


1Department of Preventive Medicine, Korea University College of Medicine, Seoul, and 2Department of Dermatology, Incheon St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
#These authors contributed equally to this work.
Tranexamic acid is a novel treatment option for melasma; however, there is no consensus on its use. This systematic review searched major databases for relevant publications to March 2016. Eleven studies with 667 participants were included. Pooled data from tranexamic acid-only observational studies with pre- and post-treatment Melasma Area and Severity Index (MASI) showed a decrease of 1.60 in MASI (95% confidence interval (CI), 1.20–2.00; p < 0.001) after treat-ment with tranexamic acid. The addition of tranexamic acid to routine treatment modalities resulted in a further decrease in MASI of 0.94 (95% CI 0.10–1.79; p = 0.03). Side-effects were minor, with a few cases reporting hypo-menorrhoea, mild abdominal discomfort, and transient skin irritation. These results support the efficacy and safety of tranexamic acid, either alone or as an adjuvant to routine treatment modalities for melasma.
Key words: tranexamic acid; melasma: systematic review;
meta-analysis.
Accepted Apr 3, 2017; Epub ahead of print Apr 4, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Hei Sung Kim, Department of Dermatology, Incheon St Mary’s
Hospital, The Catholic University of Korea, 56 Dongsuro, Bupyeong-gu, 150-713, Incheon, Korea. E-mail: hazelkimhoho@gmail.com
Melasma is a common acquired disorder of facial pigmentation with predominance in the Asian population. Various treatment modalities have been used, but with inconsistent results (1, 2). Topical bleaching agents are the mainstay of treatment, but are often insufficient. Intense pulsed light (IPL) or laser-based treatments have conflicting outcomes with significant side-effects, such as mottled hypopigmentation and paradoxical darkening of melasma (3).
Increased pigmentation is the main feature of melasma. Although the exact pathogenesis is unknown, it has been hypothesized that melasma is induced by biologically active melanocytes (4). Increased vascularity in the affected skin and elevated expression of angio-genic factors in the epidermis have been found. These factors may play an important role in the development of melasma (4–6).
Tranexamic acid (TA), a synthetic derivative of lysine, is a well-known haemostatic agent. TA is anti-fibrinolytic. It can inhibit plasminogen activation through the reversible blockade of lysine-binding sites on plasminogen molecules (7).
In recent years, off-label TA has emerged as potential treatment for melasma (5, 8). Although the mechanism of action remains unclear, it is thought that TA may inhibit melanin synthesis by blocking the interaction between melanocytes and keratinocytes. TA may also reverse the abnormal dermal changes associated with melasma, such as the aforementioned increased vasculature (9).
While different forms of TA (i.e. oral, topical and localized microinjections) have shown promising results (7, 9–11), there is a lack of support for its efficacy and safety in melasma due to the absence of sufficiently powered randomized controlled trials (RCTs). Through a systematic review of the literature, we aimed to investigate the effectiveness and safety of TA, alone, or as an adjuvant, in patients with melasma.
A systematic review and meta-analysis were conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) statement (12).
A systematic review of studies of the effect of TA in melasma was carried out. In order to collect all available evidence, EMBASE (1988 to present), MEDLINE (1946 to present), Web of Science (1975 to present), Scopus (1996 to present), and the Cochrane Central register of Controlled Trials (CENTRAL) (1991 to present) databases were searched on 4 March 2016, without limitation as to dates or language. To search for studies of TA, the following keywords were used: “tranexamic acid’, “antifibrinolytic agents” and ‘tranexamic”. To search for melasma, the following keywords were used: “melanosis”, “chloasma”, “chloasmas”, “melasma”, and “melasmas”. The full search strategy, shown in Appendix S1, was developed for MEDLINE and tailored to the other electronic databases.
