


1Department of Medicine, Dermatology and Venereology Unit, Karolinska University Hospital, and 2Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden
Basal cell carcinoma (BCC) is the most common form of cancer worldwide. Exposure of the skin to ultraviolet (UV) radiation, from sunlight and other sources, is the most important risk factor. The aim of this large-scale case-control study was to determine which occupations are associated with increased risk of BCC in Sweden. The case cohort comprised 74,247 patients with BCC and the control cohort comprised 574,055 subjects linked to population-based registers. Compared with the occupational category of farmers, foresters and gardeners we observed elevated risks of BCC for almost all occupational categories studied. Legal workers with odds ratio (OR) 2.69 (95% confidence interval (CI) 2.36–3.06), dentists OR 2.69 (95% CI 2.35–3.08) and physicians OR 2.47 (95% CI 2.24–2.74) had the highest risk for both sexes taken together. In conclusion, there appears to have been a change in the risk of BCC from outdoor to indoor occupations in Sweden, possibly related to exposure to UV radiation during leisure activities exceeding occupational sun exposure as the main cause of BCC in Sweden.
Key words: epidemiology; occupation; basal cell carcinoma.
Accepted Mar 27, 2017; Epub ahead of print Mar 30, 2017
Acta Derm Venereol 2017; 97: XX–XX
Corr: Bernt Lindelöf, Department of Medicine, Unit of Dermatology and Venereology, Karolinska Institutet, Karolinska University Hospital, SE-171 76 Stockholm, Sweden. E-mail: bernt.lindelof@karolinska.se
Basal cell carcinoma (BCC) of the skin is the most common type of cancer worldwide (1). Although BCC is a malignant tumour, it very rarely metastasizes and mortality is low. However, because of the number of cases, this places a huge burden on healthcare resources (2). Exposure to ultraviolet (UV) radiation from sunlight remains the most important environmental risk factor (3).
There are only a limited number of epidemiological studies of occupational cases of BCC (4–8). This may be due to the fact that BCC cases, in spite of the high incidence, are rarely included in central cancer registries. Occupational skin cancer may also be under-reported (9).
A systematic review of the literature regarding occupational exposure to UV and occurrence of BCC concluded that outdoor workers were at significantly increased risk for BCC (10). Farmers are considered to be a group at high risk for BCC (11), but studies related to farm workers, sun safety behaviour, and skin cancer are scarce (12).
However, in recent times, the role of sun exposure in different occupations might have become of less relative importance than leisure time in the sun, taking into account the changing sun behaviour patterns of the general public along with the increasing travel to sunny resorts and use of artificial tanning sunbeds. Furthermore there are a number of other risk factors than sun exposure, e.g. ionizing radiation or chemical agents that might be relevant in certain occupations (13).
Interestingly, in a large population-based study of occupation and cancer in the Nordic countries, fishermen and forestry workers were ranked as the groups with the lowest risk of malignant melanoma and non-melanoma skin cancer in men (BCC was not included) (14). The aim of the present study was to evaluate the role of occupation in BCC. A large number of BCC patients and control patients from an earlier study were included (15). The study used data from the public, population-based, and non-insurance-based Swedish healthcare system and population-based mandatory national cancer register. Subjects’ unique personal identification numbers allowed register linkage. The patients’ and controls’ demogra-phics, socioeconomic status and place of residence were adjusted in order to obtain reliable data.
The study was approved by the Regional Ethics Review Board, Stockholm (2009/55).
During the years 2004 to 2008 a total of 115,016 cases of BCC were reported to the Swedish Cancer Registry. For this study a case of cancer was considered to be a BCC for all topography codes between T01000 and T02830 with a histopathology code between M80903 and M80953 (variants of BCC).
