


1Department of Medicine, Section of Dermatology and Venereology, University of Verona, Verona, 2Department of Laboratory Medicine, Hospital-University of Padua, and 3Department of Medicine, Section of Endocrinology, University of Padua, Padua, Italy
Psoriasis is frequently associated with metabolic comorbidities. Advanced glycation end products (AGEs) are highly oxidant, biologically active compounds that accumulate in tissues in association with hyperglycaemia, hyperlipidaemia and oxidative stress. This is a cross-sectional case-control study involving 80 patients with mild/severe psoriasis and 80 controls matched for age, sex and body mass index (40 with severe eczema, 40 healthy individuals). Patients and healthy individuals with a smoking habit, diabetes, dyslipidaemia, hypercholesterolaemia, hypertension or who were under systemic treatment were excluded from the study. Skin AGEs were measured in normal-appearing skin by a standard fluorescence technique, and blood AGEs (total AGEs, pentosidine and AGEs receptor) by enzyme-linked immunosorbent assay. Levels of cutaneous AGEs (p < 0.04), serum AGEs (p < 0.03) and pentosidine (p < 0.05) were higher in patients with severe psoriasis. Cutaneous AGEs correlated well with serum AGEs (r = 0.93, p < 0.0001) and with Psoriasis Area and Severity Index score (r = 0.91, p < 0.0001). Receptor levels were lower (p < 0.001) in severe psoriasis, and inversely correlated with disease severity (r = –0.71, p < 0.0002). Patients with severe psoriasis have accumulation of skin and serum AGEs, independent of associated metabolic disorders.
Key words: psoriasis; eczema; advanced-glycation-end-products; inflammation.
Accepted Mar 27, 2017; Epub ahead of print Mar 30, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Anastasia Papagrigoraki, Department of Medicine, Section of Dermatology and Venereology, University of Verona, Piazzale A. Stefani 1, IT-37126 Verona, Italy. E-mail: papanastassia@yahoo.it
Psoriasis is a common chronic inflammatory immune-mediated disease that affects 2–3% of the Western population. Ten to 20% of patients with psoriasis have severe disease, defined by an involved body surface area greater than 10% (1, 2). Severe psoriasis is strongly associated with metabolic disorders, including obesity, metabolic syndrome, arterial hypertension, dyslipidaemia and type II diabetes (3–9). Advanced glycation end products (AGEs) are a group of highly oxidant, biologically active compounds that accumulate in tissues, mostly in association with hyperglycaemia, hyperlipidaemia and oxidative stress. AGEs form through several pathways, including oxidation of sugars, lipids and amino acids, to create reactive aldehydes that bind covalently to proteins. A well-characterized and easily detected member of this large class of compounds is pentosidine (10–12). AGEs are part of the normal metabolism, but, if expressed in excess, may alter cellular structure and function, and promote oxidative stress with formation and release of free radicals (13–15). Accumulation of AGEs occurs permanently in physiological terms through ageing, and it is markedly amplified in diabetes as a consequence of persistent hyperglycaemia, but is also documented in patients with obesity, metabolic syndrome, rheumatoid arthritis, and fatty liver disease (16–18). AGEs elicit biological function through activating membrane receptor (RAGE; receptor for advanced glycation end-products), which is expressed on the surface of inflammatory and epithelial cells, and promotes innate immunity. RAGE exists as several variants, and has emerged as a central regulator for vascular inflammation and atherosclerosis (19–21).
The primary objective of this study was to investigate whether psoriasis is associated with accumulation of AGEs in the skin and serum, and whether skin and serum AGEs correlate with psoriasis severity.
