


1Department of Genetics, Institute of Genetics and Microbiology, University of Wroc?aw, 2Department of Dermatology, Venereology and Allergology, Wroc?aw Medical University, Wroc?aw, and 3Department of Applied Microbiology, Institute of Microbiology, University of Warsaw, I. Miecznikowa 1, PL-02-096 Warsaw, Poland. *E-mail: t.jagielski@biol.uw.edu.pl
The genus Arthrinium comprises an environmentally and biochemically diverse group of ascomycetous fungi, most of which display an endophytic lifestyle in a wide range of plant species. To date, only Arthrinium phaeospermum has been implicated in human disease, as a causative agent of superficial infections.
We describe here a case of subungual onychomycosis, due to A. arundinis. Treatment with itraconazole and amorolfine was successful in this case.
In January 2016 a 42-year-old man was examined in the Mycological Laboratory in the Department and Clinic of Dermatology, Venerology and Allergology, Wroc?aw Medical University, Wroc?aw, Poland. He presented with a typical distal and lateral subungual onychomycosis (DLSO) of the big toenail of the left foot. The nail plate was approximately 70–80% affected, with yellow-grey discoloration and advanced hyperkeratosis. The surface of the nail plate was neither eroded nor deformed. Only a single transverse nail ridge was observed on the border of the lunula, relating to anamnestic trauma. Here, the nail plate was thickened, separating the affected region from the healthy tissue. There was empty space between the nail plate and nail bed. The detachment of the nail plate from the periungual tissue was also visible, especially on the lateral side (Fig. 1A). Apart from insulin-dependent diabetes, the patient was in good general condition. Neither systemic disease nor any use of immunosuppressive drugs was evidenced in the patient’s history. Approximately 4 months earlier he had struck his foot on a piece of wood while walking barefoot along the shore of the Baltic Sea. A splinter entered deeply under the nail plate, and was removed immediately and nail was disinfected with octenidine hydrochloride solution (Octenisept®). After approximately one month the patient noticed a small wedge-shaped alteration on the nail. During the next 3 months, he intermittently used topical Scholl Fungal Nail Treatment®, with no effect. The lesion subsequently spread over approximately 75% of the nail plate.
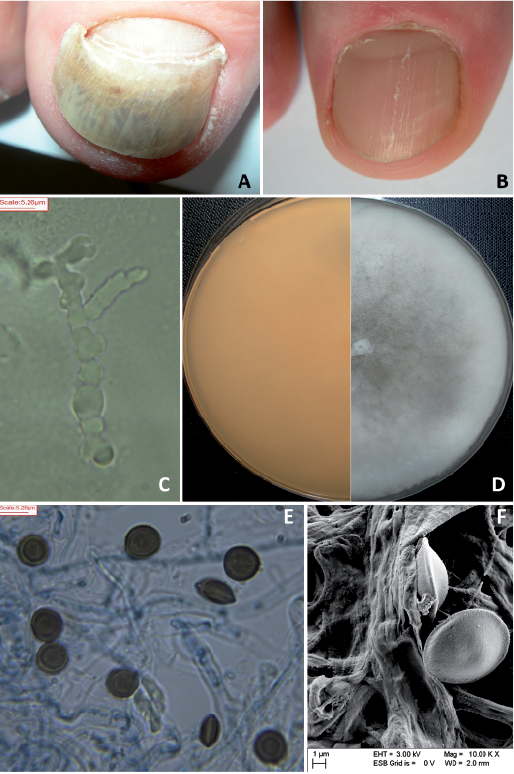
Fig. 1. (A) The big toe nail plate before treatment, and (B) after 3-month therapy with oral itraconazole and topical 5% amorolfine. (C) Hyphae of Arthrinium arundinis visualized by direct examination of nail scrapings after 10% KOH and dimethyl sulfoxide treatment (original magnification 1,000×). (D) Macroscopic appearance of A. arundinis culture on potato dextrose agar medium post 14-day incubation at 25°C. (E) Lactophenol cotton blue-stained slide culture showing the microscopic morphology of A. arundinis (original magnification 1,000×; scale bar 5.26 μm). (F) Scanning electron microscopy (SEM) of the fungus, (original magnification 10,000×; scale bar 1 μm).
Mycological examination was performed, followed by molecular speciation. A detailed, step-by-step diagnostic path was followed, as described in Appendix S1. The fungus isolated from the present case was identified as A. arundinis (Corda) Dyko & Sutton.
