


Department of Dermatology, Yale University School of Medicine, 15 York Street, LMP 5040, New Haven, CT 06510, USA. E-mail: jonathan.leventhal@yale.edu
A 65-year-old man presented to clinic with painful lesions on his left lower extremity for the past 2 months. His medical history included Crohn’s disease treated with prednisone 30 mg daily and ongoing treatment of cholangiocarcinoma with gemcitabine and oxaliplatin. The patient initially noted an ulcerative lesion on the left lower calf and then developed draining abscesses proximally on the thigh over a course of 8 weeks. He reported traumatic injury of the calf, which he believed was secondary to an arthropod bite while outdoors. The patient denied fevers, chills, and other systemic symptoms except for chronic diarrhea from Crohn’s disease.
Physical examination of the left calf revealed an erythematous ulcerative plaque with fibrinous base and hemorrhagic crust (Fig. 1, inset). Distributed on the thigh and proximal calf were tender, suppurative, erythematous subcutaneous nodules and ulcerative plaques in a lym-phangitic pattern (Fig. 1). No other lesions were noted on skin examination.
Fig. 1. The patient gradually developed suppurative, erythematous nodules proximally on the calf and thigh over the course of 2 months. (inset) An ulcerative plaque with fibrinous base and hemorrhagic crust was noted on the left lower calf.
On histopathology, punch biopsy demonstrated necrosis and a dense inflammatory infiltrate in the reticular dermis and panniculus composed primarily of neutrophils (Fig. 2A). Gram stain identified elongated, bacillary, beaded and filamentous Gram-positive bacterial organisms within the suppurative infiltrate (Fig. 2B). Both GMS and PAS stains were negative for fungi, and AFB stain was negative for mycobacterial organisms.
Fig. 2. (A) Punch biopsy revealed necrosis and a dense inflammatory infiltrate composed predominantly of neutrophils in the mid to deep reticular dermis and panniculus (hematoxylin and eosin stain, original magnification x 100). (B) Gram-positive beaded and thin filamentous bacterial rods were identified within the inflammatory infiltrate (tissue Gram stain, original magnification x 600).
What is your diagnosis? See next page for answer.
In our patient, the tissue culture and 16S rRNA gene sequencing analysis identified the organism as Nocardia inohanensis. Nocardia is a gram-positive bacillus with branching filaments, which commonly affects immunosuppressed patients (1). Cutaneous nocardiosis typically occurs in immunocompetent individuals after implantation injury and can be divided into 3 clinical variants: superficial cutaneous, actinomycotic mycetoma, and lymphocutaneous nocardiosis. Disseminated or systemic disease may occur in immunocompromised individuals (1, 2).
Lymphocutaneous nocardiosis is a rare form of Nocardia infection that presents as a primary pyodermatous lesion (purulent ulceration) or abscess with chronic drainage and crusting. Nodular lymphangitis may occur upon invasion of lymphatics, and cellulitis of the soft tissues may occur (1). N. brasiliensis is the most common species associated with lymphocutaneous nocardiosis, accounting for roughly 80% of primary cutaneous or subcutaneous infections (3). N. otitidiscaviarum is another species reported in association with lymphocutaneous disease (4). To the best of our knowledge, this is the first reported case of N. inohanensis manifesting with lymphocutaneous disease.
The differential diagnosis of “sporotrichoid” or lymphocutaneous pattern of lesions includes atypical mycobacterial infection, sporotrichosis, pyogenic bacteria (Staphylococcus, Streptococcus), nocardiosis, leishmaniasis, tularemia, as well as other dimorphic and opportunistic fungal infections. The incubation periods are typically longer for sporotrichosis (1–12 weeks) and leishmaniasis (2–24 weeks), compared to nocardiosis (1–6 weeks), Mycobacterium marinum (2–3 weeks), and tularemia (less than one week). Painful ulcers and suppurative lymphangitic nodules are more common in nocardiosis and tularemia compared to sporotrichosis and leishmaniasis, which typically manifest with painless ulcers (5).
