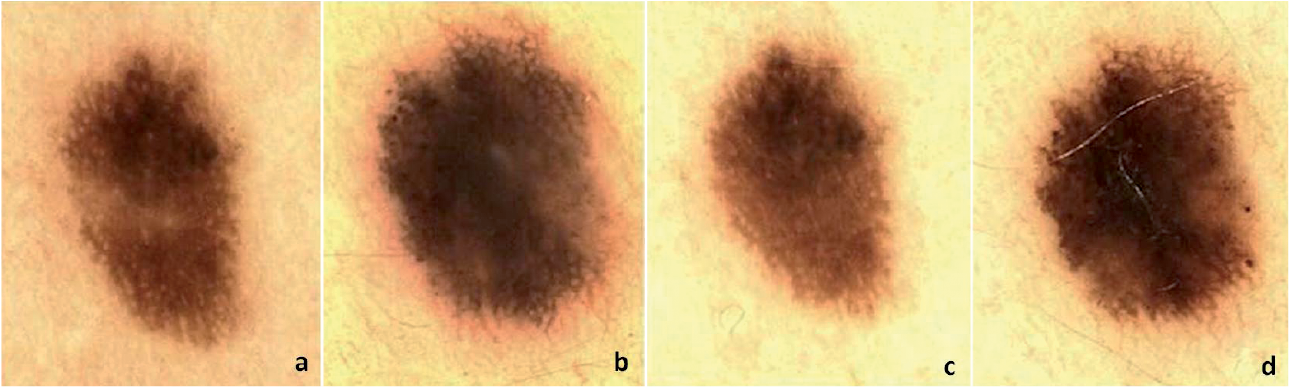 Click to show fullsize
Click to show fullsize