


1Inserm, U 1165, 2Université Paris Diderot, Sorbonne Paris Cité, Laboratoire de Pathologie, UMR-S 1165, 3Pathology Department, Hôpital Saint Louis APHP, 1 avenue Claude Vellefaux, FR-75010 Paris, 4Clinique Dermatologique, Université de Strasbourg, Hôpitaux universitaires de Strasbourg, Strasbourg, 5APHP, Hôpital Saint-Louis, Department of Dermatology, 6Université Paris Diderot, Sorbonne Paris Cité, and 7Inserm, U 976, Paris, France. *E-mail: maxime.battistella@aphp.fr
#These authors contributed equally.
Accepted Apr 18, 2017; Epub ahead of print Apr 19, 2017
Trichoblastoma is a predominantly dermal benign hair follicle tumour, characterized by well-circumscribed nests and cords of bland follicular basaloid cells in close association with stroma (1). Some cases of trichoblastic tumours with regular cytology contrasting with locally invasive growth have been reported with a wide variety of terms, such as “low-grade trichoblastic carcinomas” (2, 3), “unusually aggressive trichoblastoma” (4) or “plaque variant of trichoblastic fibromas”(5). All these cases appear similar, characterized by a large tumour size and poorly circumscribed subcutaneous and sometimes muscular infiltration. This type of locally aggressive trichoblastic tumours do not seem to recur if excised completely, but long-term follow-up is not well established (6, 7). In this work, we aimed to examine the clinicopathological features and follow-up data of locally aggressive and cytologically regular trichoblastic tumours, and to determine their malignant potential.
The archives of the Departments of Dermatopathology at Strasbourg Hospital and Paris Saint-Louis Hospital were searched for all cases of trichoblastic tumours with benign cytology (regular small nucleus, evenly distributed chromatin, small nucleolus, and regular nuclear membrane), infiltrative growth pattern and invasion of subcutaneous tissue or underlying structures, diagnosed between 1997 and 2014. Basaloid-cell tumours with cytological atypia, prominent peripheral palisading or prominent peritumoural retraction artefact were excluded. Among a total of 1,666 trichoblastic tumours diagnosed in the inclusion period, 36 cases met the inclusion criteria.
All formalin-fixed paraffin-embedded surgical specimens were stained with haematoxylin and eosin and reviewed blindly to follow-up data by 4 investigators with experience in dermatopatho-logy (CH, CV, BC, MB). When remaining tumour tissue was available, immunohistochemical staining for PHLDA1 (clone sc-23866, Santa Cruz Biotechnology; dilution 1/100) was performed on an automated Benchmark Ultra immunostainer (Ventana/Roche, Basel, Switzerland). Clinical data recorded included sex and age at the time of diagnosis, tumour location, tumour size, type of treatment, number of excisions to reach complete resection, tumour recurrence, and follow-up time. The main histopathological data recorded included presence of mitotic activity, presence of apoptosis, presence of tumour necrosis, depth of the tumour infiltration (subcutaneous tissue, muscular), connection to the epidermis, ulceration, and features of the stromal component.
Data for 36 patients were analysed. The clinicopathological features of the present study population are summarized in Table SI. The median age at diagnosis was 64 years (range 39–98 years), with male predominance (63.9%). Involved sites were most often the face (60%) followed by the trunk (20%) and the limbs (17.1%) (Fig. 1). The tumours had a median diameter of 23 mm (range 15–50 mm), and most often presented as smooth nodules. The 6 tumours with focal microscopic ulceration were not different in terms of size or location distribution, and large clinical ulceration was never present. First intention treatment consisted of surgical excision with 5–10-mm margins from the clinical tumour borders in all 36 cases. After the first excision, free margins were obtained in 5 cases, deep margin was involved in 26 (72%) and lateral margin in 19 (53%) cases. One patient with initial deep surgical margin involvement refused complementary surgery and received adjuvant radiotherapy (total dose 30 Gray). The median number of surgical excisions required for complete removal was 2 (range 1–5), with a median total excision margin of 10 mm. Five tumours required 3–5 surgical excisions to obtain free margins; most of which (4/5) involved the centrofacial area. Follow-up data were available for 20 (55.6%) patients, including 2 whose tumours showed perineural invasion. During a median follow-up of 64.2 months (range 10–120 months) after complete excision, there were no local or distant recurrences.