Inclusion criteria were: original reports (study, case series, item of correspondence, posters and meeting abstracts) describing treatment with any form of TA, alone or as an adjunct in melasma (human). According to the pre-defined criteria, 2 authors (H.J.K. and H.S.K.) independently selected reports based on the title and abstracts. Any discrepancies were resolved in consultation with a third party (S.H.M.). The first 2 authors then examined the full texts of those reports. Duplicate publications were identified by several criteria (authors, title, intervention characteristics, and number of patients). In case of duplicates, the most complete report was chosen. Studies with pre- and post-treatment Melasma Area and Severity Index (MASI) were included in meta-analysis, regardless of the mode of delivery of TA. In addition, studies comparing changes in MASI between a routine melasma treatment and those with TA as an adjuvant were analysed.
For each selected report, 2 authors (S.H.M. and H.S.K.) independently extracted information on the first author, publication year, country/setting, study design, characteristics of patients, dose and type of TA (i.e. oral, topical, microinjection) used, co-intervention, outcome (efficacy and side-effects) and duration of follow-up. Any disagreement was resolved by discussion. A data table was established for each patient. The extraction table was developed by 3 dermatologists (C.S.H., L.J.D. and K.H.S.) who are familiar with melasma. For missing data, the first author of the report was contacted when possible.
The risk of bias and methodological quality were assessed as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (13). For RCTs, the Cochrane Collaboration’s “risk of bias” tool was used. We adopted the risk of bias criteria suggested by Cochrane Effective Practice and Organization of Care (EPOC) and Newcastle-Ottawa Scale for other study designs. The magnitude of effect and quality of evidence for each outcome were assessed. Two investigators (H.J.K. and H.S.K.) independently assessed the methodological quality of each study. Any disagreement was resolved by consensus or by consultation with a third investigator (S.H.M.). Publication bias was not assessed due to the small number of studies.
Meta-analysis was conducted using Review Manager (RevMan) Version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The main outcomes of the meta-analysis were the standardized mean difference in MASI pre- and post-TA and difference in changes in MASI between a certain melasma treatment and that with TA as an adjuvant. Pooled analyses were conducted using the inverse variance method with random-effects weighting and reported as the standardized mean difference and 95% confidence intervals (CIs). Subgroup analyses were conducted in these cases by the route of TA administration, type of “other melasma treatment” (i.e. topical bleaching agent, IPL and lasers) and type of study design (RCT, retrospective cohort study, before and after study design).
Heterogeneity of the trial results was assessed by virtually examining the forest plot to detect non-overlapping CIs, using the χ2 test of heterogeneity (with p < 0.1 indicating statistical significance) and the I2 statistic of inconsistency (with 30–60% denoting moderate, > 60% high levels of heterogeneity).
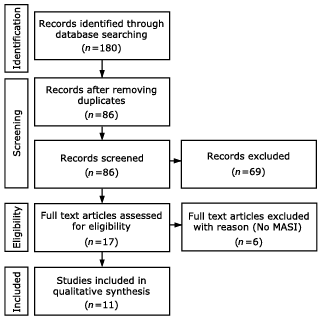
The literature search yielded 86 titles and abstracts after removing duplicates. After excluding studies that did not meet criteria for inclusion in the analysis, 11 studies were deemed appropriate and were included for meta-analysis (Fig. 1) (7, 14–23). Among the included studies we had 1 abstract and 1 poster material (15, 17).
Fig. 1. Literature search for tranexamic acid in melasma. Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) flowchart. MASI: Melasma Area and Severity Index.
Characteristics of the included trials are summarized in Table I and Table SI. A total of 667 melasma patients were included. All study patients were adults; 80–100% women. Of the 11 trials, 4 were from Korea (7, 15, 22, 23), 3 from India (17, 18, 21) and 1 from each of the following countries: Brazil (16), Iran (19), Nepal (20) and Singapore (14). Melasma severity was assessed by MASI (8 studies were assessed with the original MASI scoring (24) and 3 with 2 different forms of modified MASI scoring (18, 25)).
Table I. Treatment outcomes of trials included in this study
The regimens for TA treatment (mode of delivery, dose, applied alone or as an adjuvant, duration, etc.) differed among these studies. Oral TA (500–1,500 mg/day) was applied alone in 2 studies (14, 15) and as an adjuvant in 3 studies (20, 21, 23) for 2–6 months. Topical TA in 2–3% concentrations was applied alone in 2 studies (16, 19) and as an adjuvant in one study (22) for 3–7 months. TA microinjection (including micro-needling) was applied alone in 4 studies (7, 16–18) on a weekly or monthly basis for 3–6 months.
