


1Department of Dermatology and 2Department of Immunology, Hospital del Mar-Institut Mar d’Investigacions Mèdiques, Universitat Autònoma de Barcelona (UAB), and 3Department of Statistics, Adknoma Health Research, Barcelona, Spain
#These authors contributed equally to this article.
Although the efficacy of omalizumab has been clearly demonstrated in the treatment of chronic spontaneous urticaria (CSU), its mechanism of action, which results in improvement in CSU symptoms, is not entirely understood. This study investigated the effect of omalizumab on expression of the high-affinity IgE receptor (FcεRI) on blood basophils from patients with active CSU, and its association with the clinical response. Patients exhibiting significant clinical improvement showed a sharp reduction in the levels of basophil FcεRI after 4 weeks, which was maintained throughout the total duration of the treatment. Such evolution was not observed in non-responder patients. Furthermore, non-responders showed significantly lower baseline levels of FcεRI than responders. Baseline basophil FcεRI expression was found to be a potential immunological predictor of response to omalizumab (100% sensitivity and 73.2% specificity). The results of this study contribute to our knowledge of the therapeutic benefit and mechanism of action of anti-IgE therapy in CSU.
Key words: basophils; down-regulation; FcεRI; IgE receptor; omalizumab.
Accepted Mar 16, 2017; Epub ahead of print Mar 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Ana M. Giménez-Arnau, Department of Dermatology, Hospital del Mar-Institut Mar d’Investigacions Mèdiques, Universitat Autònoma de Barcelona (UAB), Passeig Marítim, 25–29, ES-08003 Barcelona, Spain. E-mail: anamariagimenezarnau@gmail.com, 22505aga@comb.cat
Chronic spontaneous urticaria (CSU) represents the most common subtype of chronic urticaria and is defined as the appearance of evanescent wheals, angioedema or both, which occurs suddenly and persists for longer than 6 weeks (1, 2). Although CSU is usually not a life-threatening condition, its symptoms (cutaneous swelling, itch and pain) may have a profound impact on various aspects of patients’ everyday life (2).
Omalizumab is a recombinant humanized monoclonal anti-IgE antibody that specifically binds circulating IgE, preventing its attachment to the high-affinity IgE receptor (FcεRI) of immune cells, such as basophils and mast cells (3–5). It was originally approved for the treat-ment of moderate-to-severe persistent allergic asthma (6, 7), and later in 2014, for the treatment of CSU (6, 8). Several randomized clinical trials have confirmed its efficacy and safety for the treatment of CSU, showing significant reductions in the signs and symptoms of the disease compared with placebo (9–11). It also constitutes the first drug approved for patients with CSU who remain symptomatic despite H1-antihistamine treatment. Nonetheless, approximately 41–48% of patients seen in clinical trials (9–11) and 17–23% in the real-world clinical setting (12–14) do not exhibit a complete or significant response to omalizumab therapy. Given this response rate and the expense associated with its use, the identification of biomarkers predicting responsiveness to this treatment in CSU would prove valuable in routine clinical practice.
Furthermore, the mechanisms by which omalizumab might achieve its therapeutic effects on patients with CSU are not completely understood (4, 15). In allergic rhinitis and asthma it has been shown that omalizumab has the ability to reduce free IgE serum levels and consequently down-regulate FcεRI receptors on basophils, thereby preventing the release of inflammatory mediators that cause allergic signs and symptoms (2, 3, 16–18). However, to our knowledge, this mechanism of action has not been assessed in CSU. Hence, we sought to investigate the effect of omalizumab on basophil expression of FcεRI receptor in a cohort of patients with active CSU, and its possible association with the clinical response. Moreover, we evaluated the basophil FcεRI receptor expression as a potential predictor of response to omalizumab therapy.