The cultured fungus (Fig. 1D) was subjected to drug susceptibility testing, with the Etest method (AB BIODISK, Solna, Sweden). Susceptibility assays were performed according to the Etest strip manufacturers’ instructions, with a 48-h incubation at 25°C (Appendix S1). In the absence of universally accepted guidelines specific for fungi, and especially Aspergillus, Arthrinium spp., interpretive criteria and quality control ranges for Aspergillus fumigatus, reported by the European Committee on Antimicrobial Susceptibility Testing were employed (1). The tested fungus was found to be resistant to fluconazole (32 μg/ml), anidulafungin (2 μg/ml), caspofungin (4 μg/ml); amphotericin B (2 μg/ml) and 5-fluorocytosine (> 32 μg/ml), but susceptible to itraconazole (0.125 μg/ml), voriconazole (0.25 μg/ml) and posaconazole (0.016 μg/ml).
Although terbinafine is commonly used for the treatment of onychomycosis, it was not considered in the present case, since no gradient strips are available for this drug, and thus its MIC value could not easily be established. Given the in vitro low MIC of itraconazole, its lipophilicity, high affinity for keratinizing tissues, and the high concentration that the drug reaches in the nails and maintains long after discontinuation of therapy (2), it was used to treat the present case. The drug was given to the patient at a dose of 200 mg orally twice a day for one week, according to the 3-pulse treatment scheme at 3-week intervals (3, 4). In addition, the patient applied topical 5% amorolfine nail lacquer once weekly, based on our previous experience with its effectiveness in treating toenail mould infections.
The treatment was continued for 3 months, during which time, both liver and kidney functions were monitored and showed no abnormalities. Results of physical examination were normal and blood tests were within normal limits. The 3-month treatment was fully successful, with complete clearance of the lesions and restoration of the natural appearance of the nail plate (Fig. 1B). The patient experienced no relapse during a 4-month follow-up period. Eradication of the infection was evidenced by negative direct microscopy and culture.
Fungi of the genus Arthrinium, described by Schmidt & Kunze in the early 19th century (5), belong to the family Apiosporaceae, which is named after Apiospora sexual morph described by Saccardo in 1875 (6). This family has only recently been placed in the class Sordariomycetes, which comprises a large group of filamentous ascomycete fungi of the Xylariales order and Pezizomycotina subphylum (7). To date, 32 species of Arthrinium fungi have been reported (8, 9). Many species lead a parasitic lifestyle, being facultative plant pathogens. One such pathogen is A. arundinis, which causes kernel blight in barley (10). Another example is A. sacchari, known as the aetiological agent of damping-off of wheat, and some other Arthrinium species live as endophytes in higher plants, lichens or marine algae (10). Fungi of the Arthrinium genus are generally not implicated in human or animal disease. To date, only one species, namely A. phaeospermum has been recognized, in 2 cases, as a cause of cutaneous infections in humans (11, 12).
To the best of our knowledge, the present case is the first to document human infection due to A. arundinis. Three findings strongly support the aetiological relationship be-tween the fungus and nail disease described here. Firstly, the mycological examination, always including KOH wet mount and culture, was performed thrice, on 3 independent samples (nail scrapings), and each sample produced fungal elements upon microscopic observations (Fig. 1C) and fungal growth in culture (Fig. 1D). Each time, the macro- and micromorphology of the isolated fungus was consistently the same (Fig. 1E, F), as were the results of molecular species identification performed on the first and 2 subsequent fungal isolates, based on an identical described earlier (13). Secondly, there was complete clinical resolution of the lesions following administration of antifungal treatment, according to the drug susceptibility profile of the isolated strain. Thirdly, the nail affection was preceded by a trauma to the toe by introducing a wooden splinter under the nail plate. It is likely that the trauma also led to development of Beau’s line (14), which was present only on the border of the lunula of the infected nail plate. It must also be noted that our patient was diabetic, which might have favoured the infection (15).
Since little clinical attention is paid to the Xylariales as potential aetiological agents of infection in humans, no consensus therapeutic strategy exists against this group of fungi. In this case, oral therapy with itraconazole supported by the local application of 5% amorolfine nail lacquer proved accurate and effective.
A search of the literature revealed only 2 cases of Arthrinium infections in men, both due to A. phaeospermum. The first was reported in a 25-year-old man from India, who presented with numerous erythematous nodules over the entire body, but mostly on his face (11). The patient was treated successfully with miconazole, administered topically for 30 days. Details of the second case, reported in Mandarin, are difficult to access (12). Based solely on the abstract, it appears that the patient experienced multiple subcutaneous nodules on his scalp and developed atrophic alopecia. The aetiological agent was A. phaeospermum, as evidenced by culturing the fungus from the lesions and clinical reproduction of the disease by intradermal inoculation of experimental animals.


 Click to show fullsize
Click to show fullsize