This cross-sectional case-control study involved a series of 80 patients with chronic plaque psoriasis (cases) and 80 controls matched for age, sex and body mass index (BMI). Inclusion criteria for cases were adult age between 18 and 60 years, clinical diagnosis of chronic plaque psoriasis, and lack of any systemic treatment for psoriasis for at least 6 months before enrolment. Patients affected by psoriatic arthritis were not included. The control group included healthy subjects and patients with chronic eczema, mostly atopic dermatitis. Psoriasis or eczema mean duration was ≤ 3 years at enrolment. Disease duration and patients’ age were selected in order to avoid bias associated with age-related changes in levels of AGEs. Patients and healthy individuals with smoking habit, diabetes, dyslipidaemia, hypercholesterolaemia, hypertension, any systemic inflammatory, metabolic or autoimmune disease or under systemic treatment, including corticosteroids, acitretin, cyclosporine, methotrexate, phototherapy or biologics, were also excluded from the study. All subjects, after being informed of the study purpose and procedures involved, signed informed consent and were visited by a dermatologist who registered demographic, biometric and other relevant data on a digital case report form. Relevant data collected included age, sex, weight, height, BMI, waist circumference, blood pressure, age of onset of the cutaneous disease, and concomitant medications. Severity of psoriasis was assessed according to the Psoriasis Area and Severity Index (PASI), body surface area (BSA), and static Physician’s Global Assessment (PGA) (22). Eczema severity was determined using the Scoring Atopic Dermatitis scale (SCORAD) and the PGA score (23). Cases were divided into patients (n = 40) with severe psoriasis (PASI ≥ 12; BSA ≥ 20; PGA ≥ 3) and patients (n = 40) with mild psoriasis (PASI ≤ 7; BSA ≤ 10; PGA ≤ 2). Psoriasis patients who fell between the including range (PASI 7.1–11.9; BSA 10.1–19.9) were intentionally excluded from the study. Controls included 40 subjects affected by chronic severe eczema (SCORAD ≥ 60; BSA ≥ 20; PGA ≥ 3) and 40 healthy individuals recruited from the hospital staff (physicians, nurses, secretaries and cleaning personnel) who met all the inclusion criteria requested. During the visit, cases and controls underwent a first evaluation of the total accumulation of cutaneous AGEs, and then in all subjects a venous blood sample was collected after overnight fasting. The study protocol was reviewed and approved by the local bioethics committee and was conducted in accordance with Good Clinical Practice Guidelines for physicians involving medical devices, sample storage and transportation. Strict adherence to the Declaration of Helsinki was followed at all times.
Total cutaneous content of AGEs was evaluated by the AGE Reader mu® Diagnoptics Technologies B.V., Groningen, the Netherlands), which measures tissue AGEs by means of fluorescence technique (24). This is a non-invasive method using a light source (polarized), which illuminates the skin of the medial right forearm; the polarized light excites fluorescent moieties in the tissue, which emit light of a different wavelength. The major contribution in fluorescence comes from fluorescent AGEs linked mostly to collagen, but also to other proteins and lipids. The light emitted is detected using a spectrometer, which is successively translated to arbitrary unit (a.u.). Skin AGEs levels vary in the different body areas, presenting higher levels on the left forearm and lower levels on the right calf. Normal values are age-related, and patients of mean age 45 years have an interval range of the medial right forearm between 1.7 and 2.1 a.u. Cutaneous AGEs were measured in normal appearing skin by taking 3 readings per subject that showed no variability. Lesional skin was also tested in patients with psoriasis or eczema presenting with lesions localized on the right forearm, and showed no different values from normal-appearing skin on the same patient.
Venous samples collected rested for 30 min and were centrifuged successively at 4°C for 5 min. Sera and plasma samples obtained were stored deep-frozen at –80°C until tests were performed. Serum total AGEs (CUSABIO, Wuhan, China; catalogue number CSB-E09412h) and serum pentosidine (CUSABIO; catalogue number CSB-E09412h) were measured using enzyme-linked immunoassay (ELISA) kit according to the manufacturer’s protocol: intra-assay precision CV% < 8%; inter-assay precision CV% < 10% for both analytes. Limit of detection (LOD), defined as concentration of analyte giving absorbance higher than mean absorbance of blank plus 3 standard deviations (SD) of the absorbance of blank, was 0.195 μg/ml for AGEs and 7.81 pmol/ml for human pentosidine.
The soluble RAGE (total sRAGE), comprising both the extracellular domain of wild-type full-length RAGE, which results from proteolytic cleavage at the cell surface and the endogenous secreted isoform lacking transmembrane domain (esRAGE) were measured using an ELISA kit (RayBiotech, Norcross, GA; catalogue number ELH-RAGE) according to protocol with an intra-assay precision test <10%, inter-assay precision < 12% and LOD < 3 pg/ml.
The results are presented using basic parameters of descriptive statistics, such as mean value, SD and standard error (SE). Normal distribution of data was measured using Shapiro-Wilk. The Student’s t-test for paired variables was used to compare dependent data. Independent data among groups were compared using non-parametric Mann–Whitney tests. A p < 0.05 was considered statistically significant. Calculations were performed with the software Analyse.it version 2.07 for Windows.
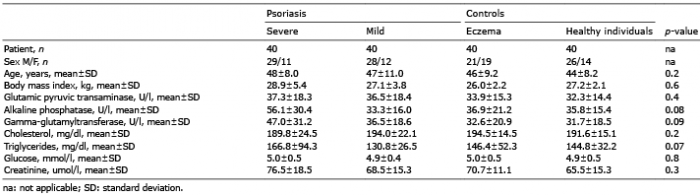
The characteristics of the study population are reported in Table I. Cases included 40 patients affected by severe psoriasis with median PASI 16.2 (95% confidence interval (95% CI) 15.8–17.2), median BSA 22.2 (95% CI 21.6–24.4), and static PGA mean value 3 (95% CI 3.0–3.2) and 40 patients with mild psoriasis presenting a median PASI 4.5 (95% CI 3.9–5.1) median BSA 8.0 (95% CI 7.3–9.1) and static PGA mean value 2 (95% CI 1.2–2). The control group included 40 patients with severe chronic eczema with median SCORAD 64.8 (95% CI 62.1–69.4), median BSA 34.1 (95% CI 29.6–36.2), static PGA mean value 4 (95% CI 3.2–4) and 40 healthy individuals with no cutaneous involvement of any chronic inflammatory and/or autoimmune and/or metabolic disease. There were no differences in age, sex, BMI, plasma cholesterol, triglycerides, creatinine, liver enzymes and glucose levels between cases and controls.
Table I. Characteristics of the study population
Levels of skin AGEs were significantly higher in patients with severe psoriasis compared with patients with mild psoriasis (2.87 vs. 2.15, p = 0.04), patients with severe eczema (2.87 vs. 1.90, p = 0.02) and healthy controls (2.87 vs. 1.86, p = 0.01) (Fig. 1a). There were no differences in levels of AGEs between normal appearing skin and lesioned skin in psoriasis and eczema patients presenting with lesions localized on the right forearm (data not shown). Serum levels of AGEs paralleled the cutaneous findings in patients with sever psoriasis, severe eczema and healthy individuals (Table II). In detail, AGEs in patients with severe psoriasis were significantly higher compared with patients with mild psoriasis, patients with severe eczema and healthy subjects. Cutaneous levels of AGEs correlated positively with the serum AGEs (r = 0.93; p < 0.0001) (Fig. 1b), and serum levels of AGEs correlated well with disease severity (r = 0.91; p < 0.0001) (Fig. 1c). Serum levels of pentosidine were also significantly higher in patients with severe psoriasis compared with patients with mild psoriasis (p < 0.05), patients with severe eczema (p < 0.0001) and healthy subjects (p < 0.0001) (Fig. 2a). Pentosidine correlated well with cutaneous AGEs (r = 0.78; p < 0.0002) (Fig. 2b), and with PASI score (r = 0.91; p < 0.0001) (data not shown). In contrast, serum levels of RAGE were significantly lower in patients with psoriasis compared with those with eczema or healthy individuals (p = 0.001), and there were no differences between patients with mild and severe psoriasis (Fig. 3a). However, RAGE levels correlated inversely with disease severity evaluated with the PASI score (r = –0.71; p < 0.0002) (Fig. 3b).
Fig. 1. Skin and serum levels of advanced glycation end product (AGE) in relation to one another and to psoriasis severity. (a) Skin levels of AGEs are higher in patients with severe psoriasis (*) compared with patients with mild psoriasis (p = 0.04), with patients with severe eczema (p = 0.02) and with healthy individuals (p = 0.01). (b) Cutaneous levels of AGEs correlated positively with serum AGEs (r = 0.93; p < 0.0001) in all subjects, and (c) serum levels of AGEs correlated well with the Psoriasis Area and Severity Index (PASI) score (r = 0.91; p < 0.0001) in patients with psoriasis.
Table II. Serum levels of advanced glycation end products (AGEs) are increased in patients with severe psoriasis compared with controls
Fig. 2. Pentosidine levels in relation to clinical severities and skin levels of advanced glycation end products (AGE) (a) Serum levels of pentosidine were significantly higher in patients with severe psoriasis compared with patients with mild psoriasis (*p < 0.05), with patients with severe eczema (**p < 0.0001) and with healthy controls (p < 0.0001). (b) Serum pentosidine correlated well with measurements of cutaneous AGEs (r = 0.78; p < 0.0002) in all subjects.
Fig. 3. Soluble receptor for advanced glycation end-products (RAGE) in relation to clinical severity. (a) Serum levels of RAGE were significantly lower in patients with psoriasis compared with controls (*p = 0.001). (b) Serum levels of RAGE correlated inversely with disease severity (r = –0.71; p < 0.0002) in patients with psoriasis.
AGEs are a group of irreversible cross-linked ketone adducts created via a non-enzymatic glycation between reducing sugars and free amino groups of proteins, lipids or nucleic acids. AGEs form endogenously during normal metabolism and exogenously from foods prepared at high temperatures, as well as from tobacco smoking (10, 15, 18). Our study, which included only patients selected for not having conditions or diseases known to be associated with accumulation of AGEs, shows that those affected by severe plaque psoriasis have increased concentration of cutaneous AGEs, serum AGEs, and pentosidine. Cutaneous AGEs correlated directly with serum AGEs and with psoriasis severity. In contrast, levels of total soluble RAGE were lower in the serum of patients with psoriasis compared with controls and correlated inversely with psoriasis severity. These results are consistent with previous studies showing a similar trend in patients with other inflammatory diseases, including rheumatoid arthritis, Still’s disease, diabetes and atherosclerosis (15–21, 25).
An unexpected finding was the low levels of serum AGEs in patients with mild psoriasis. Speculatively this could be attributed to a different diet. The mean pre-meal total serum levels of AGEs in healthy individuals is highly variable, ranging from 3.59 to 13.53 × 103 μg/ml (18, 26). Dietary AGEs (d-AGEs) derive from the Maillard’s reaction and are increased by 10–100 times in food cooked with dry heat procedures, such as grilled and fried food, compared with subjects consuming food cooked with moist heat (boiled and steamed) (26, 27). Patients with psoriasis may avoid fried food, as they may consider it might worsen psoriasis (28). AGEs accumulate slowly in human tissues during ageing, and more rapidly in association with persistent hyperglycaemia and enhanced oxidative or carbonyl stress and ultraviolet (UV) irradiation. The discrepancy between skin and serum AGEs in patients with mild psoriasis might be attributed mostly to the higher sun exposure in this group of patients, as UV radiation promotes accumulation of AGEs in the skin (29). Additionally, in patients with psoriasis, in contrast to the large difference in serum AGEs levels between mild and severe psoriasis patients, only a small difference in pentosidine levels between the two groups was observed, but pentosidine is only one member of the large family of AGEs.
The principal mechanism by which AGEs elicit biological function is by binding to and activating of, a membrane receptor, RAGE, which can trigger an array of signalling pathways that are involved in inflammation and tumourigenesis (19, 21, 25, 30). RAGE is a 35-kD trans-membrane receptor belonging to the immunoglobulin super family, localized on the surface of many cell types, such as lymphocytes, endothelial cells, keratinocytes and macrophages, which binds AGEs with high affinity. Given the ability to detect a class of ligands through a common motif, RAGE is a pattern recognition receptor, and can also bind other ligands, such as the high-mobility group box 1 (HMGB1), amyloid beta peptide, degraded extracellular matrix fragments, e.g. fibronectin fragments, and S100 proteins, including S100A7 (psoriasin), S100A12 (EN-RAGE) and S100A15 (koebnerisin) (31–34). Recently, it has been shown that HMGB1 levels are increased in the serum of patients with moderate-to-severe psoriasis (31). HMGB1 may favour the shift of T regulatory cells into Th17 cells (35), which are crucial players of psoriasis induction. The interaction between AGE-RAGE, or RAGE-other ligands, on inflammatory cells stabilizes the receptor in the active state and amplifies inflammation by favouring cytokine and chemokine release, production of reactive oxygen species, activation of metallo-proteases, inhibition of apoptosis and increased cell migration. Inflammation, in turn, is associated with induction of AGEs, including pentosidine, which prolongs and propagates inflammatory response (11–14).
The AGE-RAGE axis plays a critical role in the pathological interplay between hyperglycaemia and vascular homeostasis, and it is believed that the accumulation of AGEs in diabetes may lead to the development of all serious complications of this disease, such as macroangio-pathy, nephropathy, retinopathy or cataract. In addition, AGEs are increased in tissues of other chronic diseases associated with an augmented cardiovascular risk, such as metabolic syndrome, obesity, rheumatoid arthritis, fatty liver disease, and psoriasis (13–18). The main path-way linking AGEs with cardiovascular risk includes activation of the AGE-RAGE axis with liberation of oxygen species that induce endothelial dysfunction, arterial stiffness, direct myocardial damage and chronic coronary and myocardial inflammation (14, 20, 36). Tumour necrosis factor alpha (TNF-alpha) and interleukin-17 (IL-17), which are key cytokines in psoriasis pathogenesis have been shown to increase expression of membrane RAGE in skin fibroblast from healthy individuals and fibroblast-like synoviocytes from patients with rheumatoid arthritis, suggesting a new mechanism by which these cytokines may promote inflammation (37–43). In keeping with this hypothesis, psoriasin, a member of the S100 family of proteins containing 2 EF-hand calcium-binding motifs, is also markedly over-expressed in psoriasis skin (44). In patients with psoriasis, psoriasin is over-released by keratinocytes and binds to RAGE localized on keratinocytes, endothelial cells, lymphocytes and macrophages, activates the RAGE axis, which can induce AGEs and pentosidine production, angiogenesis, keratinocyte hyperproliferation and amplify inflammation. The levels of total soluble RAGE, which comprise both the extracellular domain of full-length RAGE and the endogenous secreted isoform lacking transmembrane domain (esRAGE), were reduced in the serum of patients with psoriasis. The soluble RAGE isoform may, in fact, counteract the detrimental effects of the full-length isoform by acting as a decoy receptor for its ligands during inflammation. The reduced levels of total RAGE in the serum of patients with psoriasis might also be secondary to occupation of RAGE by psoriasin, EN-RAGE and koebnerisin, which are additional S100 proteins up-regulated in the whole epidermis of patients with psoriasis, and bind with high affinity to RAGE, activating the inflammatory cascade (44, 45). Higher than normal levels of AGEs in both lesional and non-lesional skin may indicate that accumulation of AGEs is independent from pre-existing skin inflammation, and that AGEs might thus themselves be a driver of skin inflammation. Recently, a series of small molecules, which competitively inhibit the cytoplasmic tail of RAGE, have been identified (e.g. azeliragon). These compounds inhibit in vitro and in vivo RAGE-dependent molecular processes, such as inhibition of RAGE signal transduction, cellular migration, inflammatory gene expression and ischaemia-induced perturbation of heart function, and may be attractive for the treatment of psoriasis (46).
This study has strengths and limitations. It includes a significant number of patients and controls well matched for metabolic variables that may affect levels of AGEs. Moreover, patients and healthy individuals with a smoking habit, diabetes, dyslipidaemia, hypercholesterolaemia, hypertension or under systemic treatment were excluded from the study. The different results in patients with chronic eczema reinforce the specificity of the findings. Furthermore, the strong correlation between cutaneous and serum levels of AGEs and the association of severe psoriasis with skin and serum AGEs accumulation gives strength to the results. Study limitations include the pure descriptive nature of the study, missing data on cooking habits (d-AGEs) of the participants, and the missing levels of psoriasin, EN-RAGE and koebnerisin.
In conclusion, this study suggests that intensified protein glycation in the skin may have a role in the psoriasis inflammatory signature. Research is needed to understand the relevance of these findings to the patho-physiology of psoriasis. In addition, AGEs released from the skin of patients with severe psoriasis may serve as a link between cutaneous inflammation and increased metabolic and cardiovascular risk, and may finally serve as new therapeutic target for psoriasis.


 Click to show fullsize
Click to show fullsize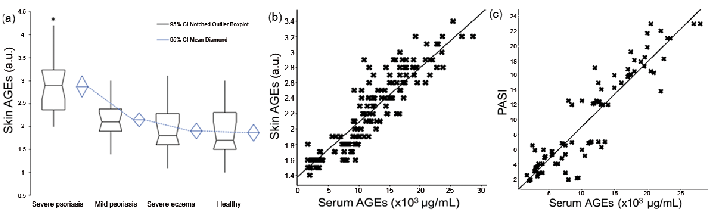 Click to show fullsize
Click to show fullsize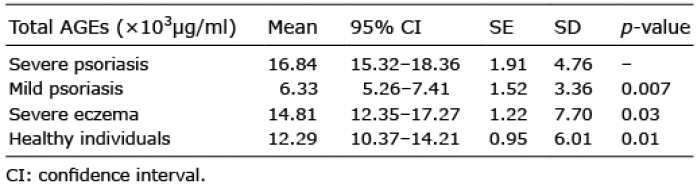 Click to show fullsize
Click to show fullsize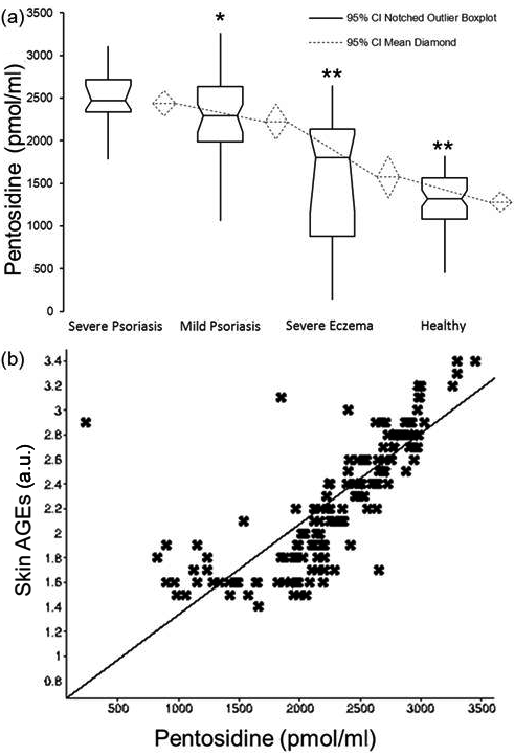 Click to show fullsize
Click to show fullsize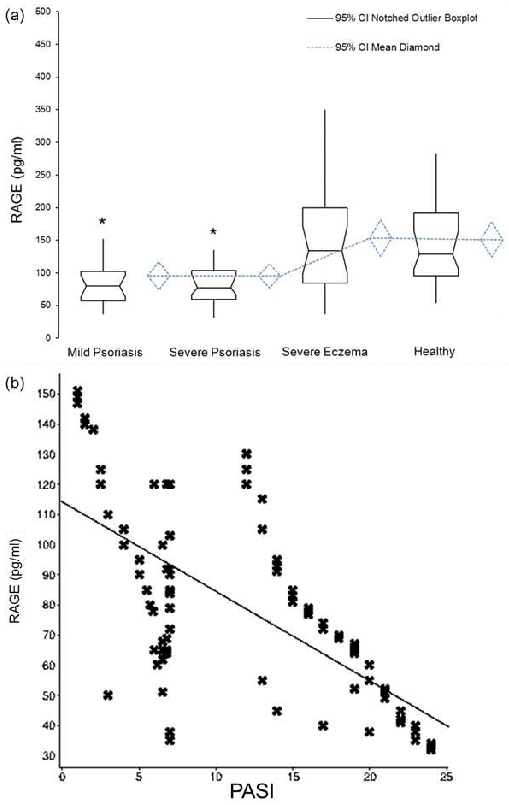 Click to show fullsize
Click to show fullsize