


1Noguchi Dermatology Clinic, 1834-1 Namazu, Kashima-machi, Kamimashiki-gun, Kumamoto 861-3101, 2Ochanomizu Institute for Medical Mycology and Allergology, Tokyo, 3Department of Pathobiology, Nihon University School of Veterinary Medicine, Kanagawa, 4Department of Dermatology, Tokyo Women’s Medical University Medical Center East, Tokyo, 5Division of Bio-resources, Medical Mycology Research Center, Chiba University, Chiba, 6Division of Internal Medicine, Yatsuda Hospital, Kumamoto, and 7Department of Dermatology and Plastic Surgery, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan. E-mail: derma@nogcli.jp
Accepted Mar 15, 2017; Epub ahead of print Mar 15, 2017
The phaeoid fungus Neoscytalidium dimidiatum and a dermatophyte Trichophyton rubrum are the most frequently isolated agents causing fungal melanonychia, followed by the phaeoid fungi of the genera Alternaria and Exophiala (1, 2). Phaeohyphomycosis is an umbrella term describing infections in humans and other animals characterized primarily by the development of dark-coloured hyphae that are caused by phaeoid fungi. The term “phaeohyphomycosis” encompasses broad mycotic infections, regardless of the site of the lesion; the pattern of tissue response, granuloma, or abscess; or the taxonomy of the aetiological agents (3). We describe here a classic example of ungual phaeohyphomycosis.
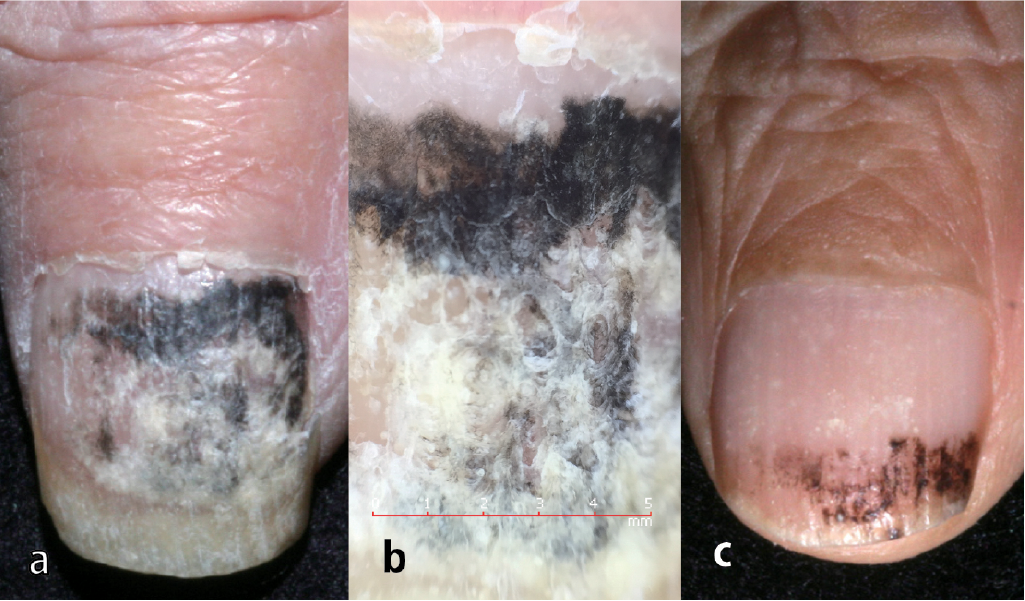
An 82-year-old retired Japanese farmer with chronic heart failure and hemiparesis noticed a black-pigmented area on his right thumbnail that had been present for 6 months. His internist (KS) considered the possibility of malignant melanoma. Upon presentation in February 2016, the nail was thickened and rough with a greyish-white surface, and black pigmentation was observed from its centre to the proximal side. Hutchinson’s sign was not observed (Fig. 1a).
Fig. 1. Clinical characteristics of the thumb nail. (a) Clinical image at presentation. Melanonychia without Hutchinson’s sign. (b) Dermoscopic image showing a black homogenous area and coarse granules proximally. (c) Findings after 4 months of topical application of 10% efinaconazole solution. The opacity ratio decreased from 91% to 32% during that time.