Of the 11 studies included, 3 were RCTs (16, 20, 21), 7 were before-after comparison (7, 14–19) and one was a retrospective cohort study (23). The quality of the studies evaluating TA treatment in melasma varied, but was generally poor (Fig. 2).
Fig. 2. Risk of bias and methodological quality were assessed. For randomized controlled trials, Cochrane Collaboration’s “risk of bias” tool was used (upper right panel). Cochrane Effective Practice and Organization of Care (EPOC) (upper left panel) and Newcastle-Ottawa Scale (lower panel) were adopted for other study designs.
MASI reduction (change in MASI between pre-treatment and post-treatment) was the primary outcome measure of 7 melasma studies with TA application alone (7, 14–19). With oral TA (14, 15), the standardized mean reduction in MASI was 2.46 (95% CI 1.13–3.80; p < 0.001; I2 =71%). MASI was reduced by 1.42 (95% CI 0.98–1.87; p < 0.001; I2 =72%) after TA injection (7, 16–18) and showed a decrease of 1.36 (95% CI –0.17–2.90; p = 0.08; I2 =87%) with topical TA (16, 19). Overall, TA treatment alone caused a reduction of 1.60 (95% CI, 1.20–2.00; p < 0.001; I2 =74%) in MASI (Fig. 3). There was high and statistically significant heterogeneity within TA alone subgroups, as shown in the wide confidence intervals. Heterogeneity among the subgroups (oral TA, TA microinjection, topical TA) was low (I2=6.3%).
Fig. 3. Tranexamic acid (TA) in melasma. Forest plot of standardized mean reduction in Melasma Area and Severity Index (MASI) by different forms of TA (upper panel) and standardized mean reduction in MASI with TA as an adjuvant vs. routine melasma treatment (lower panel). CI: confidence interval.
In 4 studies (20–23), MASI reduction was compared between routine treatment and routine treatment with TA as an adjuvant. For routine treatments, topical hydroquinone (n = 1) (20), triple combination cream (n = 1) (21), IPL (n = 1) (22) and IPL+Q-switched neodymium-doped yttrium aluminium garnet (Q-switched Nd: YAG) laser toning (n = 1) were used (23). Oral TA was applied as an adjuvant in 3 trials (20, 21, 23) while topical TA was used in one trial (22). Of the 4 TA trials, 3 were RCTs (20–22) and 1 a retrospective cohort study (23). They were sub-classified accordingly. Meta-analysis of the RCTs showed that MASI reduction was greater in the TA adjuvant group by 0.94 (95% CI 0.10–1.79; p = 0.03; I2 = 84%). The addition of TA was also found to result in a further reduction of MASI by 0.46 (95% CI –0.09–1.02, p = 0.10) in the retrospective cohort study. The heterogeneity was high within the RCT subgroup (I2 = 84%), but was low between the 2 TA adjuvant subgroups (I2 = 0%) (Fig. 3).
Adverse events were identified in 4 studies (Table I) (15, 18–20). With oral TA, one study reported oligomenorrhoea (14.7% of female patients), belching (9.2%), abdominal cramps (6.9%), palpitation (2%) and urticarial rash with angioedema (2%) (20), while another study reported headache (11%) (15). With topical TA, a single study reported erythema, skin irritation, xerosis and scaling as side-effects (19). TA microinjection was said to cause mild discomfort, burning sensation, and erythema for 1–2 days in one study (18).
Melasma is a common pigmentary disorder, with a preponderance in Asian females. This was also apparent in our review, with 80–100% of the study participants being women. All 11 trials (7, 14–23) were from Asian countries, with the exception of 1 study from Brazil (16). Melasma is psychologically distressing. Although various treatment options have been offered, no mode of treatment guarantees satisfactory results (4, 8). Management of melasma remains challenging and the search for a safe and effective therapy continues.