Histopathology demonstrates necrosis and a mixed inflammatory infiltrate with clusters of neutrophils. The organisms are not usually visualized in hematoxylin and eosin-stained sections. In a tissue Gram stain, the organisms are thin, beaded, branched filamentous rods (6). Most Nocardia species are weakly acid fast and modifications of the Ziehl-Neelsen stain may be useful. Certain species of Nocardia causing mycetoma adopt a unique morphology with the formation of sulfur granules. However, while granules are observed in Nocardia mycetoma, they are absent in other forms of cutaneous nocardiosis. Definitive diagnosis involves isolation and identification of the organism from tissue culture. Visualization of weakly acid fast, filamentous, branching rods can provide a presumptive diagnosis; however, PCR is required for accurate identification of the organism. The 16S rRNA gene sequencing technique is a commonly utilized method for identification of the species (3).
Sulfonamides are the treatment of choice for nocardiosis. Although sulfadiazine and sulfisoxazole have historically been employed, trimethoprim-sulfamethoxazole (TMP-SMX) is most frequently used. There have been only rare reports of clinical treatment failure and in vitro studies have demonstrated little resistance to TMP-SMX. A study of 552 Nocardia isolates from 6 U.S. medical centers found only 2% had resistant minimum inhibitory concentrations for TMP-SMX (7). For patients allergic or intolerant to sulfonamides, minocycline provides an effective alternative. Other antimicrobial agents that may be used include imipenem, moxifloxacin, tigecycline, linezolid, amikacin, and cefotaxime (8). Combined antimicrobial therapy may improve efficacy (9). Recommended duration of treatment is 3–6 months for cutaneous infection in immunocompetent individuals and 6–12 months or longer in patients with immunocompromised status or central nervous system disease. Deep abscesses may require surgical drainage.


 Click to show fullsize
Click to show fullsize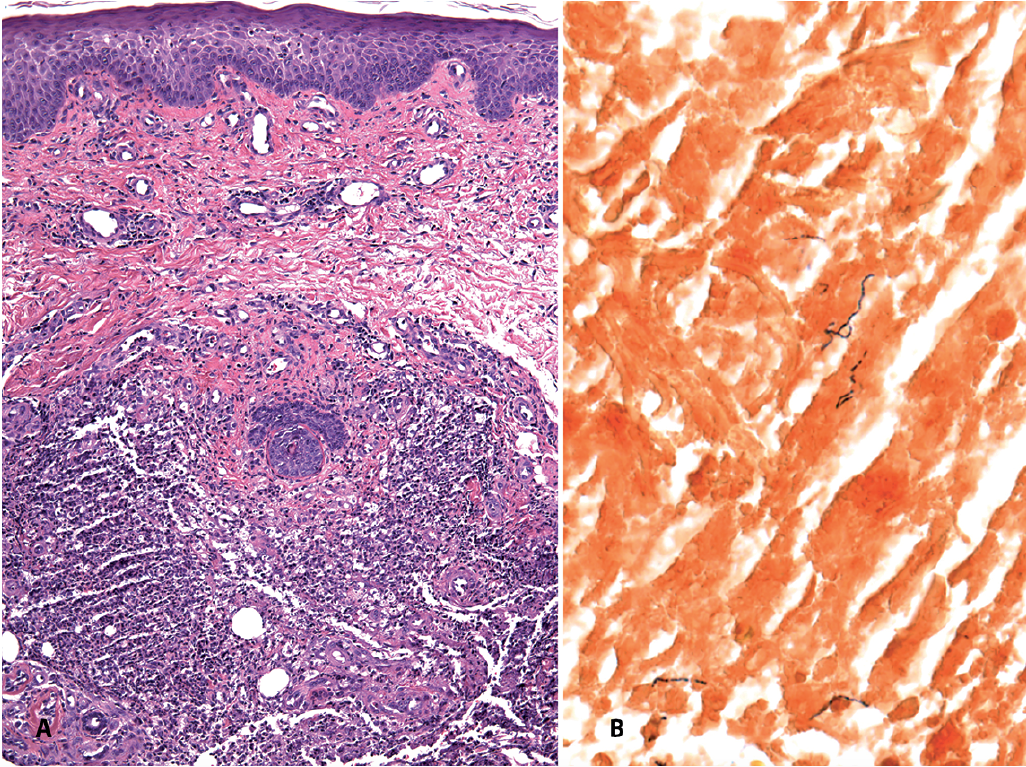 Click to show fullsize
Click to show fullsize