Consecutive adult patients controlled at the Urticaria Clinic of the Department of Dermatology of Hospital del Mar (Barcelona) with moderate-to-severe persistent and active CSU (7-days Urticaria Activity Score [UAS7] ≥16 (2)) and refractory to antihistamine therapy were included in the study during the period from January 2014 to December 2015. Following a systematized prospective protocol, treatment with omalizumab 300 mg was administered every 4 weeks. Peripheral blood samples were obtained from these patients prior to the 1st (baseline), 2nd, 3rd, 6th and 12th injections. Exclusion criteria for study participation were: < 18 years of age; concomitant treatment with oral corticosteroids and/or other immunosuppressive agents; and suffer a chronic pruritic disease besides CSU (in order to avoid potential interferences on evaluated clinical scores). In addition, peripheral blood samples from a control group of healthy adult volunteers without family and personal history of allergic asthma, allergic rhinitis, chronic urticaria and atopic dermatitis were also evaluated. The local Clinical Research Ethics Committee granted ethical approval for the study (approval no. 2012/4913/I).
Clinical variables were evaluated using the following patient-reported outcomes (PROs) (2, 19, 20): Urticaria Activity Score (UAS; UAS7 is a composite score of itch severity and hive count over 7 days; range 0–42) and Urticaria Control Test (UCT, a validated tool for assessing disease control in routine clinical practice; range 0–16). Response to therapy was assessed at 6 months of treatment and was defined as an improvement in the patients’ signs and symptoms achieving UAS7 ≤ 6 or ≥ 90% reduction in the UAS7 (1, 21, 22).
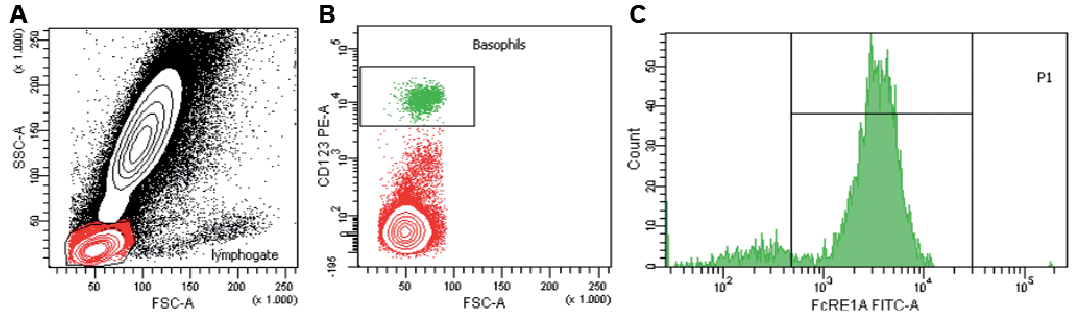
Two independent researchers evaluated the levels of basophil FcεRI receptor and the PROs. FcεRI receptor expression on basophils was measured by flow cytometry from peripheral blood samples obtained from patients with CSU on day 0 and on weeks 4, 8, 20 and 44 of treatment, and from healthy controls (HCs). Flow cytometry analysis was performed following standard procedures. Briefly, 150 μl anticoagulated blood was incubated on the same day of collection during 20 min at 4ºC, with an excess of human immunoglobulins to block unspecific binding. Afterwards, blood was stained with either anti-CD123-PE (BD) or anti-CD193-APC (Miltenyi) to identify basophils and with anti-FcεR1a-FITC (clone CRA1, Ebiosciences) or an isotype control to establish the expression of FcεRI on the surface of blood basophils. After incubation, red blood cells were lysed with a hypotonic solution and samples were analysed by flow cytometry using the FACSDiva software. At least 2 × 105 events were acquired. Gating strategy is represented in Fig. 1. Levels of basophil FcεRI receptor are expressed as mean fluorescence intensity (MFI).
Fig. 1. Gating strategy for detection of FcεRI receptor expression levels on peripheral blood basophils by flow cytometry. (a) Basophils are located within the lymphocyte gate as defined by forward and side scatter parameters. (b) Anti-CD123-PE or alternatively anti-CD193-APC (not shown) allow the identification of basophils among the cells contained in such gate. (c) Anti-FcεRIa-FITC or an isotype control are used to establish the expression levels of FcεRI receptor on CD123+ cells.