The exact pathogenesis of melasma remains unclear, but genetic influences, ultraviolet (UV) exposure, and hormonal therapy have been reported as possible causative factors (5, 8, 26). Although epidermal hyperpigmentation is the key feature of melasma, increased dermal vascularity and expression of angiogenic factors also play a role and have remained important areas of interest in pigment research (4–6). TA can inhibit melanin synthesis by interfering with keratinocyte-melanocyte interaction, through its effects on the plasminogen-plasmin pathway (14). In addition, it has been postulated that TA is effective in modulating the vascular component of melasma (6, 9). Histological evaluation in prior studies have identified reduced erythema and decreased number of vessels, which is probably the result of the anti-angiogenic effects of TA (6, 9). The use of TA for melasma was first reported (27) in 1979. Since then, TA has been applied to melasma in oral (14, 15), topical (16, 19), and intralesional forms (16–19), and in combination with Q-switched Nd: YAG laser and IPL (22, 23).
The aim of this systematic review was to assess the efficacy and safety of TA in melasma. Our results show that TA is beneficial for melasma, either alone or as an adjuvant to other treatment modalities. Pooled data on TA-only observational studies with pre- and post-treatment MASI showed a 1.60 decrease in MASI (p < 0.001) after TA treatment. In terms of the subgroups, the standardized decrease in MASI was the greatest with oral TA, followed by that with TA microinjection and topical TA. Heterogeneity among the 3 subgroups (oral, microinjection, topical) was low, suggesting that the difference in MASI reduction is insignificant. In these studies, post-treatment MASI was assessed 3–6 months after the commencement of TA, with the majority (71.4%) being checked after 3 months. The findings suggest that pigment lightening is likely to be apparent after 3 months of therapy.
Prior studies have suggested that TA is a good adjunct for refractory cases as a second- or third-line agent (8, 23, 28). Our meta-analysis showed consistent findings; the addition of TA to routine treatments resulted in a further decrease in MASI by 0.94 (p = 0.03) in the RCTs subgroup. As an adjuvant, oral TA was most popular and tested in the majority (93.1%) of our study patients. In clinical practice, oral TA is often combined with topical hydroquinone or triple combination cream. It is also routinely used with lasers and light therapy (i.e. Q-switched Nd: YAG laser, IPL) to minimize aggravation of melasma including post-inflammatory hyperpigmentation.
The present standard of care for melasma is the triple combination cream, which contains hydroquinone 4%, tretinoin 0.05%, and fluocinolone acetonide 0.01%. It is nevertheless important to compare the effect of TA in melasma with that of reference treatment, but we were not able to find a direct comparison study. To overcome this problem, we analysed the triple combination studies (21, 29–32) and identified their standardized mean reduction in MASI. In these studies, post-treatment MASI was assessed after a mean of 3 months. Overall, the triple combination cream reduced MASI by 1.14 (95% CI 0.57–1.72; p < 0.001; I2 =78%), which was less pronounced than the values obtained from all 3 forms of TA (oral TA, TA injection and topical TA).
Melasma is known to have a high relapse rate (26). In one of the studies (14), oral TA alone resulted in a decrease in MASI by 1.89 at 3 months follow-up. However, to the authors’ disappointment, 72% of patients reported a relapse within 2 months of TA cessation. This suggests that TA treatment should not be short-term, but needs to be maintained for an extended period of time. The optimal time of maintenance needs to be further studied.
From our systematic review, TA was well-tolerated, with a small proportion of patients experiencing transient adverse effects. Adverse events mentioned in association with oral TA (dosages between 500 and 1,500 mg/day) were generally minor, some (e.g. oligomenorrhoea) being associated with the haemostatic effects of TA. Although oral TA is an anti-fibrinolytic with potential side-effects, such as deep vein thrombosis, massive pulmonary embolism, and acute myocardial infarction, no thromboembolic adverse events have been reported with low dosages of TA used in the treatment of melasma (14). When TA is used as a haemostatic treatment, it is prescribed at a dosage of 1,000 mg 3 times daily. For melasma, it is commonly used at a dosage of 250 mg twice daily, which is only one-sixth of the normal dosage of TA as a haemostatic agent. Clinicians should ask patients questions regarding risk factors in both personal and family history before prescribing TA treatment. There was only one case of study withdrawal in association with an adverse event (headache) (15).