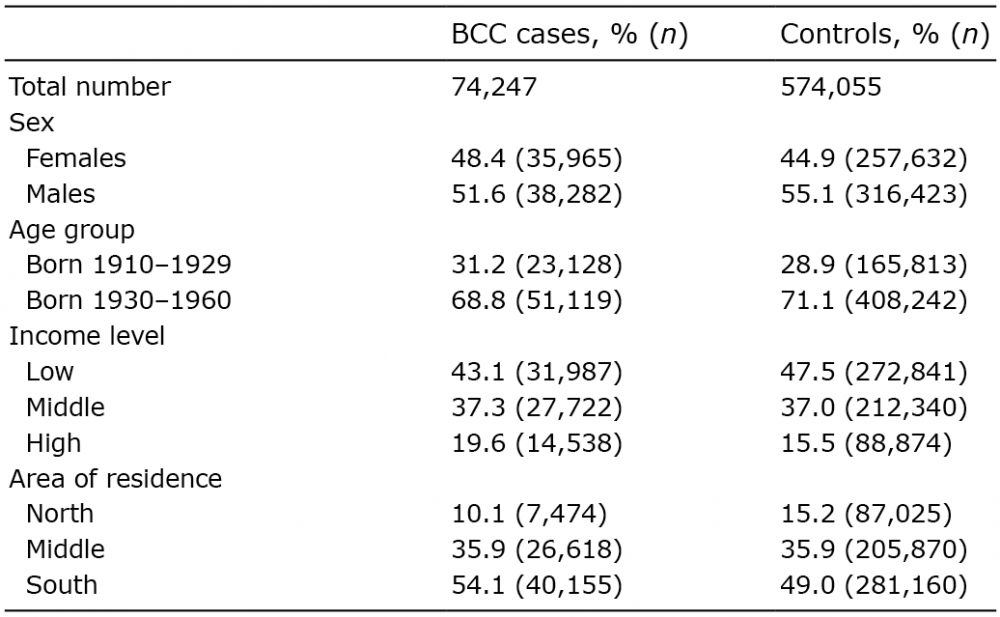
In the 17% of the patients who had 2 or more BCC reported to the registry, the first verified BCC was included in the study. Incidence density sampling was applied to find 10 controls with the same age and sex with which to match the cases. The controls were identified from the Register of Total Population (2004–2008). Incidence density sampling makes it possible for a case to be selected as a control before its own cancer is diagnosed. They were further required to be alive and free of BCC at the time of BCC diagnosis of the case. For each case and control, information was received from the databases of persons participating in computerized population censuses at Statistics Sweden. Furthermore, only persons born in Sweden were included and those with missing information according to occupation, income and place of residence were omitted. All persons with an earlier skin cancer (not BCC) were also excluded. Finally, occupation information was available only for persons born during the period 1910–1960. After these adjustments the case cohort comprised 74,247 subjects and the control cohort 574,055 subjects (Table I).
Table I. Distribution of characteristics among basal cell carcinoma (BCC) cases and controls
All Swedish inhabitants have a unique 12-digit identification number, enabling identification of patients in national registries.
The National Swedish Cancer Registry managed by the Swedish Board of Health and Welfare has registered BCC since 2004 (16). According to regulations all pathology and cytology departments in Sweden must report all cases of BCC to the registry. Thus, all diagnoses of BCC in the registry file are based on histopathological examination. The reporting is performed automatically via the histopathology code. No figures on the completeness of registration of BCC have been presented up to now.
Statistics Sweden run a large number of registers covering the whole Swedish population, i.e. historical population register, occupational register, educational and income register. All BCC cases and controls were linked to these registers in order to get information about their country of birth and socioeconomic data. The register linkages were made at Statistics Sweden and the Swedish Board of Health and Welfare and before the database was sent for analysis the personal identification numbers were deleted.
Level of income. Disposable income for each case and control for the year of BCC diagnosis was stratified at 3 different levels: low < 200,000, middle 200,000–360,000, and high > 360,000 Swedish crowns (SEK) (current exchange rate: 1 Euro = 10.1 SEK).
Occupations. The main occupation status at 31–50 years of age was determined for the study population. The ISCO 88 (International Standard Classification of Occupation) codes on a 2-digit level were mainly employed, giving 54 specific occupations based on 6 national censuses 1960–1990.
Geographical regions. The country of Sweden (latitude 69–55°) was divided into 3 geographical regions, and cases and controls were referred to northern, middle or southern part of Sweden according to their home addresses for the year of BCC diagnosis.
Conditional logistic regression was conducted to calculate crude and adjusted odds ratios (OR) with 95% confidence intervals (95% CI) as estimates of relative risk of BCC in relation to different occupations. These were adjusted for geographical region, income level and education level for a subset (not shown in Table I). The results are shown for all and by sex. Analyses were conducted using SPSS, version 20 (IBM, Armonk, NY, USA).
The characteristics of the cases and the matched control subjects are shown in Table I. The BCC cases had slightly higher income than controls and lived more often in the south of Sweden.
In Table II OR and 95% CI (adjusted for age, level of income and place of residence) are provided by occupation category for all and separately for women and men. In comparison with the occupational category of farmers, foresters and gardeners we observed elevated risks for BCC for all occupational categories shown.
Table II. Odds ratios (OR) for basal cell carcinoma by occupation and sex
Legal workers, dentists and physicians had the highest risk for both sexes taken together, ORs between 2.69 and 2.47. The highest risk for females was found in dentists: OR 2.50 and for males in legal workers: OR 2.83. Seventeen occupations with OR <1.40 or non-significant (NS) are not shown in Table II. (NS: fishermen, hunters; forestry workers; miners, quarry workers; boat crew; other transport work; smelting workers OR<1.40: employees at farms, gardens; transport workers, rail and road; mechanics; wood-workers; other construction workers; glass, brick-makers, etc; chemical process workers; other manufacturers; unskilled workers; engine operators; cleaners, building caretakers).
This study found the occupational risk of BCC to be more than 2.5-fold for the indoor occupational category, such as legal workers, dentists and physicians, compared with the outdoor occupational category of farmers, foresters and gardeners, which was used as a reference. Legal workers, dentists and physicians in most countries have 3 things in common; a very long education, high salaries and they perform most of their work indoors. In fact most of the occupational categories investigated had significantly higher risk of BCC than the reference. This finding is in contrast with other epidemiological studies. Bauer et al. (10) performed a systematic review of the literature and included 23 studies in a meta-analysis. The conclusion was that outdoor workers are at significantly increased risk for BCC. In a recent study of farmers in Poland the authors highlight the increased incidence and risk of recurrence of BCC in farmers (11).
However, in a large epidemiological study of occupation and cancer in the Nordic countries comprising 15 million people, outdoor occupations such as fishermen and forestry workers had the lowest risk for melanoma and non-melanoma skin cancer in men (BCC was not included). In contrast, the highest risks were found in occupations of relatively high socio-economic status, such as dentists and physicians (14). The findings in our study support that this is also valid for BCC.
There appears to have been a shift in the risk of BCC in Sweden from outdoor to indoor occupations, which is probably related to UV exposure during leisure-time and not to the occupation. Legal workers, dentist and physicians with high risk of BCC are not sun-exposed during work, but might be sun-burned during their leisure-time, in contrast to farmers, foresters and gardeners with low risk and more consistent and repetitive sun exposure during outdoor work on a regular or daily basis. An illustration of the importance of leisure-time sun exposure could be the increased incidence of skin cancer reported among airline cabin crew. Cabin crew are not exposed to UV radiation, but they may spend more time in sunny resorts due to their work than the general population. In a recent Finnish study of female cabin crew-members and controls from the general population, the cabin crew reported more sunbed use and slightly more intermittent UV exposure than the reference population. Also, exposure to cosmic radiation did not explain the excess of skin cancer among the cabin crew studied (17). This is in line with the findings of this study, in which flight workers had among the highest risk of BCC.