The discoloured area accounted for 91% of the entire nail plate (Image J version 1.48; National Institutes of Health, Bethesda, MD, USA). Dermoscopy (Handyscope connected to an iPhone 6, FotoFinder, Bad Birnbach, Germany) revealed that the distal three-fifths of the nail plate showed a whitish scaly area with random reflection and intermingling irregular black dots, while the proximal one-fifth showed a normal nail plate. Between these 2 areas, a black homogenous area and a partially grey granular area were observed (Fig. 1b).
Direct microscopy revealed branching brown septate hyphae (Fig. 2a), and haematoxylin and eosin and periodic acid-Schiff staining revealed black septate hyphae in the nail plate. The thick cell wall appeared to be double contoured (Fig. 2b). Plate culture on potato dextrose agar after 7 days at 30°C showed a greyish-white woolly colony with coal-black pigmentation on the reverse (Fig. 2c, d). Slide culture showed pigmented broad and unpigmented narrow branching hyphae and intercalary and acropetal chlamydoconidia measuring up to 40 μm (Fig. 2e). The sequence of the internal transcribed spacer 1 region of the ribosomal RNA gene from the nail and isolate had 99% homology to the Botryosphaeria dothidea type strain CBS 115476 (accession: KF766151) (4).
Fig. 2. Mycologic characteristics. (a) Direct microscopic examination revealed branching black hyphae (KOH preparation, original magnification ×400). (b) Septate black hyphae in the nail plate (periodic acid-Schiff staining ×400). (c, d) Plate culture showed a greyish-white woolly colony with a coal-black pigmentation on the reverse. (e) Slide culture showed pigmented broad and unpigmented narrow hyphae and chlamydoconidia. (Lactophenol Cotton Blue staining ×400).
Based on the morphological characteristics and gene analysis results, we diagnosed the patient with ungual phaeohyphomycosis due to B. dothidea (Moug. ex Fr.) Ces. & De Not. The minimum inhibitory concentrations for the isolate were as follows: amphotericin B, 0.25 µg/ml; efinaconazole (EFCZ), 1.0 µg/ml; fluconazole, > 64 µg/ml; 5-fluorocytosine, 2 µg/ml; itraconazole, > 16 µg/ml; micafungin, 0.25 µg/ml; miconazole, 0.25 µg/ml; terbinafine, 0.5 µg/ml; and voriconazole, 0.03 µg/ml. Nail opacity was reduced to 74% and 32% of the nail surface after 1 and 4 months, respectively, of topical application of 10% EFCZ solution (Fig. 1c). The discoloration disappeared with negative conversion of the fungi after 7 months. The patient showed no recurrence of fungal infection during a 3-month follow-up, as of December 2016.
Botryosphaeria dothidea was first described as Sphaeria dothidea Moug. in 1823. The type species of the genus (family Botryosphaeriaceae, order Botryosphaeriales, class Dothideomycetes, phylum Ascomycota) is B. dothidea. Fungi in the order Botryosphaeriales are the most widespread and important plant-pathogens associated with twig, branch, and stem cankers; tip and branch dieback; fruit rot; blue stain; and plant death (5). To date there have been no reports of B. dothidea infection in humans or lower animals, while N. dimidiatum is the most frequent non-dermatophyte and non-Candida pathogen causing onychomycosis in tropical and subtropical regions (6). A survey in Brazil showed that the typical symptom associated with onychomycosis caused by N. dimidiatum was a lateral-distal and lateral-subungual lesion in the big toenail, and melanonychia accounted for 66.6% (20/30) of all cases. It developed in 27.2% (3/11) of Caucasians and 89.4% (17/19) of non-Caucasian individuals (7). The sequence of the internal transcribed spacer 1 region of the ribosomal RNA gene from the isolate and the nail in our case had 95% homology with the N. dimidiatum type strain CBS 499.66 (accession: FM211432) (4). Our case occurred on the Kyushu island of Japan, which is located in the temperate region at 32° north latitude with a mean temperature of 17.2 ± 0.5°C. The annual mean temperature in the Northern hemisphere has increased by 0.85°C during the past 30 years (1983–2012) (8). The incidence of B. dothidea infections might therefore increase gradually even in temperate regions.