This systematic review has several limitations. First, we were not able to determine the inter-study variability in the type or severity of melasma. Secondly, there was a lack of data on ongoing sun-exposure in treated patients. Also, studies included in this systematic review had various follow-up times, used different forms of MASI scoring and carried unknown dose-response curves of TA for melasma, which implies that the treatment protocols used were not necessarily optimal. Our pre-emptive decision to pool data from TA studies with different routes of administration and variation in treatment algorithm (in terms of dose, number of procedures, time sequence of the procedures, concurrent treatments, etc.) also created some heterogeneity. Despite these limitations, this systematic review and meta-analysis provides a snapshot of the best level of evidence currently available on the use of TA in the management of melasma.
This systematic review and meta-analysis provides evidence to support the use of TA as a treatment modality for patients with melasma. Further large-scale RCTs are warranted to identify the optimal dose and treatment schedule of TA (i.e. length of treatment, treatment interval, co-treatments).
This study was supported by a grant from the Korean Healthcare technology R&D project, Ministry of Health & Welfare, Republic of Korea (Grant No.: HN15C0105).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize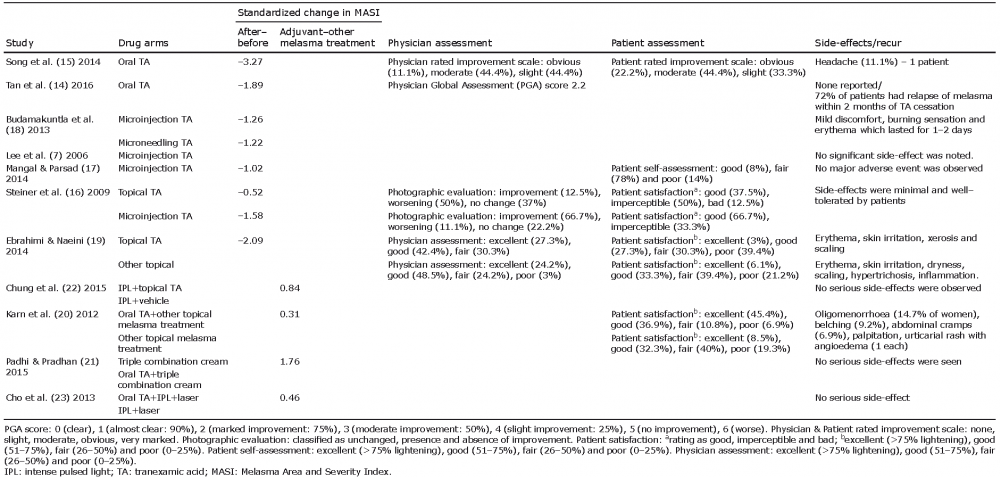 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize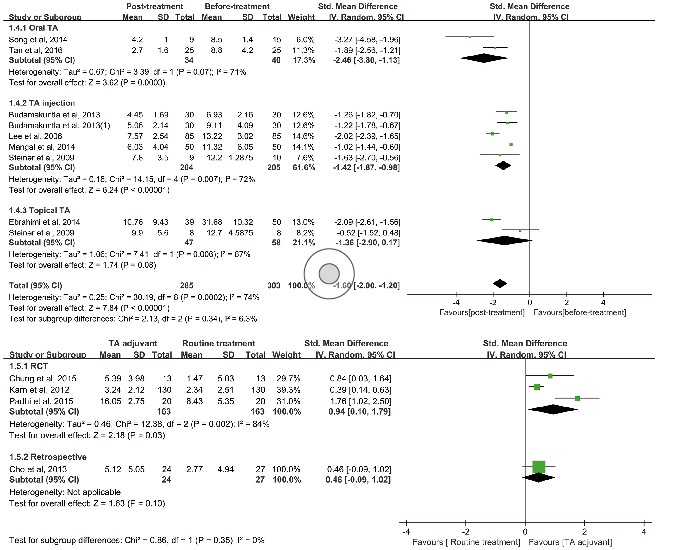 Click to show fullsize
Click to show fullsize