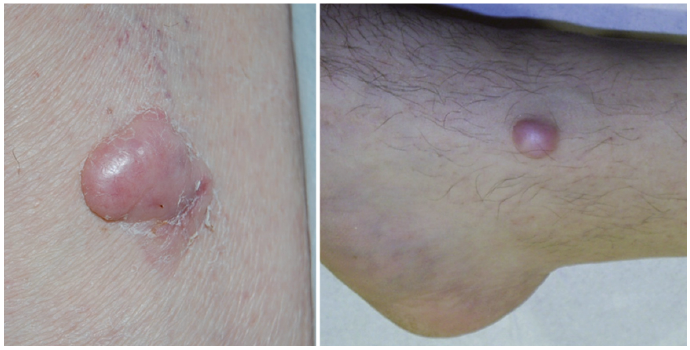
Fig. 1. Locally aggressive trichoblastic tumours on the leg of a woman (left) and a man (right).
Similar histopathological features were observed in all cases (Table SI). All neoplasms showed aggregations of basaloid cells with a variety of architectural patterns (Fig. S1). Perineural infiltration was found in 3 cases (8.3%), but not vascular invasion. Tumours reached the lower portion of the subcutaneous tissue in 36 cases (100%) and the skeletal muscle in 18 cases (50%) (Fig. S1c). All neoplasms showed a specific trichogenic-follicular stroma with the presence of papillary mesenchymal bodies (Fig. S1d). Cytologically all neoplasms displayed bland regular cells with ovoid, finely nucleolated, and fairly uniform nuclei (Fig. S1e). A cleft between stroma and adjacent connective tissue was rare and was observed in 5 cases (13.9%). No cleft was observed between tumour and stroma.
PHLDA1 expression could be studied in 17 cases. Sixteen tumours showed some degree of PHLDA1 expression (94%), with a diffuse pattern in 5 cases and a heterogeneous patchy pattern of expression in 11 (Fig. S2).
We present here a retrospective study of 36 cases of a peculiar category of trichoblastic tumours, with locally aggressive growth and benign cytomorphology.
The results show that this type of tumour exhibits a benign behaviour, and most often occurs in the cephalic extremity, the trunk or the limbs, mainly in adults over 60 years of age.
In the literature, 8 sporadic cases of trichoblastic tumours showing locally aggressive growth and regular benign cytology have been reported (Table SII). Some cases were interpreted as low-grade trichoblastic carcinoma (2, 3, 6), others as “a plaque variant of trichoblastoma” (5, 7), and the last as “unusually aggressive trichoblastoma” (4). Kazakov (8) also use the term low-grade trichoblastic carcinoma to describe such lesions. Our cases are clinically and microscopically similar to the 8 published cases. The strength of our study includes a larger sample size and a longer median follow-up of 64 months in the patients with available follow-up data.
Trichoblastomas and basal cell carcinoma (BCC) can sometimes be difficult to differentiate histologically on biopsy samples. Sellheyer et al. (9) showed that PHLDA1, a follicular stem cell marker, differentiated between desmoplastic trichoepithelioma (PHLDA1+) and morpheaform BCC (PHLDA1-), but showed variable staining in microcystic adnexal carcinoma. We also showed that PHLDA1 expression could help to differentiate trichoblastoma from BCC in tumours with clear-cell or granular-cell variants (10). Here, we showed that locally aggressive trichoblastic tumours almost always have some degree of PHLDA1 expression, a feature that may be useful to differentiate such tumours from BCC.
In the literature and in our study, all reported cases exhibited a benign behaviour after complete surgical excision or radiotherapy, with no evidence of distant metastasis or local recurrence. There is no consensus in the literature about the surgical management of trichoblastic tumours with locally aggressive growth. Complete excision with free surgical margins seems mandatory. From our data, we would recommend a 10 mm initial lateral margin from the palpable tumour, and an excision including the entire subcutis, until the first fascial plan as deep margin. Mohs micrographic surgery may also be an option, although this has not been reported to date.
Overall, this report describes the clinicopathological features of locally aggressive trichoblastic tumour/low-grade trichoblastic carcinoma, and shows that this category of tumours appears to have a good prognosis after complete removal, without local or distant recurrence. The naming of this type of tumour remains controversial. Although the cytology is benign and clinical behaviour after complete surgical removal also appears to be benign, the muscle-infiltrating invasive growth, perineural infiltration, and need for multiple resections to reach complete removal in some cases argue in favour of a low-grade carcinoma. Therefore, the designation of “low-grade trichoblastic carcinoma” seems best for this type of lesion.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize