


1Department of Dermatology and Venereology, Sahlgrenska University Hospital, and 2Department of Infectious Diseases, Institute of Biomedicine, The Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden
The aim of this study was to monitor Staphylococcus aureus colonization and disease severity in adults with atopic dermatitis (AD) during 5 months. Twenty-one patients attended 3 visits each for severity SCORing of Atopic Dermatitis (SCORAD) assessment, quantitative cultures from the skin and conventional cultures from the anterior nares, tonsils and perineum. S. aureus isolates were typed for strain identity with pulsed-field gel electrophoresis (PFGE). Seventy-one percent of patients were colonized with S. aureus on lesional skin at least once. Density (colony-forming units (CFU)/cm2) was higher on lesional skin than on non-lesional skin (p < 0.05). Density on lesional skin and number of colonized body sites were positively correlated with SCORAD (p = 0.0003 and p = 0.007, respectively). Persistent carriers of the same strain on lesional skin had higher mean SCORAD index than intermittent/non-carriers (36.3 and 17.1, respectively, p = 0.002). The results show a temporal correlation between several aspects of S. aureus colonization and disease severity in AD raising the question of the importance of this in pathogenesis and treatment.
Key words: atopic dermatitis; S. aureus; SCORAD; PFGE.
Accepted Apr 4, 2017; Epub ahead of print Apr 4, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Mikael Alsterholm, Department of Dermatology and Venereology, Sahlgrenska University Hospital, Gröna Stråket 16, SE-413 45 Göteborg, Sweden. E-mail: mikael.alsterholm@vgregion.se
Staphylococcus aureus is a gram-positive bacteria that can act as a human commensal on the skin as well as a causative agent in several types of skin and soft tissue infections. The carriage pattern of S. aureus in healthy subjects has been studied extensively (1). The nasal cavity, skin, perineum and pharynx can all carry S. aureus, with the anterior nares being the most common site of carriage. Carriage rate on the skin ranges from 5% to 30% depending on body site and whether the individual is a persistent nasal carrier. In contrast, lesional skin of patients with atopic dermatitis (AD) is reported to be colonized with S. aureus in 70% of cases (2). Flare-ups of AD are often associated with S. aureus super-infection, and one treatment strategy is the use of topical or oral antimicrobials (3). While there is a strong link between acute S. aureus infection of the skin and increase in disease activity, the role of colonization in the pathogenesis and maintenance of AD remains unclear.
A currently favoured theory in AD pathogenesis is the “outside-in” hypothesis, whereby an impaired epidermal barrier, allowing penetration of environmental substances into the skin, is described as the starting point in an early march towards atopy (4). As a consequence there is sensitization to microbial products and allergens, which in turn triggers an immune dysregulation followed by inflammation of the skin. In 1990, Williams et al. (5) demonstrated a positive correlation between S. aureus density on lesional skin and the severity of AD, later confirmed by numerous other investigators (6). In recent years, several studies have demonstrated a higher disease activity in AD associated with the presence of S. aureus and sensitization to staphylococcal toxins (7–12). Lomholt et al. (13) reported that a change from one colonizing strain of S. aureus to another was associated with increased disease activity in children with AD.
In view of this, it is somewhat surprising that there is little, and also conflicting, data to support the efficacy of anti-staphylococcal interventions in patients, primarily children, with clinically non-infected AD (14–16). The failure to demonstrate convincing clinical benefit could be due to a lack of high-quality randomized controlled trials, as concluded in a Cochrane review on this topic (17). Another explanation could lie in the selection of patients for interventional studies. Presumably, the pattern of S. aureus colonization varies between patients. It could be suggested that only those with persistent and high-density colonization are likely to benefit from anti-staphylococcal interventions.
Variation in S. aureus colonization over time in relation to severity of AD has, to our knowledge, rarely been described in adult patients. Therefore, we investigated S. aureus carriage in adults with AD at repeated visits during a 5-month follow-up period to investigate whether any temporal shifts in S. aureus carriage occurred and if this could be related to disease severity measured with the SCORAD index.
The study was conducted at the Department of Dermatology and Venereology, Sahlgrenska University Hospital and at the Department of Infectious Diseases, Institute of Biomedicine, The Sahlgrenska Academy at the University of Gothenburg in 2010–2012.
The patient records for all patients, 18 years or older, given the diagnostic code “Prurigo Besnier (atopic dermatitis) L20.0” according to the Swedish version of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) during the period 1 January to 22 September 2010, were reviewed (n = 489). All patient records, which described moderate to severe AD without ongoing systemic anti-inflammatory treatment, long-term treatment with antibiotics or phototherapy, were selected (n = 78). These patients were contacted in random order and offered participation until 20 patients had agreed to participate. Due to complete and partial loss to follow-up for 2 patients in the early stages of the study (patient 6 and 10, respectively), 2 additional patients were recruited.
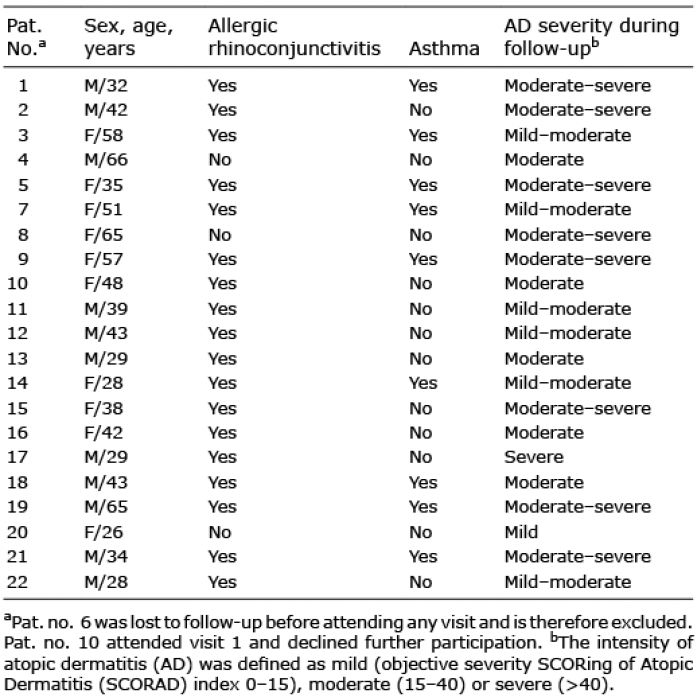
In total, 11 men and 10 women fulfilling the criteria for AD according to Hanifin & Rajka (18) participated in the study. The age ranged from 26 to 66 years (mean 42.8 years, median 42.0 years). For individual clinical data see Table I.
Table I. Clinical characteristics of participating patients
All patients were asked to attend 3 visits, evenly spaced over 5 months, during January to June 2011. They were also instructed to contact the investigators in case of a flare-up of AD. At all visits, SCORAD assessment was performed and quantitative and qualitative cultures for S. aureus were obtained by the same investigator (MA).
The patients were instructed to continue their usual treatment regimen (emollients and/or topical corticosteroids and/or topical calcineurin inhibitors) as needed during follow-up. The use of topical antimicrobials was not allowed at any time. The patients were asked not to apply any topical treatments on the morning of their visits.
The severity of AD was assessed with the SCORAD index (19, 20). The combination of an area estimation and intensity grading by the investigator renders a score referred to as objective SCORAD index (range 0–83). Patients were asked to grade their average pruritus and sleep loss, respectively, during the previous 3 days and nights, using a visual analogue scale. This subjective grading renders an additional score, which is added to the objective SCORAD score, resulting in the total SCORAD index (range 0–103). The intensity of AD was defined as mild (objective SCORAD index 0–15), moderate (15–40) or severe (> 40) according to the classification of Oranje et al. (21).
Cultures were obtained from representative sites of lesional skin, as well as from non-lesional skin. The arm was the preferred site of sampling, but the trunk or leg was also used. The sampling and culture method was an adaptation of methods previously described (22, 23). A stainless steel ring with an inner area of 5.5 cm2 was placed on the skin and held in place with moderate pressure by 2 fingers. One millilitre of dispersed detergent (phosphate-buffered saline (PBS), pH 7.9, with 0.1% Triton X-100) was applied inside the ring. The skin was then rubbed with a glass rod for exactly 1 min. The dispersed detergent, now containing skin surface microbes in single-cell suspension, was aspirated and aliquoted. Serial 10-fold dilutions were immediately prepared. A 100 µl volume of each dilution was plated on blood agar plates (Columbia agar; Oxoid, Basingstoke, UK) + 5% defibrinated horse blood). Plates were incubated for 24–48 h at 37°C.
All morphologically different colonies found after incubation were tested with a S. aureus-specific agglutination test (Slidex® Staph Plus; Biomérieux, Lyon, France). All Slidex® Staph Plus-positive isolates were verified with the tube coagulase test as S. aureus. The S. aureus alike colonies on the plates were counted manually. The density of S. aureus on the skin expressed as colony-forming units (CFU)/cm2 was calculated. All S. aureus isolates were cultured on new blood agar plates and then kept in freezing medium at –80°C.
Swab samples for S. aureus cultures were collected from the anterior nares, tonsils and perineum at each visit. Samples were cultured at the Clinical Microbiology Laboratory, Sahlgrenska University Hospital according to standard laboratory procedures. S. aureus isolates were verified and stored as above.
All S. aureus isolates found on lesional skin, in the anterior nares and perineum and selected S. aureus isolates found on non-lesional skin were typed for strain identity with pulsed-field gel electrophoresis (PFGE), as previously described (24). Briefly, smaI digested DNA was electrophoresed in 1% agarose in 0.5 × TBE at 14°C for 23 h, using the Gene Path system (Bio-Rad Laboratories, Sweden), set at 6 V/cm, with pulse times linearly increased from 5 s initial switch time to 60 s final switch time. smaI-digested DNA from S. aureus NCTC 8325 was included as a normalization standard on every gel. The DNA band patterns were analysed using BioNumerics software version 6.6 (Applied Maths NV, Sint-Martens-Latem, Belgium) with the Dice coefficient for calculating pair-wise similarities, and the UPGMA algorithm for constructing dendrograms of estimated relatedness. Position tolerance and optimization were set at 1.0%. Interpretation of strain similarity was performed according to previously published guidelines (25, 26). Strains were assigned the same PFGE-type if the similarity was ≥ 80%.
Persistent carriage was defined as S. aureus of the same PFGE-group on lesional skin at all 3 visits or at 2 visits and negative at the remaining visit. Intermittent carriage was defined as detection of low counts of S. aureus (less than 103 FU/cm2) at one visit, negative at remaining visits. Non-carriage was defined as S. aureus-negative at all 3 visits.
All data were analysed using R version 2.14.2 (The R Foundation for Statistical Computing, Vienna, Austria). Comparison of S. aureus density on lesional and non-lesional skin was made with Wilcoxon sign-rank test. Mean objective SCORAD index for persistent S. aureus carriers and non- or intermittent carriers was compared with Wilcoxon rank-sum test. Correlation between the density of S. aureus on lesional skin and objective SCORAD index was analysed with linear regression. The number of S. aureus-positive body sites was related to objective SCORAD index with generalized least square regression. The significance level was p < 0.05.
The study design was approved by the regional ethics committee, Gothenburg, Sweden. Participants received oral and written information about the study before their written consent was obtained.
A total of 21 patients participated in the study, of which 19 attended all 3 visits. The objective SCORAD index showed that 90% (19/21) of patients exhibited moderate AD at 1 or more visits, for some fluctuating to mild (6/19) or severe (8/19) (Table I).
Altogether, 71% (15/21) of the patients were found to be colonized with S. aureus on lesional skin at one or more visits and 62% (13/21) at 2 or more visits. By comparison, 90% (19/21) of patients were colonized with S. aureus on non-lesional skin at least once. For those colonized on non-lesional skin, counts were generally low (Table SI).
The number of body sites colonized with S. aureus was positively correlated with the objective SCORAD index (p = 0.007, R2=0.46) (Table II, Fig. 1). Statistical analysis was made with generalized least square regression for all observations from all visits and with linear regression for all observations from each visit separately (data not shown) with similar result.
Table II. Frequency of patients with S. aureus isolates on different body sites at visit 1, 2 and 3. Expressed as percentage of total number of patients sampled at each visit
Fig. 1. Mean objective severity SCORing of Atopic Dermatitis (SCORAD index) related to the mean number of body sites carrying S. aureus and the carriage pattern of S. aureus strains on lesional skin during follow-up. Investigated body sites were lesional skin, non-lesional skin, anterior nares, tonsils and perineum). Persistent carriage (black circle) defined as S. aureus of the same pulsed-field gel electrophoresis (PFGE)-group on lesional skin at 3 visits or at 2 visits and negative at the remaining visit. Intermittent carriage (black triangle), defined as detection of low counts of S. aureus (<103 colony-forming units (CFU)/cm2) at 1 visit, negative at remaining visits. Non-carriage (black square), defined as S. aureus-negative at all 3 visits. Each dot represents the mean SCORAD index, the mean number of S. aureus positive body sites and the carriage pattern of S. aureus strains on lesional skin during follow-up for 1 patient (n = 21). Statistical analysis with generalized least square regression for correlation between mean objective SCORAD index and mean number of S. aureus positive body sites (p = 0.007, R2=0.46). Statistical analysis with Wilcoxon rank-sum test for the comparison of mean objective SCORAD index for patients with persistent carriage (36.3) vs. patients with non-/intermittent carriage (17.1) (p = 0.002). The significance level was p < 0.05.
The density of S. aureus on non-lesional skin was typically low and ranged from non-detectable to, at most, 5.5 × 104 CFU/cm2 (mean 9.1×102 CFU/cm2, median 1.9 × 10 CFU/cm2) whereas the density of S. aureus on lesional skin ranged from non-detectable to 9.6 ×107 CFU/cm2 (mean 2.6 × 106 CFU/cm2, median 6.5 × 10 CFU/cm2) (Table SI).
The mean S. aureus density was higher on lesional skin than on non-lesional skin at all visits (p = 0.04, p = 0.02 and p = 0.02 for visits 1, 2 and 3, respectively). Higher density of S. aureus on lesional skin corresponded to more severe disease, measured as objective SCORAD index (visit 1, p = 0.0003, R2 = 0.49; visit 2, p = 0.0003, R2=0.52; visit 3, p = 0.004, R2=0.35) (Fig. 2).
Fig. 2. S. aureus density on lesional skin related to objective severity SCORing of Atopic Dermatitis (SCORAD) index at visit 1, 2 and 3. Density expressed as log10 (colony-forming units (CFU)/cm2 +1) in order to include observations without S. aureus in the figure. Visit 1 (n = 21), visit 2 (n = 19) and visit 3 (n = 20). Statistical analysis with linear regression. Significance level was p < 0.05.
PFGE was performed on all S. aureus isolates from lesional skin (n = 39), the anterior nares (n = 36) and perineum (n = 20) and on a majority of isolates from non-lesional skin (n = 25 out of 36 found) (Table SI).
Altogether 55% (11/20) of patients were persistent carriers of a specific strain on lesional skin, whereas 35% (7/20) of patients were non-carriers (5/7) or intermittent carriers (2/7) on lesional skin. The mean objective SCORAD index was significantly higher among persistent carriers than among non-carriers plus intermittent carriers (36.3 and 17.1, respectively) (p = 0.002) (Fig. 1). One patient (patient 10) was excluded from this analysis because the samples were from only one visit.
Seventy-six percent (16/21) of patients were colonized with S. aureus in the anterior nares at least once during follow-up and 65% (13/20) were colonized at 2 or more visits. A different strain compared with the strain colonizing the skin was found in 24% (5/21) of patients (Table SI).
S. aureus was isolated from the perineum at least once in 11 patients. All strains were concordant with the strains simultaneously found elsewhere on the skin (Table SI).
Two patients experienced flare-ups of AD during follow-up, but unfortunately were not cultured at the time of flare-up (Table SI). Patient 17 flared 1 month prior to visit 3 and was treated with oral flucloxacillin for 10 days without contacting the study investigator. The same S. aureus strain was found on lesional skin before and after treatment (Table SI). Patient 21 flared 2 months prior to visit 2 and was treated with oral clindamycin for 14 days after telephone counselling. The lesional skin was colonized with strain S prior to treatment (visit 1), not colonized with S. aureus at all at visit 2 and finally colonized with strain N at visit 3.
Two additional patients were treated with antibiotics unrelated to AD, as detailed in Table SI.
Research in the field of AD tends to focus on children; however, AD is not just a disease of the young, it often persists in adulthood and even in old age (27). We there-fore believe that it is important to study the dynamics of S. aureus colonization in order to understand the influence that they might have on the severity of AD in an adult population.
We have studied S. aureus colonization and SCORAD index in adult patients with AD during 5 months. The patients experienced moderate to severe AD, which they felt were sufficiently managed with their pre-existing treatment. They were not treated with antimicrobials (topical or systemic), ultraviolet (UV) therapy or oral immunomodulation drugs, as these treatment modalities can affect the skin microbiome, including S. aureus (28–30). Also, during the study period, little natural exposure to UV occurs in Sweden. The mean objective SCORAD index for all participating patients and the mean number of S. aureus isolates found were similar at all visits, indicating a lack of general improvement of AD or change in the number of S. aureus isolates found at visit 3 in June, the first month of Swedish summer.
There were few flare-ups of AD that prompted patients to seek medical advice during follow-up. Therefore, the data primarily represents the normal variation in disease intensity for adult patients with moderate to severe AD.
The patients were colonized with S. aureus on lesional skin, non-lesional skin, in the anterior nares, tonsils and perineum to a higher extent than is reported for the general population (1). In fact, carriage rates were similar to those seen among persistent nasal carriers of S. aureus, even though 24% (5/21) of patients were non-carriers in the anterior nares during follow-up. Nasal colonization with S. aureus is a risk factor for staphylococcal skin infection and presumably also for colonization/recolonization of atopic skin (1, 31). While the nose is the main ecological niche for S. aureus in humans it is possible that the skin could serve as an equally important reservoir in patients with AD (32). Fibronectin is redistributed to the cornified layer in atopic skin; an observation not made in normal skin, and can serve as an important binding site for S. aureus through fibronectin-binding protein (Fnbp) (33). Interestingly, 24% (5/21) of patients in this study carried a different S. aureus strain in the anterior nares compared with lesional skin at one or several visits, demonstrating that nasal carriage does not always determine which strain is carried on the skin.
There appeared to be 2 subgroups of patients with regards to S. aureus colonization on lesional skin; persistent carriers and non-/intermittent carriers. The persistent carriers had significantly higher mean objective SCORAD index than non-/intermittent carriers. This supports previous findings that S. aureus carriage on lesional skin is associated with more severe AD (5, 8, 13, 34). Also, linear regression analysis showed that patients with more severe AD had higher density of S. aureus on lesional skin and carried S. aureus on multiple body sites.
Since atopic skin is prone to colonization with microbes, specifically S. aureus, it could be hypothesized that patients would readily pick up new strains. It has also been proposed that colonization with a new S. aureus strain could provoke an increase in disease severity, presumably by introducing a new trigger for the immune system (13). Therefore, we wanted to investigate any temporal shifts in S. aureus strain carriage among our patients and relate this to disease severity. Since our primary aim was to establish isolate interrelationships we chose to type for strain with PFGE, which was the gold standard for typing bacteria at the time of the study and is still extensively used for this purpose (25). Our results indicate that increases in AD intensity, in the absence of acute flare-ups and antimicrobial treatment, are associated with a change in S. aureus density on lesional skin, but not with a change of strain. In fact, the patients with the most severe AD were persistent carriers of the same strain on lesional skin and on multiple other sampled sites during follow-up.
Despite extensive efforts by the research community to understand the complex interplay between S. aureus and atopic skin the question remains: is S. aureus a primary trigger of dermatitis or is colonization a secondary phenomenon due to a beneficial environment for S. aureus in the altered epidermal barrier of AD? A causal relationship between S. aureus colonization and severity of AD cannot be inferred from the temporal association in our study or the similar association shown by others in cross-sectional studies. However, the findings raise the question of causality and the possible implications for treatment.
So far, there is little evidence for the efficacy of staphy-lococcal reducing therapies in clinically non-infected AD, as extensively reviewed in 2010 (17). A recent randomized, placebo-controlled, single-blinded clinical trial in 21 children with AD compared the cutaneous microbiome and AD severity before and after 4 weeks with topical corticosteroids alone or topical corticosteroids in combination with intermittent bleach baths (16). S. aureus density on the skin and AD severity decreased similarly in both treatment groups, indicating that the bleach bath intervention did not contribute to the treatment result. In contrast, a randomized, placebo-controlled, investigator-blinded study including 31 children with AD and a similar therapeutic approach (3 months of intermittent intranasal mupirocin and bleach baths vs. intranasal petrolatum ointment and plain water baths) demonstrated decreased AD severity among those who received anti-staphylococcal treatment (15). The conflicting results could mean that the density of S. aureus is secondary to the inflammatory changes in atopic skin and without real significance for the pathogenesis and maintenance of AD. Instead, the mere presence of S. aureus, an acknowledged inflammatory trigger, rather than the actual amount of bacteria, might be an important pathogenic factor. Conversely, it could mean that the studies that have been performed to date have been unable to detect significant effects due to relatively few participants, short follow-ups or insufficient characterization of the participants with regard to S. aureus colonization at inclusion. It is important to consider that anti-staphylococcal treatment may be effective for patients who are persistent S. aureus carriers, but probably less so for intermittent carriers. We believe that persistent high-density carriers, as well as intermittent carriers, need to be identified in the inclusion process of future clinical trials.
The skin microbiome before, during and after disease flares, analysed using 16S ribosomal RNA bacterial gene sequencing, has been described previously in children with AD (35). Microbial diversity on lesional skin was dramatically reduced during flare-ups, but changed towards higher diversity post-treatment. Flare-ups were characterized by a build-up to high numbers of one species, typically staphylococci, while an increasing proportion of Streptococcus, Propionibacterium, Corynebacterium and other species were observed following therapy.
Taken together, it is an appealing thought that intermittent long-term treatment with topical preparations could prevent the dominance of S. aureus and promote microbial diversity on atopic skin. Assuming causality, this could, in turn, potentially reduce overall disease severity, number of flare-ups and antibiotic consumption for patients with AD who are persistent carriers of S. aureus on lesional skin. Preferably, antiseptics such as clioquinol, potassium permanganate or dilute bleach baths should be used, since it is vital to minimize the use of topical and oral antibiotics.
In summary, we describe here the temporal shift in S. aureus density, strain distribution and disease severity in adult patients with AD. Colonization with S. aureus on lesional skin and multiple other sites is associated with more severe disease. Even in the absence of acute flare-ups objective SCORAD index varied greatly for the individual patients. These variations occurred without a shift in strain, but with concomitant changes in S. aureus density on lesional skin. Causality between the degree of S. aureus colonization and AD severity can neither be assumed nor rejected based on our data. Intermittent anti-staphylococcal treatment could be beneficial in AD. More clinical trials investigating the effects of anti-staphylococcal treatment in patients with AD persistently colonized with S. aureus are needed.
This work was supported by the Edvard Welander Foundation and by ALF, Gothenburg, Sweden.


 Click to show fullsize
Click to show fullsize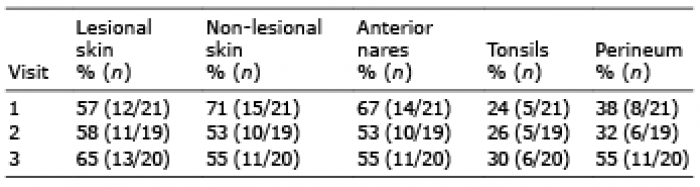 Click to show fullsize
Click to show fullsize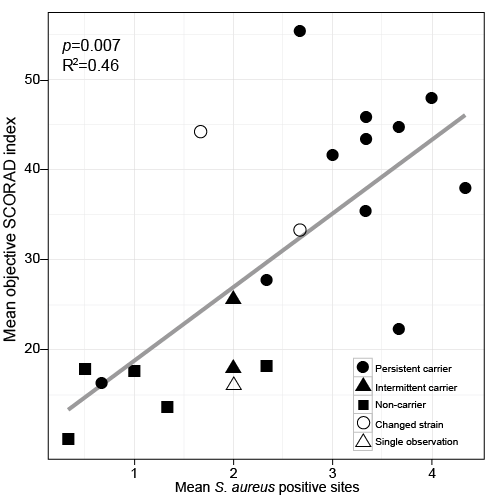 Click to show fullsize
Click to show fullsize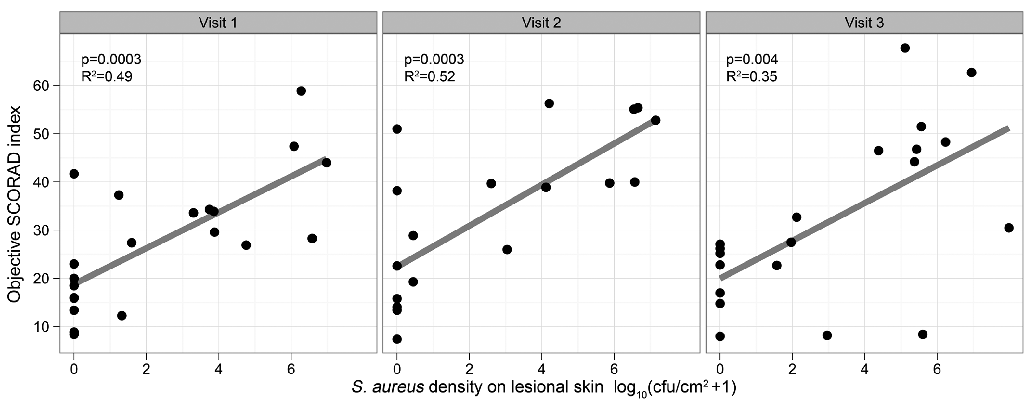 Click to show fullsize
Click to show fullsize