All analyses were carried out with SPSS 21.0 statistical package. Descriptive statistics were performed for each variable, using median, percentiles 25th (P25) and 75th (P75) for quantitative variables, and absolute (n) and relative (%) frequencies for categorical variables. χ2 test and Mann-Whitney U test were used to compare the demographic characteristics and the baseline FcεRI receptor expression between patients with CSU and HCs. Pearson’s correlation was used to evaluate the association of the FcεRI receptor expression with serum IgE levels and blood basophil count. Friedman test was used to detect differences over time in the FcεRI receptor expression, UAS7 and UCT during omalizumab therapy. Post-hoc comparisons were performed using Wilcoxon test, and p-values were adjusted using the Bonferroni correction. A mixed linear model was applied to compare the FcεRI receptor expression between responder and non-responder patients (subjects as random effects, weeks of treatment as fixed effects). A receiver-operating characteristic (ROC) curve analysis was used to evaluate the baseline FcεRI receptor expression as a potential predictor of response to omalizumab therapy. A p-value < 0.05 was considered statistically significant.
A total of 91 subjects, 47 patients with active CSU and 44 HCs, were enrolled in this single-centre study. In the control group, the median (P25–P75) age was 45 years (range 33–59) , and 34 out of 44 (77.3%) were women. Demographic and clinical features of CSU group are summarized in Table I. The median (P25–P75) age in this population was 51 years (range 41–64) and there were 37 women (78.7%) and 10 men (21.3%). After 6 months of treatment, 38 out of 47 patients (80.9%) with CSU achieved significant clinical improvement and were classified as “responders” (median value of UAS7 and UCT at 6 months: 0 and 14, respectively), and the remaining 9 (19.1%) as “non-responders” (median value of UAS7 and UCT at 6 months: 23 and 2, respectively). Despite responder patients presented higher total IgE levels at baseline (p = 0.0003) and a lower rate of positive autologous serum skin test (p = 0.022), both groups showed the typical features of “classic” CSU (Table I).
Table I. Characteristics of patients with chronic spontaneous urticaria included in the study
At 12 months of treatment, responder patients showed a satisfactory continued clinical response (median value of UAS7 and UCT at 12 months: 2 and 13, respectively), whereas non-responders did not exhibit significant improvement in CSU symptoms (median value of UAS7 and UCT at 12 months: 26 and 6, respectively).
The median (P25–P75) expression of the basophil FcεRI receptor at baseline was significantly higher in patients with CSU compared with the HC group (11,430 [7,600–16,259] and 4,743 [2,770–7,406] of MFI, respectively) (p < 0.0001) (Fig. 2a). However, the median [P25–P75] expression at baseline in non-responder patients (577 [493–705] of MFI) was significantly lower than in responders (12,227 [10,130–17,899] of MFI; p < 0.0001) and in HCs (p < 0.0001) (Fig. 2b).
Fig. 2. Baseline FcεRI receptor expression (expressed as mean fluorescence intensity; MFI). Comparison (a) between patients with chronic spontaneous urticaria (CSU) and healthy controls (HCs); and (b) between non-responders, responders and HCs. ***p < 0.0001.
The evolution of the basophil FcεRI receptor expression, UAS7 and UCT values during the 12 months of treatment of the 47 patients with CSU is shown in Fig. S1. Overall, a significant sharp drop in the basophil FcεRI receptor expression was observed after the first dose of omalizumab (median [P25–P75] reduction from baseline at 4 weeks: 88.1% [80.9–90.7]; p < 0.0001) (Fig. S1a). This trend was maintained throughout the whole treatment (median reduction from baseline at weeks 8, 20 and 44: 91.0% in all cases). A similar evolution was observed for the values of UAS7 (median reduction from baseline at weeks 4, 8, 20 and 44: 90.6%, 87.4%, 88.2% and 91.4%, respectively) and UCT (median increase from baseline at weeks 4, 8, 20 and 44: 78.6%, 78.5%, 77.5% and 75.0%, respectively) (Fig. S1b). A significant association was found between such a reduction in the FcεRI receptor expression and the clinical improvement observed during the therapy (p < 0.0001).