Since UV exposure related to BCC takes place over a long period of time, differentiation between occupational exposure and recreational exposure is problematic. Only if the cumulative occupational UV exposure exceeds the cumulative exposure during leisure-time can the BCC be considered occupational. Also, for the same occupation there could be individually variations in sun exposure during work, depending on, for example, natural shading, habits and indoor breaks (18, 19). The findings in this study of high risks among occupations of relatively high socio-economic status with low sun exposure during work highlight the importance of leisure-time exposure and sun-burns. Other factors that at least partly affect the risk might be the temperature and weather conditions in Sweden, causing outdoor workers to cover the skin with clothing, and that the proportion of the population working in outdoor occupations, such as agriculture, has decreased dramatically since 1960. However, we cannot rule out that the excess risk in some of the occupational categories is due to non-UV factors (8), e.g. healthcare personnel might, at least partly, be affected by products they handle in their work or exposition to ionizing radiation (7).
The current study has the advantage of using individual data on cancer and socioeconomic factors from population-based registries covering the whole Swedish population. Whilst we consider the internal validity of the current study to be high, some limitations should be emphasized. The Swedish Cancer Registry started to register BCC in 2004, in contrast to the registration of all other forms of cancer, which started in 1958. Thus we have no control over the patients’ and control subjects’ history of BCC before 2004. A limited number of control subjects were, in fact, cases and some of the cases had already had a BCC before the entry in the study. This caused some overlapping of cases and controls and tends to underestimate the differences between cases and controls found in this study. However, it does not interfere with the ranking of the occupational risks presented in this study.
Also, we have no figures on completeness of the BCC register, but the reporting is performed automatically via the histopathology code. Furthermore, the higher risk for medical personnel; physicians, dentist and nurses might indicate that there is some degree of surveillance bias and more educated individuals might also be more likely to seek healthcare.
In conclusion, we observed a number of occupations involving excess BCC risk. Occupations with relatively high socio-economic status dominated. UV exposure during leisure-time might be the explanation.


 Click to show fullsize
Click to show fullsize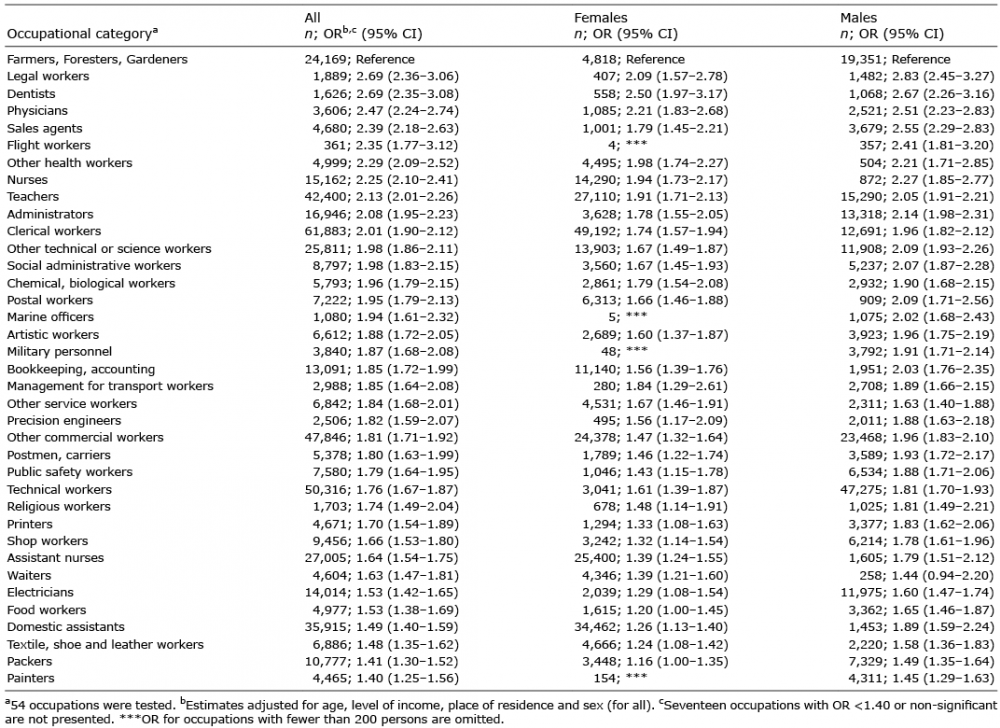 Click to show fullsize
Click to show fullsize