Although pigment cells exist in both the nailbed and the nail matrix, melanoma derived from the nailbed has an amelanotic tendency. It is important to differentiate melanonychia arising in the proximal part of the nail from malignant melanoma even if Hutchinson’s sign is not noted (9). The characteristic dermoscopic images of fungal melanonychia are homogeneous pigmented coarse granular lesions with fine black granules of a diameter of 0.1 mm or less (9), which were useful for ruling out a diagnosis of malignant melanoma. The clinical appearances of longitudinal melanonychia were similar to those caused by Phialophora species (10) and were different from those caused by T. rubrum presenting bundle-forming longitudinal lines with a brownish or yellow element (11).
Because onychomycosis caused by N. dimidiatum is refractory and resistant to itraconazole and terbinafine (6), the conventional therapy was expected to be ineffective against B. dothidea infection. In this case, topical application of 10% EFCZ solution was effective. EFCZ is a novel triazole antifungal agent that has good human nail permeability and retention properties (12, 13). Because of its broad spectrum of antifungal activities (14), EFCZ is a promising option in the treatment of non-dermatophyte onychomycosis including ungual phaeohyphomycosis (15).
This research was partially supported by the Research Program on Emerging and Re-emerging Infectious Diseases from the Japan Agency for Medical Research and Development, MAED.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize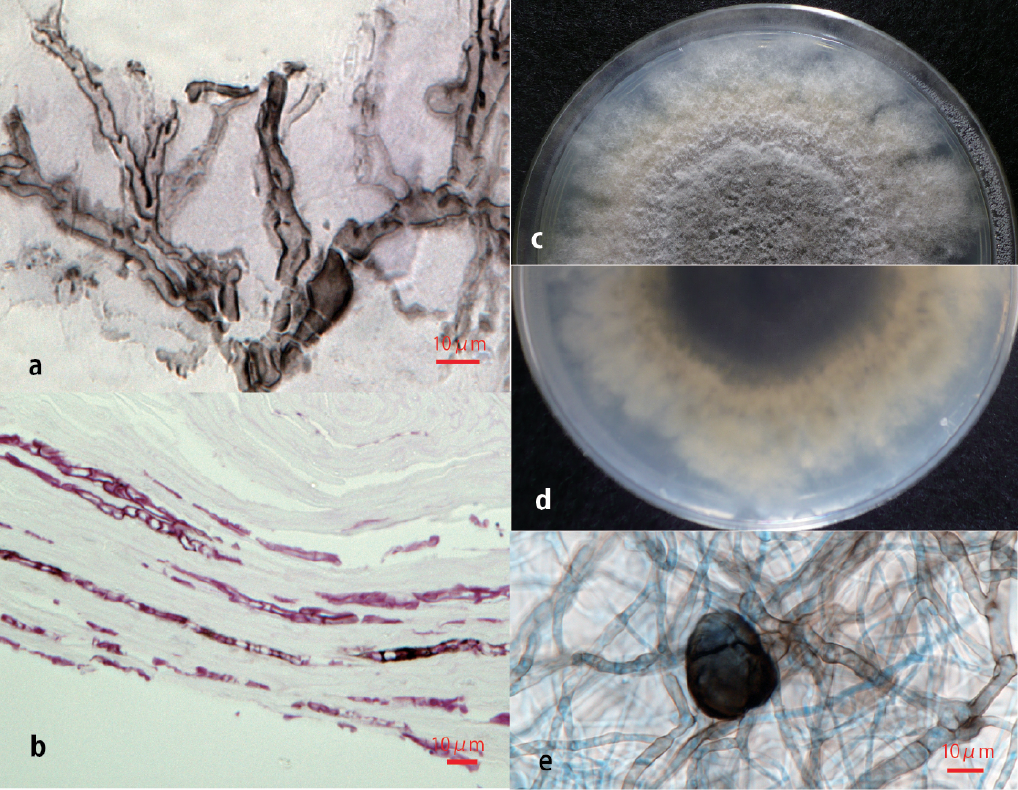 Click to show fullsize
Click to show fullsize