The kinetic of omalizumab-induced reduction in the FcεRI receptor expression on blood basophils in responder and non-responder patients is shown in Fig. 3a. This kinetic was significantly different between these 2 subgroups, with a lower reduction in non-responders at all time points (median reduction from baseline at weeks 4, 8, 20 and 44: 57.4% vs. 89.2%; 35.3% vs. 91.9%; 35.7% vs. 92.2%; 11.9% vs. 91.8%; respectively) (p < 0.0001). Furthermore, a different evolution was also observed for the values of UAS7 (p < 0.0001) and UCT (p < 0.0001) between responders and non-responders (Fig. 3b–c), which were consistent with the aforementioned evolution of FcεRI receptor levels.
Fig. 3. Kinetic of omalizumab-induced reduction in the FcεRI receptor expression on blood basophils in responder and non-responder patients. (a) Evolution of basophil FcεRI receptor expression, (b) values of 7-day Urticaria Activity Score (UAS7), and (c) values of Urticaria Control Test (UCT) in responder (n = 38) and non-responder patients (n = 9) during omalizumab therapy (levels of FcεRI receptor and UAS7 are expressed as percentage of decrease from baseline, while values of UCT are expressed as percentage of increase from baseline).
The distribution of the baseline FcεRI receptor expression in responder and non-responder patients compared with the median value of the control group (i.e. 4743 of MFI) is shown in Fig. 4.
Fig. 4. Distribution of baseline FcεRI receptor expression in responder and non-responder patients to omalizumab therapy compared with the median value of the control group (MFI: mean fluorescence intensity).
The baseline expression was found to be below this value in the 9 non-responders, and above in the 38 responders. In view of these results, we sought to evaluate the baseline FcεRI receptor expression on basophils as a potential predictor of the response to omalizumab therapy, and the median value of the control group presented 100.0% of sensitivity (i.e. proportion of non-responders correctly identified) and 73.2% of specificity (i.e. proportion of responders correctly identified) to predict the therapeutic response (area under the ROC curve: 0.967; p < 0.001).
Finally, we investigated whether basophil FcεRI receptor expression could be associated with total serum IgE levels and/or blood basophil count, all of them assessed at baseline. A positive correlation was found between IgE levels (median [P25–P75]: 116 [42–277] kU/l) and the FcεRI receptor expression (R=0.573; p < 0.001). Conversely, no association was detected between blood basophil count (median [P25–P75]: 0.032 [0.015–0.065] × 103/µl) and FcεRI receptor expression (R=0.199; p = 0.18).
Omalizumab is a monoclonal antibody that binds selectively to human IgE on its Fc domain (6). By this binding, the interaction between IgE and its high (FcεRI) and low (CD23) affinity receptor is blocked. It has been demonstrated that activation of the FcεRI receptor, which is located on the surface of basophils, mast cells and antigen-presenting cells, plays an essential role in immediate-type hypersensitivity and allergic diseases (16, 17, 23, 24). Furthermore, genetic variability in its α and β subunits has been associated with increased IgE levels and the presence of atopic features (25, 26). Previous data have also demonstrated a positive correlation between FcεRI receptor expression on inflammatory cells and serum IgE levels in a variety of disease states, such as asthma, atopic dermatitis and hyper-IgE syndrome (27). Similarly, this association also appears to be applicable to CSU, as demonstrated by our results. However, considering that CSU is not a classic allergen-driven disease, other factors might also have a significant influence on FcεRI receptor expression. An interesting finding from our study is the difference in the baseline expression of basophil FcεRI receptor between patients with CSU and HCs. Likewise, Metz et al. (28) found higher baseline levels of FcεRI positive cells on cutaneous biopsies from patients with CSU compared with healthy subjects. These results, therefore, would reflect the increased reactivity of inflammatory cells observed in subjects with active CSU, as a higher FcεRI receptor expression would make those cells more sensitive to the stimulation by incoming triggers (5).
In patients with allergic rhinitis and asthma, clinical improvement during treatment with omalizumab has been related to a reduction in free IgE serum levels, and consequently, in the FcεRI receptor expression on the immune effector cells surface, as IgE-free FcεRI is structurally unstable and becomes internalized and degraded (23, 29). This would lead to a reduction in the FcεRI-mediated production of inflammatory cytokines and chemokines (3, 16, 17, 24). Hence, this therapeutic down-regulation represents a unique molecular target whereby both the sensitization and the effector phases of the allergen-specific immune response could be inhibited (29). The fast in vivo onset of action of omalizumab in the treatment of these allergic diseases could also be explained by this mechanism. In this sense, Lin et al. (16) observed a rapidly inhibited ragweed-induced nasal response in patients with allergic rhinitis within the first 7–14 days of treatment, which was associated with a marked reduction (96%) in free IgE serum levels within 3 days and in the basophil FcεRI receptor expression within 14 days (70%). In CSU, however, this mechanism of action has not been extensively evaluated. Previously, Saavedra & Sur (30) reported a female patient with CSU who was treated successfully with omalizumab with a clear reduction (80%) in basophil FcεRI receptor expression after 14 days that was maintained throughout the duration of the treatment. In the present study we confirmed this assumption, and we found that the rapid clinical improvement assessed through the PROs (UAS7 and UCT) was associated with a rapid and sharp reduction in basophil FcεRI receptor expression within the first 4 weeks of therapy. In addition to our study on blood basophils, other investigations have evaluated the kinetic of omalizumab-induced reduction in FcεRI receptor expression on skin mast cells from patients with CSU, and it seems that the time course for such down-regulation is slower on the tissue. Thus, levels of FcεRI positive skin cells in patients with CSU could decline to levels seen in healthy subjects after 12 weeks of treatment (28).
Because CSU represents a complex and multifactorial disease, it seems reasonable to think that a unique pharmacological mechanism could not fully explain the pattern of symptom improvement observed with omalizumab therapy. Some additional mechanisms of action have been proposed, including reversing basopaenia and improving basophil FcεRI receptor sensitivity to allergen-driven secretion (18, 31), alteration of the expression of genes associated with mast cell/leukocyte infiltration, oxidative stress, vascularization and skin repair events2, reducing mast cell releasability (2, 32), or reducing the activity of IgG autoantibodies by lowering the levels of available surface IgE and FcεRI receptor (27), among others. Thereby, given that subsets of patients with CSU may have different disease aetiopathogenesis, the combination of more than one of the aforementioned mechanisms may explain the complete involvement of omalizumab in relieving symptoms associated with CSU (33).
2Unpublished: Metz M, Letzkus M, Hartmann N, Staubach P, Bauer A, Brehler R, et al. Omalizumab normalizes gene expression in lesional skin of patients with chronic spontaneous urticaria: results from a randomized, double-blind, placebo-controlled study. In: 24th European Academy of Dermatology and Venereology Meeting; Copenhagen, Denmark; 2015.
Availability of reliable biomarkers of therapeutic response to different drugs in chronic diseases such as CSU might have an important impact in routine clinical practice. In this sense, for example, cyclosporine-treated CSU patients with a positive serum Basophil Histamine Release Assay (BHRA) showed higher rates of treatment response compared with those patients with negative BHRA (34). More recently, in a retrospective study of 41 patients with CSU the assessment of basophil CD203c-upregulating activity, which is thought to reflect the presence of autoantibodies to IgE and/or FcεRI receptor in the serum of patients with CSU, has been found to be associated with the clinical response to omalizumab (35). However, none of these biomarkers are currently validated for their use in clinical practice.
In the present study we observed that baseline expression of basophil FcεRI receptor may represent a potential predictor of response to treatment with omalizumab in CSU. In fact, all patients who did not achieve clinical improvement with omalizumab had significantly lower baseline levels of basophil FcεRI receptor (and therefore a deficient down-regulation with the treatment) in comparison with responder patients, which would be the most likely explanation for the non-responder status. The reason why these patients show almost undetectable levels of basophil FcεRI receptor is not yet fully understood. Genetic variability in the FcεRI receptor could be a plausible explanation, since recent studies have shown that experimental molecular changes in the subunits of this receptor can affect its expression on the cell surface (36). Other authors have also observed basopaenia in patients with more active CSU disease (37, 38), which reflects the recruitment of basophils to skin tissue and might lead to decreased expression of FcεRI receptor on peripheral blood. However, in our cohort we did not find differences regarding the blood basophil count between responders and non-responders. Therefore, the practical value of basophil FcεRI receptor expression as a clinically useful biomarker of omalizumab therapeutic response should be confirmed in future multicentre prospective studies. This fact would allow physicians to early identify patients who will not benefit from this treatment. In addition, it should be taken into consideration that the results of FcεRI receptor expression assessed by flow cytometry could vary depending on the study population and technical issues. However, using reference data from a control group of healthy subjects would allow more accurate evaluation of the levels of this receptor in patients with CSU.
Although responder patients showed higher baseline total IgE levels in comparison with non-responders, there are not enough arguments to believe in the assessment of total IgE as a good therapeutic predictor in CSU. This is due to the wide range (and therefore overlap) of IgE values observed in responders (16–683 kU/l) and non-responders (1–100 kU/l). Thus, approximately 37% (14/38) of the patients showing satisfactory clinical improvement with omalizumab had baseline total IgE levels within the range observed in non-responders. Furthermore, no predictive value has been found with this biomarker in other allergic diseases (39).
In summary, although further investigations are needed to fully understand the mechanism of efficacy of omalizumab in CSU, our study highlights the importance of the down-regulation of basophil FcεRI receptor expression in this process. Basophil FcεRI receptor expression holds promise as a clinically useful biomarker predicting response to omalizumab therapy. Thereby, low baseline levels would identify a special phenotype of CSU predicting a poor therapeutic response. While additional research should be conducted to further document these observations, the results of this study would have an important impact in the management of CSU and contribute to understanding the clinical utility and mechanism of action of anti-IgE therapy.
The authors would like to thank Miguel Angel Descalzo (Research Unit, Fundación Piel Sana. Academia Española Dermatología y Venereología) for statistical support, and Monica Giménez for helping with English editing and correction of the manuscript.
Conflicts of interest. AMG-A is a medical Advisor for Uriach Pharma, Genentech and Novartis. She has received research grants from Intendis-Bayer, Uriach Pharma and Novartis, and has participated in educational activities sponsored by Uriach Pharma, Novartis, Genentech, Menarini, Glaxo Smith & Kline, Merck MSD, Almirall and Leo Pharma. The other authors declare no conflicts of interests.


 Click to show fullsize
Click to show fullsize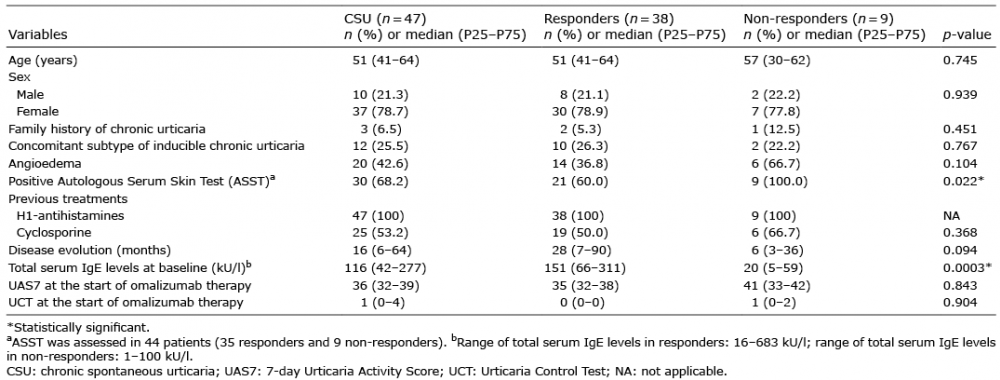 Click to show fullsize
Click to show fullsize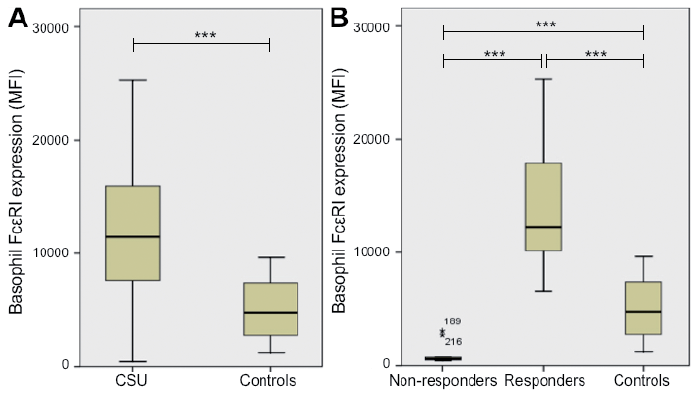 Click to show fullsize
Click to show fullsize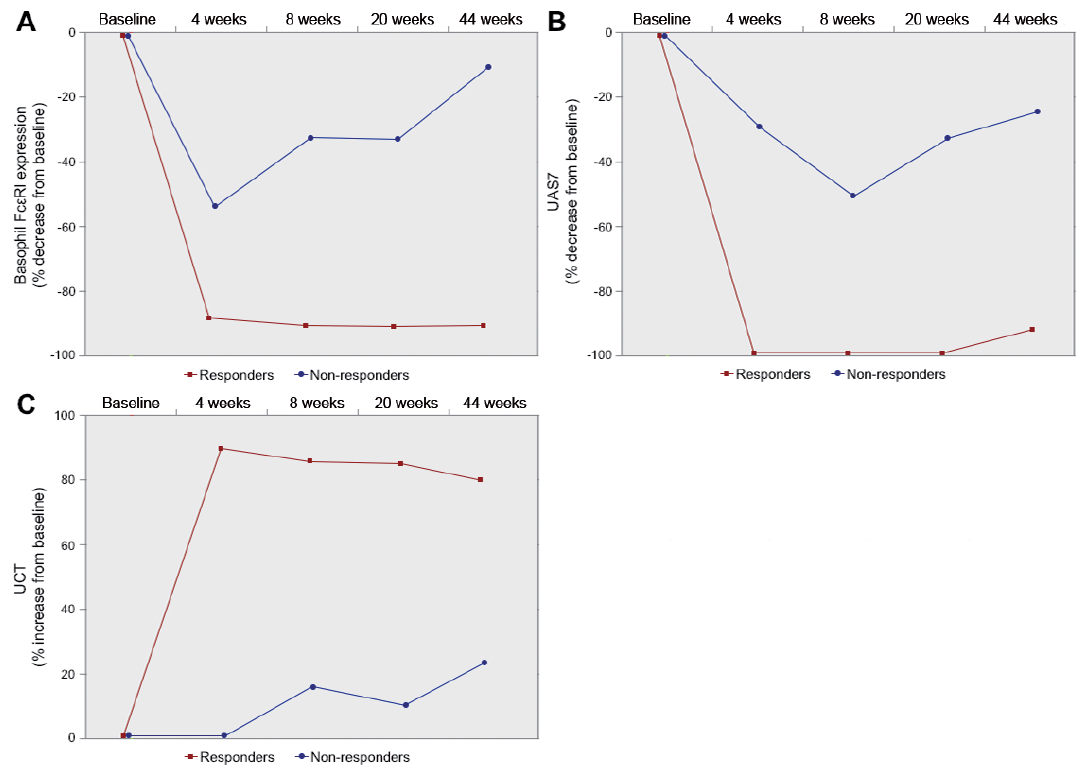 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize